Article Text

Abstract
Background: Because of concerns about harmful effects of 100% oxygen on newborn infants, air has started to be used for resuscitation in the delivery room.
Objective: To describe changes in preductal oxygen saturation (Spo2) and heart rate (HR) in the first 10 min after birth in very preterm infants initially resuscitated with 100% oxygen (OX100) or air (OX21).
Patients and methods: In July 2006, policy changed from using 100% oxygen to air. Observations of Spo2 and HR before and after the change were recorded whenever a member of the research team was available to attend the birth.
Results: There were 20 infants in the OX100 group and 106 in the OX21 group. In the OX100 group, Spo2 had risen to a median of 84% after 2 min and 94% by 5 min. In the OX21 group, median Spo2 was 31% at 2 min and 54% at 5 min. In the OX21 group, 92% received supplemental oxygen at a median of 5 min; the Spo2 rose to a median of 81% by 6 min. In the first 10 min after birth, 80% and 55% of infants in the OX100 and OX21 groups, respectively, had an Spo2 ⩾95%. Increases in HR over the first 10 min were very similar in the two groups.
Conclusions: Most very preterm infants received supplemental oxygen if air was used for the initial resuscitation. In these infants, the use of backup 100% oxygen and titration against Spo2 resulted in a similar course to “normal” term and preterm infants. Of the infants resuscitated with 100% oxygen, 80% had Spo2 ⩾95% during the first 10 min. The HR changes in the two groups were very similar.
Statistics from Altmetric.com
For many years, 100% oxygen was recommended for delivery room (DR) resuscitation of newborn infants of all gestational ages.1 In recent years, experts have suggested that even a brief exposure to high oxygen concentrations at birth in very-low-birthweight infants is harmful.2 There is also accumulating evidence of oxygen toxicity from animal and in vitro studies.3–5 Several studies have found evidence of oxidative damage in infants after short exposure to 100% oxygen in the DR.6–9 This evidence has led to a change in national guidelines for DR resuscitation, which now advise that 21% oxygen should be considered rather than 100% oxygen during initial resuscitation of all infants.10 11 Very preterm infants appear to be at greatest risk of oxidative damage.7 9 12 Data from infants born at <30 weeks’ gestation are limited.
The protocol for resuscitation of newborn infants at The Royal Women’s Hospital, Melbourne was changed in line with recommendations of the Australian Resuscitation Council.10 Before the change, 100% oxygen was used throughout resuscitation. After the change, air was used with 100% oxygen as a backup guided by ranges of oxygen saturations previously seen in term and preterm infants not requiring resuscitation.13 14 We aimed to describe the changes in oxygen saturation (Spo2) and heart rate (HR) of infants <30 weeks’ gestation resuscitated in the two eras.
What is already known on this topic
Brief exposure to supplemental oxygen in the delivery room can produce an Spo2 ⩾95%.
Preductal oximetry measures Spo2 and heart rate within 90 s of birth.
Using oximetry in the delivery room, clinicians can adjust the Fio2 to the Spo2.
What this study adds
When very preterm infants are initially resuscitated with air, some will require supplemental oxygen.
If very preterm infants are initially resuscitated with 100% oxygen, many will rapidly become hyperoxic.
Titrating oxygen administration may reduce the number of very preterm infants with Spo2 measurements ⩾95%.
PATIENTS AND METHODS
In this prospective observational study, the cohorts included infants <30 weeks’ gestation, born at The Royal Women’s Hospital, Melbourne between 12 January 2006 and 31 December 2007, when a member of the research team was available to attend the birth. This included 6 months before (OX100) and 18 months after (OX21) 17 July 2006, when the change in policy and implementation of the new guideline took place.
