Article Text

Abstract
Objectives: To examine whether clinically determined ventilator settings will produce acceptable arterial blood gas values on arrival, in preterm infants ventilated from delivery to the newborn intensive care unit (NICU). Further, to examine the usefulness of tidal volume and minute ventilation measurements at this time.
Design: A prospective observational cohort study in a tertiary level 3 NICU.
Patients: Twenty six preterm infants requiring intubation and mechanical ventilation at the point of delivery to the NICU.
Setting: Infants who required mechanical ventilation were monitored with a blinded Ventrak 1550 dynamic lung function monitor from the point of delivery to the NICU. A Dräger Babylog 2000 transport ventilator was set up to achieve adequate chest wall movement, and Fio2 was adjusted to achieve preductal Sao2 of 90–98%. Dynamic lung function monitoring data were recorded and related to the arterial blood gas taken on arrival.
Results: Mean gestation was 28 weeks (range 23–34) and mean birth weight was 1180 g (range 480–4200). A quarter (26% (95% confidence interval (CI) 12% to 48%)) were hypocarbic, with 20% (95% CI 7% to 39%) below 25 mm Hg, and 38% (95% CI 20% to 60%) had hyperoxia. Some (20% (95% CI 7% to 39%)) were both hypocarbic and hyperoxic. Total minute ventilation per kilogram correlated significantly with the inverse of Paco2 (p < 0.001).
Conclusions: Clinically determining appropriate mechanical ventilation settings from the point of delivery to the NICU is difficult, and inadvertent overventilation may be common. Severe hyperoxia can occur in spite of adjustment of the Fio2 concentration to achieve an Sao2 range of 90–98%. Limiting minute ventilation during resuscitation may prevent hypocarbia.
- hyperoxia
- hypocarbia
- minute ventilation
- resuscitation
- tidal volume
- NICU, newborn intensive care unit
- IPPV, intermittent positive pressure ventilation
- IVH, intraventricular haemorrhage
- RDS, respiratory distress syndrome
- Fio2, fractional inspired oxygen
- Pao2, arterial oxygen tension
- Paco2, arterial carbon dioxide tension
- Sao2, arterial oxygen saturation
- A-aDo2, alveolar-arterial oxygen tension difference
Statistics from Altmetric.com
- NICU, newborn intensive care unit
- IPPV, intermittent positive pressure ventilation
- IVH, intraventricular haemorrhage
- RDS, respiratory distress syndrome
- Fio2, fractional inspired oxygen
- Pao2, arterial oxygen tension
- Paco2, arterial carbon dioxide tension
- Sao2, arterial oxygen saturation
- A-aDo2, alveolar-arterial oxygen tension difference
Many preterm infants require assisted ventilation at birth for severe respiratory failure or apnoea. Little has been published on the adequacy of mechanical ventilation in these infants in the first 20 minutes of life, from the time of intubation in the delivery room until arrival in the newborn intensive care unit (NICU). After a clinical decision to intubate and ventilate, the infant may be hand bagged or placed on a mechanical ventilator with intermittent positive pressure ventilation (IPPV). Clinical estimates of the adequacy of mechanical ventilation are mostly limited to observation of chest wall movement, the interaction with the baby’s own respiratory efforts, and either colour or Sao2 monitoring where available. During transportation, the baby is often covered to help maintain thermoregulation, which reduces the ability to observe changes in chest wall movement.
