Article Text

Abstract
Objective: To assess the effect of routine measurement of postductal oxygen saturation as an adjunct to routine clinical examination in the asymptomatic newborn.
Design and setting: Prospective study in a district general hospital.
Patients: All 6166 infants inborn between 1 April 1999 and 31 March 2001.
Intervention: Oxygen saturation was measured over two minutes, after the age of 2 hours and before discharge, in one foot of all babies not admitted directly to the neonatal unit. Babies with fractional (as opposed to functional) oxygen saturation (Sao2) below 95% were examined by the midwife. If this examination was abnormal or if normal but further measurements were below 95%, an echocardiogram was performed. All babies with cardiac malformations diagnosed by 1 year of age were identified from databases maintained at the regional cardiology referral unit and the regional congenital malformation survey.
Results: Measurements were made in 98% of eligible babies. A fractional Sao2 less than 95% was found in 5% but persisted in only 1%. Structural cardiac malformations were found in 50 (8.1/1000), 26 of whom had isolated ventricular septal defects. Of the remaining 24 with other cardiac malformations, attention was first drawn to six by low Sao2, and four more, first noticed for other reasons, also had low Sao2. Low Sao2 also first drew attention to 13 other babies ill for other reasons.
Conclusion: Newborn babies with important cardiac malformations are often asymptomatic initially and the yield from clinical examination is poor. Measuring postductal saturation routinely in newborn babies before discharge is easy and can alert staff to ill babies.
- screening
- congenital heart disease
- cardiac malformations
- oxygen saturation
Statistics from Altmetric.com
Even though “a thorough physical examination of every neonate is now universally accepted as good practice”,1 it is apparent that an appreciable proportion of babies with congenital cardiac malformations are not detected by this routine examination as currently performed.2–5 The most likely reason is not that the examination is poorly performed, although this may be the case at times, but that many babies with congenital cardiac malformations have no signs that can be detected by clinical examination. For example, babies with an isolated interruption of the aortic arch may have no murmur and, while the ductus remains patent, would have normal femoral pulses. They would therefore be likely to pass a routine examination only to become rapidly and severely unwell within a few days as the duct closes.2,3,5 Most early deaths due to undiagnosed heart malformations occur in babies with obstructions of the left ventricular outflow tract,2 all of whom are likely to have appreciable right to left ductal flow at some stage.
If the diagnosis in these babies is being missed because they have no clinically detectable physical signs, it becomes clear that a different strategy should be used to detect them. We therefore decided to measure postductal oxygen saturation routinely in all babies before discharge home in order to identify those babies with measurable but clinically undetectable hypoxaemia. We hoped that this would facilitate early detection of cyanotic congenital heart disease but also realised that it may draw attention to babies ill for other reasons. This paper reports the effect of this policy in one hospital over a two year period.
METHODS
From 1 April 1999 all babies born in Sunderland Royal Hospital, unless admitted directly to the neonatal unit at birth, had oxygen saturation measured over two minutes by pulse oximetry in one or other foot by a midwife after the age of 2 hours and before discharge home. Midwifery staff were asked to note the highest and lowest stable readings measured when the baby was settled. Any baby whose postductal fractional saturation while breathing air did not reach 95% was brought to medical attention. Initially, we did not know how many such babies would be identified and we also did not know to what extent, if any, such a measurement was abnormal. After a period during which echocardiograms were performed on all such babies the following policy was adopted.
Any baby who did not achieve a postductal fractional saturation of at least 95% was clinically examined by the midwife. If no suspicions were raised by the examination, a second saturation measurement was performed an hour or two later. If either the examination or the repeat saturation measurement were not satisfactory, an echocardiogram was performed. It is already routine in this hospital for babies in whom a murmur is heard on examination in the newborn period to have an echocardiogram performed either before initial discharge home or within 48 hours of discharge.
Saturation was measured using a Radiometer Oxi machine which displays fractional oxygen saturation. Two algorithms are used by manufacturers of pulse oximeters. One displays fractional oxygen saturation6
(HbO2/(HbO2 + reduced Hb + MetHb + COHb)) × 100 whereas the other displays functional oxygen saturation (HbO2/(HbO2 + reduced Hb)) × 100.
Fractional oxygen saturation is about 2% less than functional saturation.
All babies with suspected heart disease in the northern part of the Northern and Yorkshire region are referred to a single paediatric cardiology centre at Freeman Hospital. Any baby born within this area who is found to have a structural cardiac malformation confirmed by echocardiography or autopsy is reported to both the diagnostic database at Freeman Hospital7 and that maintained by the Northern Congenital Abnormality Survey.8 Any baby born within the area and dying in the first year of life will also be reported to the Regional Perinatal Mortality Survey.9 These three databases were interrogated in March 2002 to identify all cases of congenital cardiac malformation among babies liveborn in Sunderland Royal Hospital from 1 April 1999. The study was approved by the Sunderland local research ethics committee.