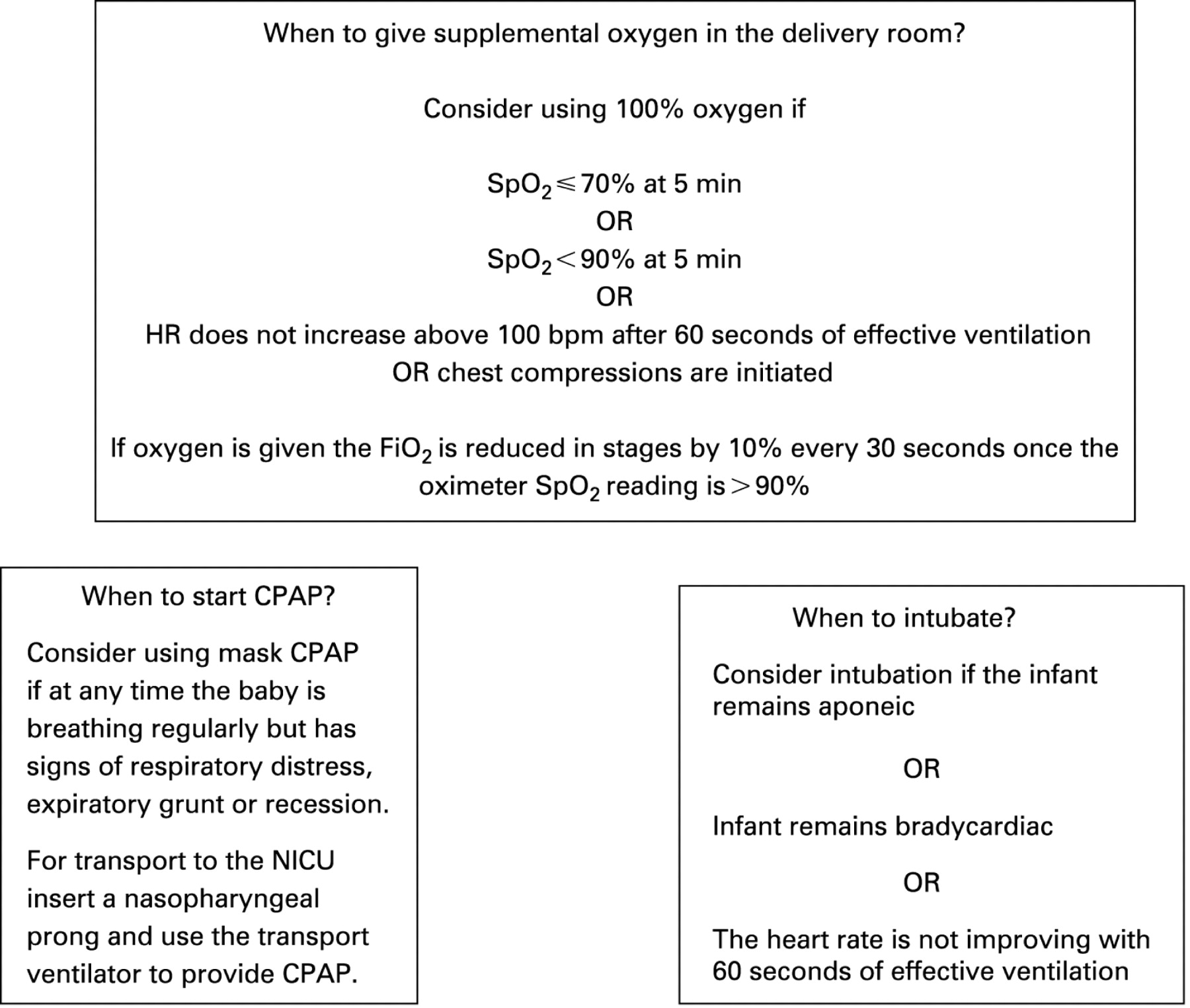
Immediately after birth, an oximetry sensor (LNOP Neo sensor; Masimo, Irvine, California, USA) was placed on the infant’s right hand and then connected to the oximeter (Radical7 V5; Masimo), as previously described.15 Spo2, HR and signal quality were stored by the oximeter every 2 s for at least the first 10 min after birth. We used 2 s averaging and maximum sensitivity. A member of the research team documented any interventions during resuscitation including adjustments made to the fractional inspired oxygen (Fio2). In the OX100 group, the Fio2 was not able to be changed because there was no gas blender available until infants were moved into a transport cot for transfer to the neonatal intensive care unit. Infants in the OX21 group were managed according to the 2006 Royal Women’s Hospital DR protocol with oxygen titrated according to Spo2 measurements (fig 1). If infants reached an Spo2 >90%, the Fio2 was reduced in stages of ∼10% to target the Spo2 to 80–90%. Active, spontaneously breathing infants, of any gestation, were started on continuous positive airway pressure (CPAP); infants requiring additional support were intubated and ventilated. This did not change over the time of this study. If free flow oxygen, CPAP or intermittent positive pressure ventilation were required, this was given with a Neopuff (Fisher & Paykel, Auckland, New Zealand) T-piece resuscitation device. In the second time period, a small number of infants were managed using a self-inflating resuscitation device (Laerdal, Stavanger, Norway).