Mechanical ventilation may cause excessive tidal volumes, which have been shown to injure healthy and surfactant deficient lungs, in both animal models and humans.1–6 Overventilation causing hypocarbia can induce alkalosis, worsen bronchopulmonary dysplasia,7 and reduce cardiac output 8. Hypocarbia has been associated with periventricular leucomalacia,9–12 hearing impairment,13,14 and cerebral palsy.13–15 Inadequate minute ventilation may cause hypercarbia, which has been linked to intraventricular haemorrhage (IVH) and acidosis.16 Hyperoxia at birth may increase the risks for bronchopulmonary dysplasia17,18 and may be associated with prolonged cerebral vasoconstriction,19 whereas severe hypoxia has known deleterious effects.16
Over recent years, more sophisticated measurements of lung function such as tidal volumes and minute ventilation have improved management of mechanical ventilation in the NICU. Commonly used techniques use either a pressure differential pneumotach or a hot wire anemometer. They may be integral to the mechanical ventilator as with the Dräger Babylog 8000 Plus or a separate device such as the Novametrix Ventrak 1550 (Novametrix Medical systems, Inc, Wallingford, CT, USA). It has previously been difficult to apply these techniques during transportation of these critically ill ventilated infants to the NICU. However, with increased portability of these devices, it has become feasible to introduce them into the delivery room, which allows objective measurements of ventilation in the first few minutes of the baby’s life.
The aims of this study were twofold: (a) to determine how successful clinical estimates of ventilator settings are in attaining normocarbia and normoxia on arrival of the baby in the NICU; (b) to assess whether the use of dynamic lung function monitoring during transportation from the delivery room could contribute to greater achievement of these blood gas targets.
METHODS
This was a prospective cohort study, carried out at the Nepean Hospital, a level 3 NICU in Sydney, Australia. Infants were enrolled from August 1998 to October 2001. Infants were eligible if they were < 35 weeks gestational age and required intubation and mechanical ventilation at the point of delivery. Ventilation was for severe respiratory distress not responding to continuous positive airway pressure, persistent cyanosis, or apnoea despite bag and mask ventilation in 100% oxygen. Infants were excluded if they had significant congenital anomalies or were thought to be at risk of pulmonary hypoplasia with prolonged rupture of membranes (> one week).
In addition to the resuscitating team, the chief investigator attended all deliveries to manage data collection with the Ventrak 1550 dynamic lung function monitor. Infants were intubated with the appropriate sized Portex endotracheal tube. The infant was stabilised and transported on a Dräger open care cot model RH600 modified as a dedicated newborn intensive care transport system. This included a Dräger Babylog 2000 transport IMV ventilator, Fisher&Paykel MR700 humidifier, Hewlett-Packard M1275A transport monitor with electrocardiograph and Sao2, and an uninterrupted power supply (UPS) battery. The Dräger Babylog 2000 transport ventilator has no respiratory monitoring and delivers intermittent mandatory ventilation through pressure limited, time cycled settings. The system has oxygen and air cylinders mounted at the back to provide blended fractional inspired oxygen (Fio2) concentration.
After intubation and tube stabilisation, the Ventrak 1550 single use precalibrated pneumotach (dead space 0.8 ml) was connected to the endotracheal tube and the Ventrak module. The Ventrak 1550 uses a pressure differential pneumotach, which has been shown in a comparative trial to have an absolute volume error of −0.1 (0.2) ml in the range 2–10 ml when compared with a known reference volume.20 The Ventrak 1550 was powered by a separate UPS battery. All measurements on the Ventrak 1550 were blinded during the study. The data were recorded continuously into a laptop computer until arrival in the neonatal unit and the baby was transferred to the NICU cot.
IPPV settings were started at 18/5 cm H2O, inspiratory time 0.3 seconds, and rate 60/min. These settings represent our unit consensus for the initiation of IPPV as a starting point only. The pulse oximeter was placed on the right hand to obtain preductal measures. The peak and end expiratory pressures were increased or decreased to achieve the minimal acceptable chest wall excursion and oxygenation. The ventilator rate was altered from a starting point of 60 to improve synchrony of the infant’s spontaneous breaths with the ventilator. Fio2 settings were adjusted to obtain arterial oxygen saturation (Sao2) in the range 90–98% (functional estimate). These adjustments occurred within two minutes of intubation and connection to the ventilator. After this stabilisation, the pressure and rate settings were not altered during the transport. The study protocol allowed the Fio2 to be adjusted during transport to maintain the Sao2 in the target range. On arrival in the NICU, an arterial blood gas sample was taken with the baby still on the transport cot and ventilator.