After resuscitation, data from the oximeter (HR, Spo2 and signal quality) were downloaded to a computer using the NeO2m program16 (Dr Girvan Malcolm, Royal Prince Alfred Hospital, Sydney, Australia). The data were analysed with Stata (Intercooled 10). We only analysed measurements where the signal was considered normal, ie, no alarm messages (low IQ signal, low perfusion, sensor off, ambient light).
These observational data are presented to illustrate the effects on Spo2 and HR of resuscitation with either 100% oxygen or air with backup 100% oxygen if the Spo2 was <70% at 5 min. The data are presented as numbers and proportions (%) for categorical variables, or means (SD) for normally distributed continuous variables and median (interquartile range) when the distribution was skewed. Spo2 and HR during the first 10 min are illustrated by group using box plots showing the median, interquartile range (IQR) and range with outliers. We did not define primary or secondary outcomes a priori, therefore inferential statistics have not been used to compare these historical cohorts.
In the OX100 group, verbal consent was obtained from parents to monitor their infants in the DR. In the later group, parental consent was not obtained to monitor infants, as applying an oximeter sensor for monitoring in the DR was the standard of care for management of infants at “high risk” for receiving active resuscitation in our institution.
RESULTS
A total of 126 infants were studied. Pulse oximeter data were available for 125 infants (sensor failure in one infant in the OX21 group). All 20 infants in the OX100 group received 100% oxygen before 1 min of age. In the OX21 group, 97/105 (92%) were subsequently treated with supplemental oxygen at median (IQR) of 5.05 (4–5.5) min. Eight infants (8%) in the OX21 group did not receive supplemental oxygen in the DR. Tables 1 and 2 present the clinical characteristics and DR interventions, respectively. No infants received external cardiac massage.
Changes in oxygen saturation
Figure 2 shows the changes in Spo2 values for the two groups over the first 10 min. The median Spo2 at 1 min was 60% for the OX100 group and 55% for the OX21 group. By 2 min, the OX100 group had a median Spo2 of 84%, which continued to rise steadily to a median of 94% at 5 min and 96% by 10 min. For the OX21 group, the median Spo2 fell to 31% at 2 min, then rose to a median of 54% at 5 min, followed by a sharp rise to 81% at 6 min, after supplementary 100% oxygen was started, reaching a median Spo2 of 91% at 10 min. After 5 min, the median Spo2 was very similar in the two groups. In the first 10 min after birth, 80% and 55% of infants in the OX100 and OX21 groups, respectively, had an Spo2 ⩾95%.
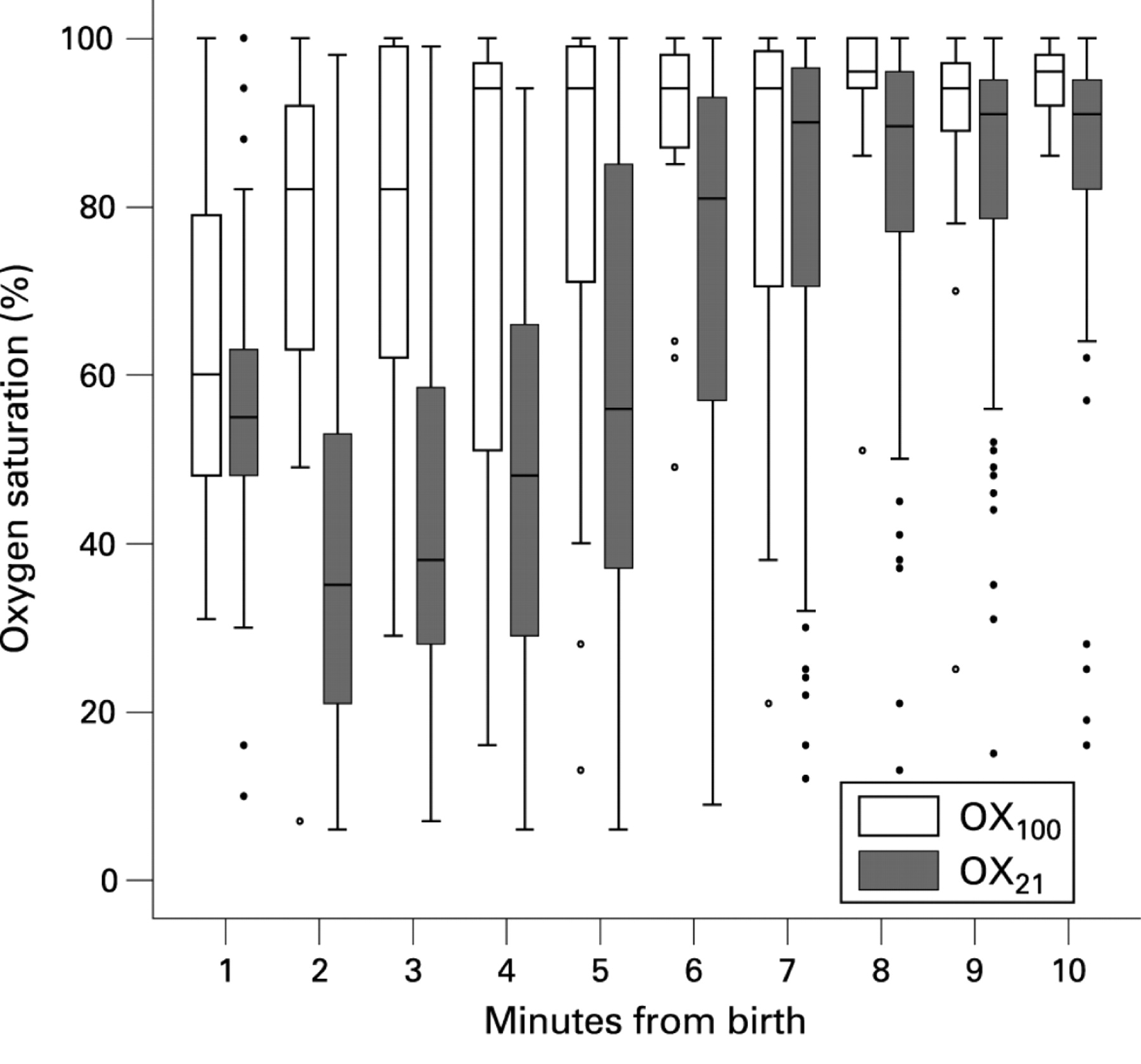
The eight infants not receiving supplemental oxygen were similar in gestation to infants in both the OX100 and OX21 groups, with a mean (SD) gestational age of 27.5 (1) weeks; however, they were slightly larger with a mean (SD) birth weight of 1044 (167) g. Six received CPAP and three received intermittent positive pressure ventilation via a face mask. The median Spo2 in these eight infants at 1, 2, 5 and 10 min was 60%, 71%, 87% and 93%, respectively.