Hypocarbia was defined as arterial carbon dioxide tension (Paco2) < 4 kPa (30 mmHg), hypercarbia as Paco2 > 8 kPa (60 mm Hg), hypoxia as arterial oxygen tension (Pao2) < 6.7 kPa (50 mm Hg), and hyperoxia as Pao2 > 13.3 kPa (100 mm Hg). Respiratory distress syndrome (RDS) was defined as an infant with respiratory distress, typical chest radiograph, and the need for surfactant treatment. IVH was independently reported according to the Papile system.21
The study was approved by the research and ethics committee of the Wentworth Area Health Service.
ANALYSIS
The Ventrak for Windows program incorporates correction factors for changes in viscosity that occur with changes in Fio2,20 and automatically corrects for this. Dynamic lung function data were averaged from the time ventilator rate, and pressure settings were kept constant until the arterial blood gas was taken on arrival in the NICU. The averaged data were then related to the arterial blood gas result.
Statistical analysis was performed using Statistica 6.0 for Windows (StatSoft, Inc, Tulsa, OK, USA; http://www.statsoft.com).
Data collected are given as means (SD) unless indicated otherwise. Data were tested for normality using the Sharpiro-Wilk W test. Student’s t test was used for normally distributed data, Kruskal-Wallis test for non-normally distributed data, and Pearson’s χ2 test for proportions. It has been suggested that the χ2 test is appropriate to use even with small cell sizes.22 Confidence intervals for proportions were calculated using the exact, Clopper-Pearson method. Significance was taken as p < 0.05.
PATIENTS
Twenty six infants were studied, with a mean gestational age of 28 weeks (range 23–34) and a birth weight of 1184 g (range 480–4200). Four babies died from extreme prematurity, and two developed grade 3 IVH (table 1). No baby developed periventricular leucomalacia or a grade 4 IVH.