Changes in HR
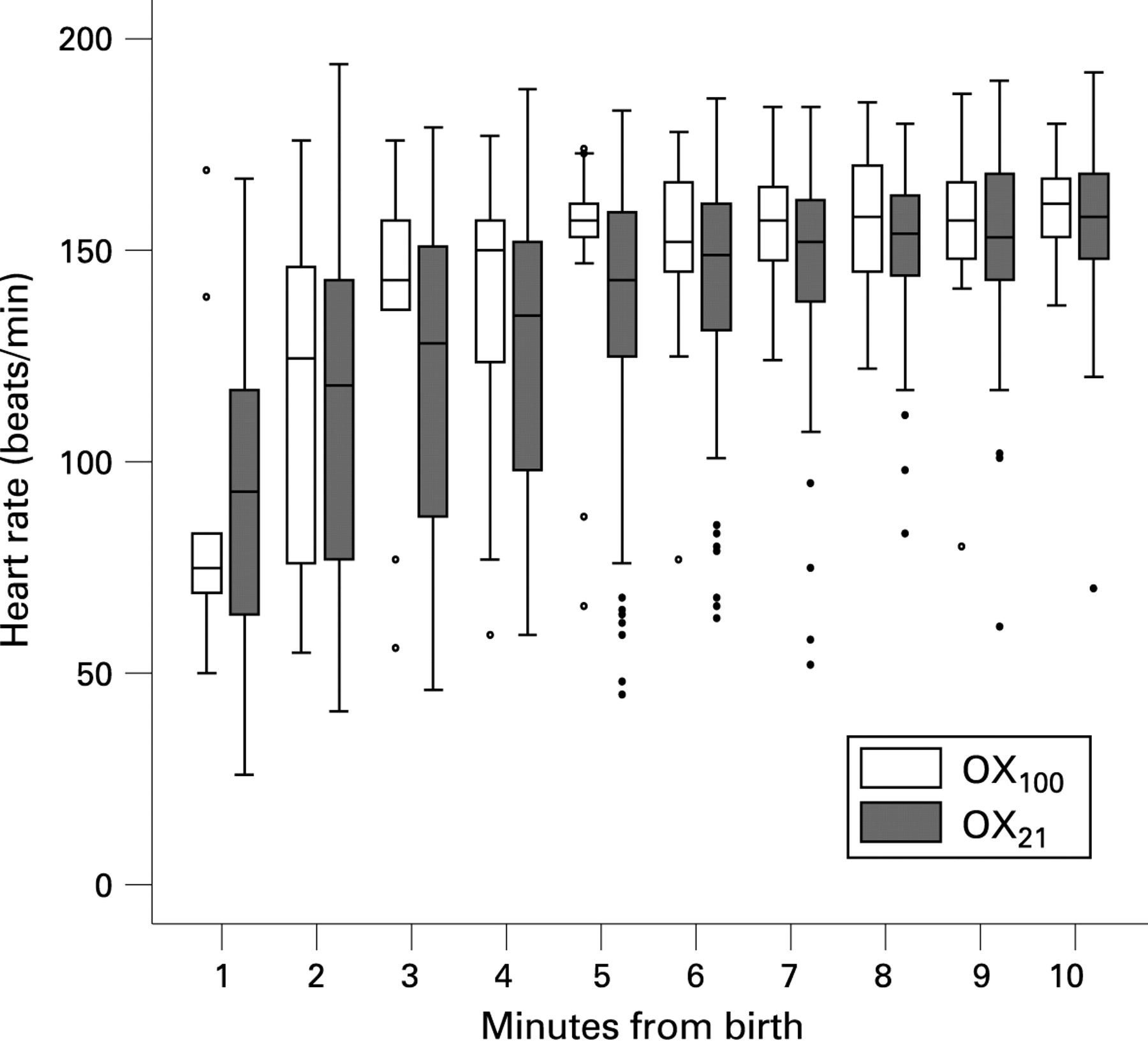
Figure 3 shows the changes in HR over the first 10 min. The median HR in both groups at 1 min was <100 beats/min: 76 beats/min (OX100 group) and 93 beats/min (OX21 group). In both groups, the median HR increased to over 100 beats/min by 2 min, over 140 beats/min by 5 min and over 150 beats/min at 10 min.
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
Pulse oximetry is increasingly used during neonatal resuscitation17 18 with some centres using it to target a specific Spo2 range.19 Several studies report Spo2 changes in term or near-term infants not requiring resuscitation in the first minutes after birth.13 14 20–22 Recent studies used pulse oximeters with algorithms that deal with low perfusion and motion artefact, both of which are common in the DR.13 14 20–22 These studies reported an Spo2 of ∼60% at 1 min, with many infants taking at least 10 min to achieve ⩾90%. Data from our very preterm infants initially resuscitated with air and backup 100% oxygen had a similar course. In our very preterm infants resuscitated with 100% oxygen, the Spo2 rose more quickly.