Details of babies studied
RESULTS
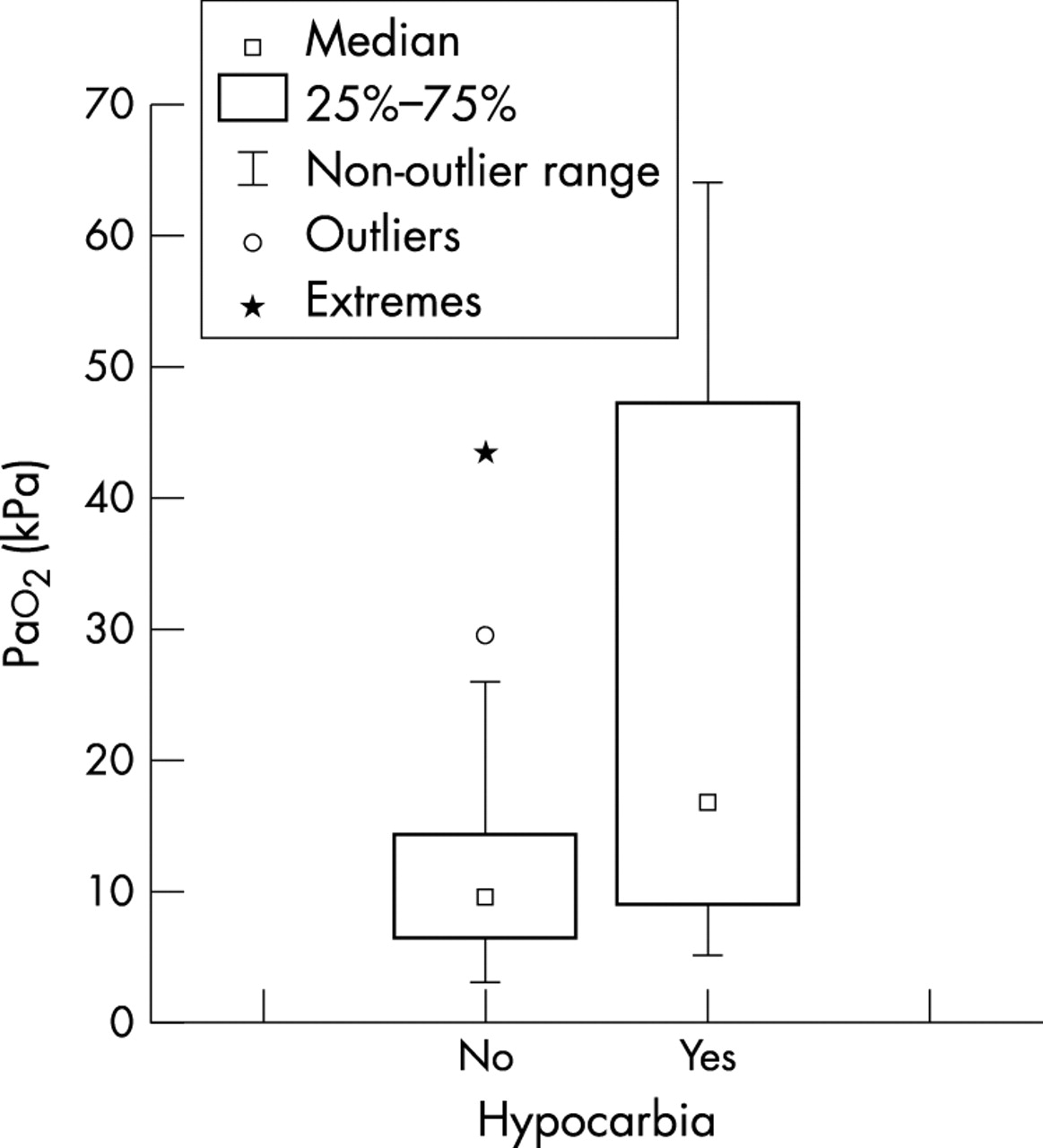
Seven babies were hypocarbic on arrival in the NICU, 19 were normocarbic, and none were hypercarbic. The hypocarbic group had a mean gestational age of 26 weeks and birth weight of 825 g compared with 29 weeks and 1315 g for those not hypocarbic (table 1). Four babies died, three were normocarbic and one hypocarbic. The groups did not differ significantly in the average duration of transport/resuscitation, Fio2, pH, Pao2, base excess, and A-aDo2 (table 2). A box plot of Pao2 grouped by hypocarbia shows the extreme values of hyperoxia in some patients, particularly those with hypocarbia (fig 1). Infants who were hypocarbic were significantly more likely to be hyperoxic also. Of the 10 hyperoxic infants, five were also hypocarbic, whereas of the 16 non-hyperoxic infants only two were hypocarbic (χ2 test; p = 0.04).
Comparison of blood gas and ventilator variables in hypocarbic infants and those not hypocarbic

Box plot of Pao2 against hypocarbia.
The hypocarbic infants had significantly higher PIP (25.0 cm H2O v 20.5 cm H2O; p = 0.005), PEEP (5.6 cm H2O v 4.6 cm H2O; p = 0.001), and MAP (11.9 cm H2O v 9.5 cm H2O; p = 0.02). There was no significant difference in respiratory rate.
As shown in table 2, the exhaled tidal volume per kilogram was not significantly different, with both groups having mean values of > 7 ml/kg. In contrast, the minute ventilation per kilogram was significantly different, with an average 627 ml/kg/min in the hypocarbic group compared with 402 ml/kg/min (p = 0.0002). Linear regression of Paco2 against total minute ventilation/kg reveals a highly significant relation (fig 2).

Linear regression of Paco2 against total minute ventilation. Paco2 = 8.002 − 0.007x. r2 = 0.68; r = –0.82; p < 0.0001.
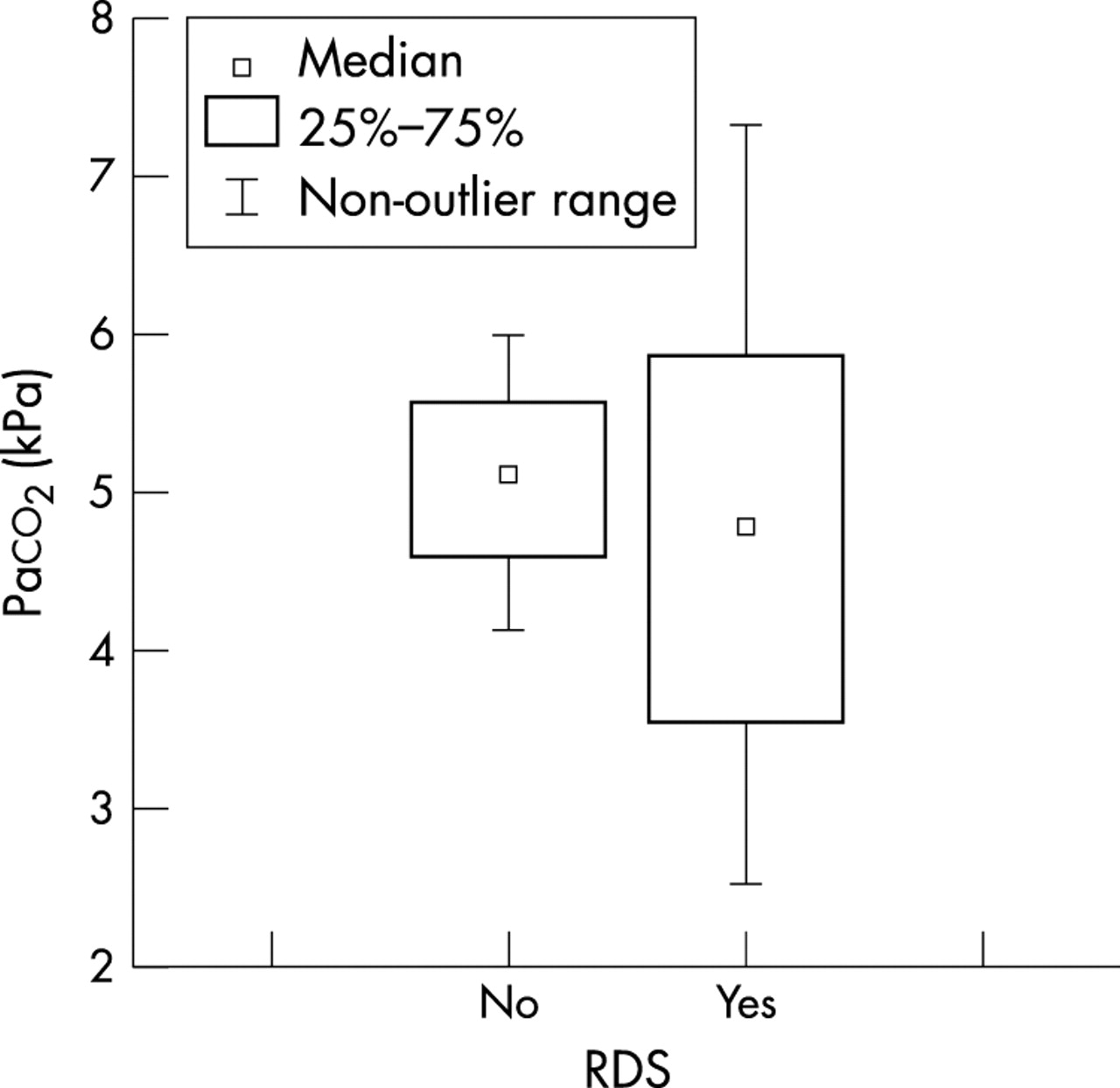
A box plot of Paco2 grouped by RDS shows that there is a wide range of Paco2 in the RDS group compared with those without RDS (fig 3), although this was not significant.