When the infants in our study were resuscitated initially with air, the Spo2 levels were at the lower end of the normal range for healthy term infants13 and rose into the “normal” range when they were treated with supplemental oxygen at about 5 min. By 6 min, their median Spo2 was 81%. By 7 min, there was little difference in the Spo2 between the OX21 group and the OX100 group. Fewer infants in the OX21 group had an Spo2 ⩾95% in the first 10 min than in the OX100 group.
A systematic review found that air was more effective than 100% oxygen for resuscitation of asphyxiated term infants.23 Spo2 data available for some infants in these trials24–26 show no significant difference in Spo2 measurements for infants randomised to receive air or 100% oxygen. However, few very preterm infants were enrolled in these studies.
Our hospital changed policy to starting resuscitation in air on the basis of evidence from randomised trials comparing initial DR resuscitation with 100% oxygen or air plus 100% oxygen as needed.8 9 26 When we developed our protocol, there were few data from randomised trials comparing 100% oxygen with an oxygen concentration other than 21% in preterm infants. Two studies had randomised infants to either <100% or >21% oxygen. Lundstrom et al27 randomised 70 infants <33 weeks’ gestation to receive air or 80% oxygen in the DR. They hypothesised that cerebral blood flow at 2 h of age might be reduced after a brief period of hyperoxia from 80% oxygen at birth. They found that the cerebral blood flow was significantly (p<0.0001) higher in the group treated with air. They also showed, in a subgroup of infants monitored with oximetry, that the mean Spo2 was significantly higher at 3, 5 and 7 min in the 80% oxygen group than the air group. In the air group, 74% did not receive supplemental oxygen. In those who received oxygen, the maximum was 50%. The reasons for the different oxygen requirements from those in our study are that the infants in the study of Lundstrom et al were more mature and clinical methods were used rather than Spo2 to titrate oxygen in the air group. We have shown that clinicians’ ability to measure colour28 or HR29 in the DR is weak. Harling et al30 randomised 63 infants <31 weeks’ gestation to either 50% or 100% oxygen in the DR. They hypothesised that cytokine concentration in bronchoalveolar lavage fluid 12 h after birth would be highest in infants treated with 100% oxygen, but found no significant difference. In infants randomised to receive 50% oxygen, one-third had an Fio2 above 50% during resuscitation. They did not measure Spo2 in the DR.
One approach to selecting the Fio2 to use in the DR is to use Spo2 measurements to adjust the Fio2.31 In the neonatal intensive care unit, targeting a narrow range for Spo2 and avoiding hyperoxia is associated with reduced morbidity in extremely-low-birthweight infants32 33 without a detrimental effect on developmental outcomes.32 It seems logical that a “targeted oxygen delivery approach”34 should be applied during resuscitation. A small observational study35 titrated Fio2 against targeted Spo2 in 15 infants born at 24–29 weeks. They were initially resuscitated with 100% oxygen and the Fio2 adjusted to maintain the Spo2 between 80% and 92%. The Fio2 was reduced from 100% to ∼40%.
There are now three controlled studies on very preterm infants where the Fio2 has been titrated to the Spo2 after birth. Escrig et al36 randomised 28 infants <29 weeks’ gestation to receive 30% or 90% oxygen. The Fio2 was adjusted to achieve an Spo2 of 85%. By 5 min, the Fio2 was just above 50%, with no significant difference between the groups. Wang et al34 randomised infants <32 weeks’ gestation to start resuscitation with 100% oxygen or air. In the 100% oxygen group, the Fio2 was weaned if the Spo2 was >95% at 5 min. In the air group, the Fio2 was increased in 25% steps if the Spo2 was <70% at 3 min or 85% at 5 min, or to 100% if the HR was <100 beats/min for 2 min or <60 beats/min for 30 s at any time. All infants in the air group received oxygen from ∼3 min. Infants in the 100% oxygen group had significantly higher Fio2 from 1 to 7 min, but from 8 to 20 min it was similar in the two groups. From 2 to 10 min, the Spo2 was higher in the group initially resuscitated with 100% oxygen.