Box plot of Paco2 grouped by respiratory distress syndrome (RDS).
There was a trend to a significant difference with a higher arterial lactate 6.7 mmol/l in the hypocarbic group compared with 4.5 mmol/l in the normocarbic group (p = 0.07) (table 2).
DISCUSSION
We have shown that clinically determining mechanical ventilation settings in preterm infants intubated and ventilated from the point of delivery to the NICU is not adequate in preventing inadvertent overventilation and hypocarbia. The initial ventilator settings of pressures of 18/5 cm H2O and rate of 60 used in our study are lower than most current neonatal textbooks recommend, with peak pressures of 20–30 cm H2O.23–26 Our results (fig 2) suggest that measuring and limiting the total minute ventilation per kg to < 460 ml/kg/min may prevent this overventilation.
Further, significant and severe hyperoxia was common in our study (fig 1) even when targeting preductal Sao2 values of 90–98% by altering the Fio2. We found that some infants had decreasing Sao2 with good pulse oximeter trace during the transfer to the unit. As a consequence, the Fio2 was increased during the transport to achieve the target range, and we found that some infants had overshot Sao2 to > 98% on arrival. Targeting a lower saturation range (86–92%) and having a higher threshold for altering the Fio2 during movement may reduce the incidence and severity of hyperoxia.