In the only randomised study to mask clinicians to the Spo2, Rabi et al37 randomised 106 infants <33 weeks’ gestation to three groups. One received 100% oxygen throughout resuscitation, the second received an initial concentration of 100%, which could than be changed, and the third group started with air. In the last two groups, the Fio2 was changed by 20% every 15 s until the Spo2 was between 85% and 92%. The mean time that each group spent in the Spo2 target range was 11%, 21% and 16%, respectively (p<0.01). At the end of resuscitation, the Fio2 was similar in the two targeted groups.
The safe Spo2 range for very preterm infants during resuscitation is undefined. We targeted an Spo2 of 80–90%. Escrig et al36 targeted 85%, Wang et al34 targeted 80–85% at 5 min and 85–90% after 7 min, and Rabi et al37 targeted an Spo2 range of 85–92%. Each group used slightly different targets combined with different resuscitation protocols, which will have influenced the Fio2 used.
Hyperoxia is common during resuscitation of preterm infants. Tracy et al38 showed that, of 26 ventilated preterm infants of mean gestation 28 weeks (range 23–34), 38% were hyperoxic (Pao2 >100 mm Hg) 15 min after birth. Both Wang et al34 and our own study have shown that more of the infants who started in 100% oxygen had an Spo2 of >95% than those who started in air. Rabi et al37 reported that infants resuscitated in 100% oxygen spent 49% of the time above the Spo2 range of 85–92%. Therefore, in very preterm infants, hyperoxia appears to be a problem after starting resuscitation with a high Fio2 and indicates that starting with a lower Fio2 may be preferable.
Our results contribute to a growing body of evidence that it is possible to adjust the Fio2 to keep Spo2 measurements within a targeted range during resuscitation. 34 36 37 Our study shows that most of our very preterm infants received supplemental oxygen when the initial resuscitation was with air and their Spo2 was <70% at 5 min or <90% at 10 min. However, with different Spo2 targets, the use of supplemental oxygen would be different. We have shown that, using oximetry, it is possible to titrate the Fio2 to the Spo2, with the Spo2 rising at a similar rate to that in term infants not receiving assistance in the delivery room.13 14 21
When the initial resuscitation of very preterm infants has been started with >90% oxygen, it has generally been possible to reduce the Fio2 in response to the Spo2 to ∼ 50% at 5 min and 35% at 10 min. In comparison, when the initial resuscitation gas was air or a low Fio2, the Fio2 at 5 min was similar to when a high Fio2 was used. Therefore it now appears that, whatever the Fio2 used to initiate resuscitation, if the Spo2 is monitored within a few minutes an appropriate Fio2 is achieved.
HR is the most important indicator of an infant’s response to resuscitation.18 31 Using pulse oximetry in the DR provides clinicians with a continuous display of HR without having to interrupt resuscitation to listen to the HR intermittently. Importantly we found that the HR increased after birth at a similar rate in this group of very preterm infants, regardless of whether the infant was resuscitated with air or 100% oxygen. Our finding and those of other researchers34 36 have shown that, even with a low Spo2 during the first few minutes after birth, HR was similar to that achieved by healthy newborn term infants not receiving assistance.13 14 21
Two important questions cannot be answered by our study but could be addressed in future trials. Does pulse oximetry in the DR improve outcomes for preterm infants? If pulse oximetry is effective, what is the safe Spo2 range for preterm infants in the first minutes after birth?
Acknowledgments
JAD and COFK are recipients of a RWH Postgraduate Scholarship. ATP is the recipient of a Ter Meulen Fund grant for working visits, Royal Netherlands Academy of Arts and Sciences, The Netherlands, and PGD is the recipient of a NHMRC Practitioner Fellowship. The work was supported by Australian National Health and Medical Research Council Program Grant No 384100. We thank Dr Girvan Malcolm, Royal Prince Alfred Hospital, Sydney for his assistance with the NeO2M program.
REFERENCES
Footnotes
Competing interests: None.
Patient consent: Parental consent obtained.