We are not aware of similar studies that have investigated the clinical utility of dynamic lung function measurements from the delivery suite. Our transport ventilation system allows accurate delivery of IPPV with humidified fractional oxygen. We feel this provides a more controlled system than hand bagging with an endotracheal tube. Upton and Milner27 studied 30 asphyxiated newborn infants, of whom 22 were preterm. When an anaesthetic bag with no pressure limitation was used, tidal volumes rose from 8.7 ml/kg early in the resuscitation compared with 9.7 ml/kg later in the resuscitation. Pressures generated were a median maximum of 50 cm H2O (range 33–73). Tidal volumes as measured in our study were similarly high with much lower pressures. Clinical estimates of ventilator settings did not produce average tidal volumes < 7 ml/kg, which may promote lung injury.4
All infants who did not have RDS had Paco2 values in the acceptable range (fig 3). Those with RDS had a wide range of Paco2 values, with 32% being hypocarbic (95% CI 14% to 55%). RDS is a disease of variable severity, and, although we detected no differences in the duration of resuscitation between those with RDS and those without, it is possible that differences in functional residual capacity and compliance may explain the observed incidence of hypocarbia in the RDS group.
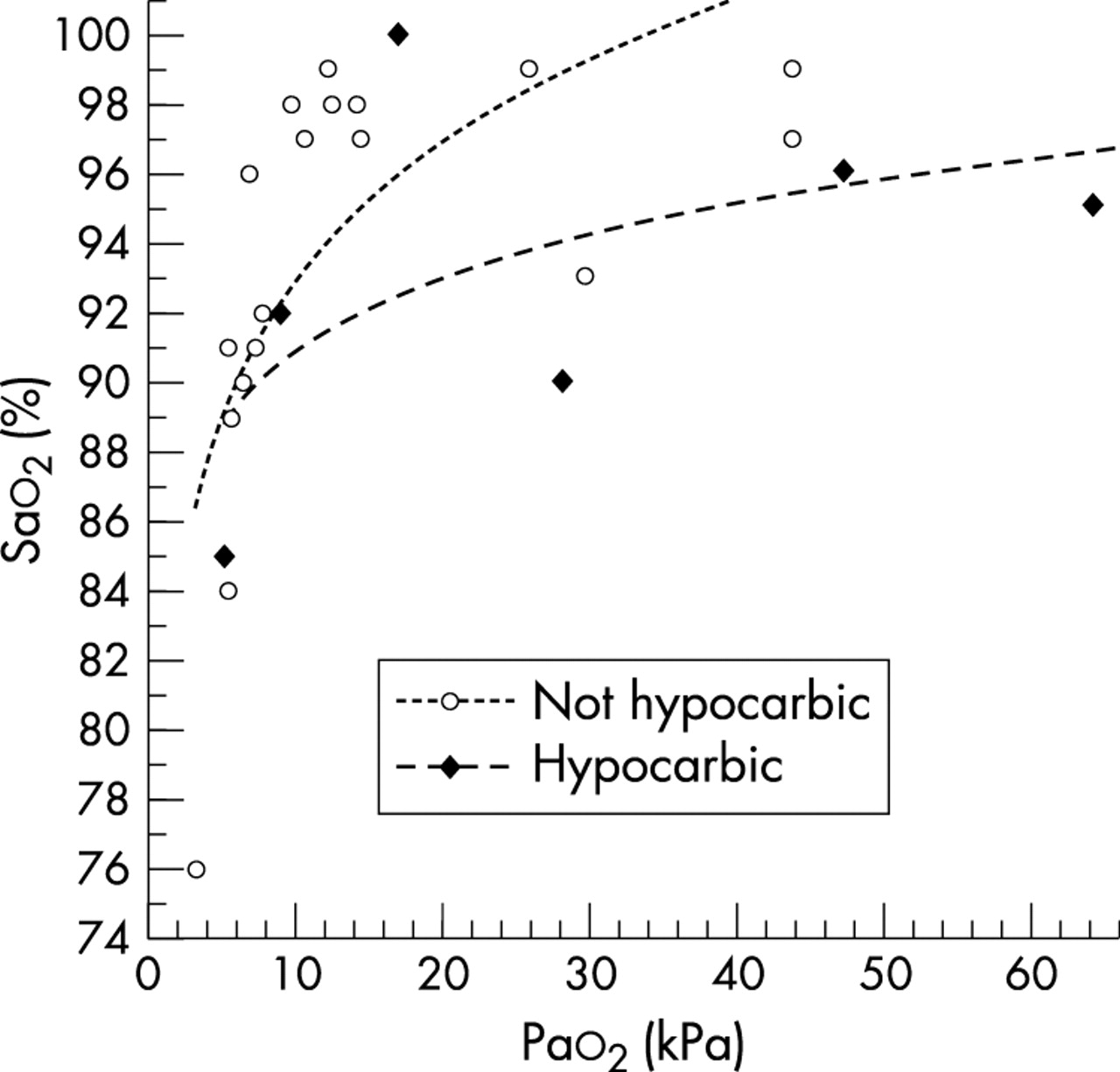
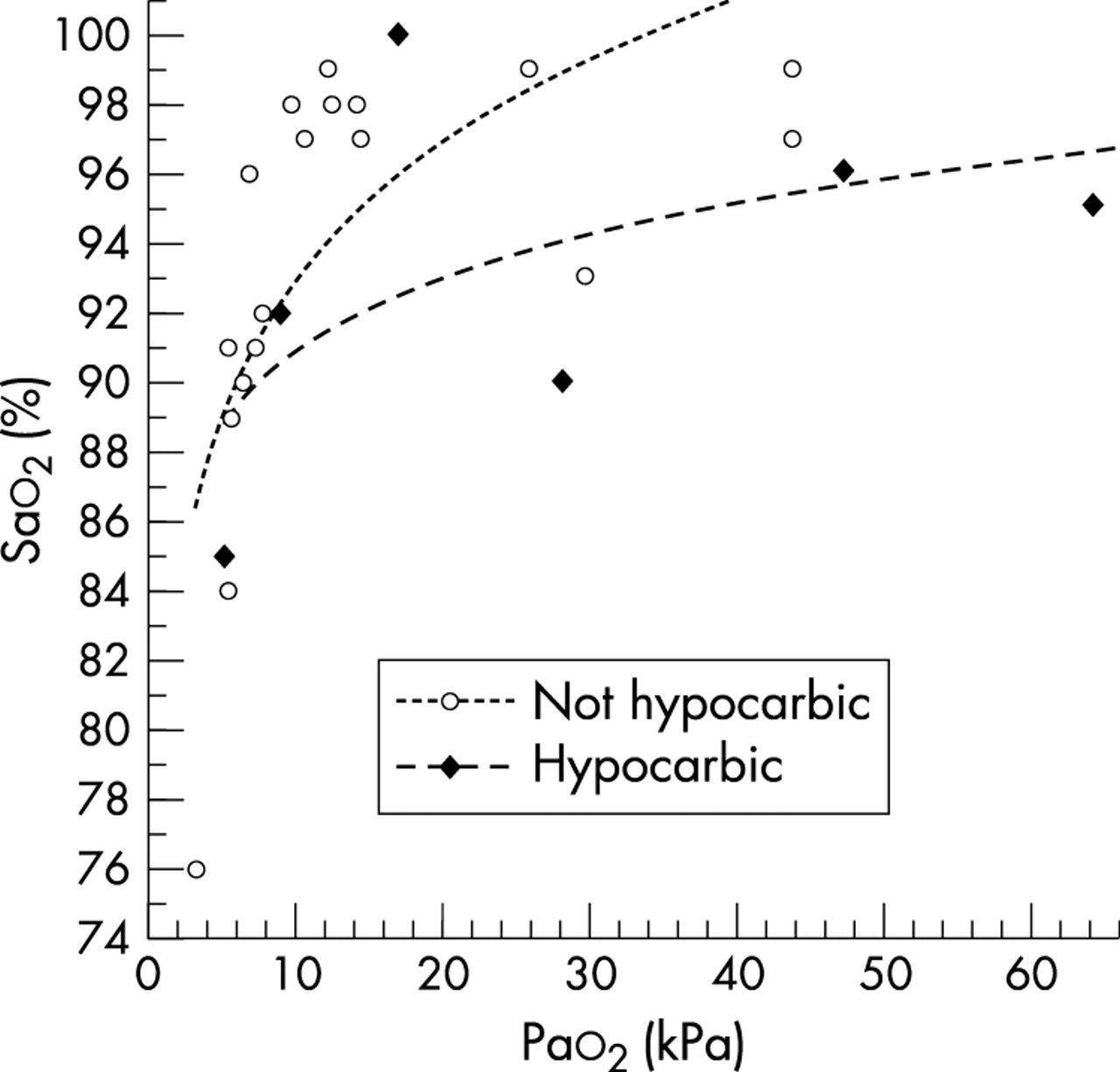
The pulse oximetry was particularly inaccurate in those infants with hypocarbia (fig 4). It is possible that overventilation, particularly in the hypocarbic group, may have reduced cardiac output and hence peripheral perfusion, which may have contributed to underreading of the oxygen saturation monitor.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Scatterplot of Sao2 by Pao2.
The limitations of our study are the small sample size and a possible selection bias resulting in some preterm infants not being studied because of the advance notice required to assemble the research team for all resuscitations. However, we believe that these observations are concerning and require further investigation.
Recent reviews on the pathogenesis of brain injury in ill preterm infants highlight the importance of cerebral autoregulation as a protective mechanism.28 Brief, inadvertent overventilation with excessive tidal volumes may cause a number of unwanted adverse effects, which, when combined with hyperoxia, may pose heightened risks to a critically ill newborn infant with impaired cerebral autoregulation.
In view of this, we are planning a larger randomised controlled trial targeting both tidal volume per kilogram at 5–7 ml/kg and minute ventilation per kilogram < 460 ml/kg/min in the treatment arm. Also, the ILCOR guidelines currently recommend the use of 100% Fio2 for the resuscitation of premature infants.29 Data from our study suggest that this strategy may result in common and extreme hyperoxia in the first 20–30 minutes of life. Consequently, in our planned randomised controlled trial, we also intend to lower the target Sao2 range to 86–92% to reduce the incidence and severity of hyperoxia.