RESULTS
Between 1 April 1999 and 31 March 2001, there were 6166 livebirths at Sunderland Royal Hospital, 447 (7.2%) of whom were admitted direct to the neonatal unit from the labour ward and were thus not eligible for routine measurement. Parents did not give consent for five babies to have measurements, and in 88 babies (1.5% of those eligible) the opportunity to make a measurement was missed.
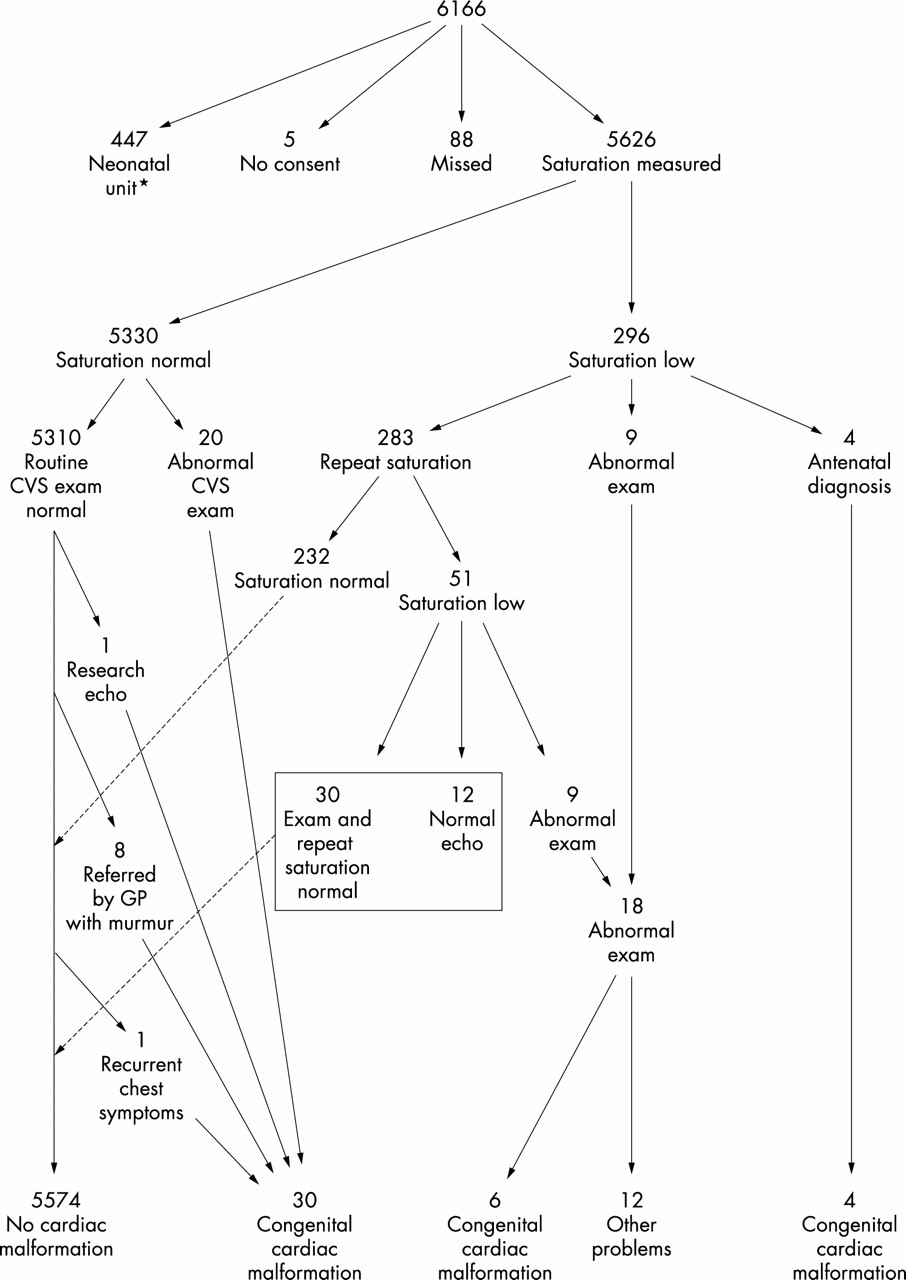
A postductal fractional saturation of less than 95% was found in 296 (5.2%) of the 5626 babies in whom measurements were taken. In four of these babies, an antenatal scan had already identified a cardiac malformation, and in a further nine, clinical examination raised concerns. The remaining 282 mostly underwent a second measurement after an interval, although a few had an echocardiogram instead. In 51 babies (0.9% of those originally measured) a second measurement was also less than 95%. All 51 were then clinically examined and concerns were raised in nine. Of the remaining 42, 12 had normal echocardiograms and 30 achieved a postductal fractional saturation of at least 95% on a third measurement. Figure 1 shows the routes by which the babies were identified.

Flow chart showing how the babies with low saturation and those with congenital cardiac malformation were processed. CVS exam means clinical examination of the cardiovascular system, and exam means clinical examination including CVS examination. *An additional 10 babies with congenital cardiac malformation were also identified among babies who were either preterm (less than 35 weeks gestation) or dysmorphic.
Table 1 shows the problems and initial saturations of the 18 babies brought to clinical attention by routine measurement of postductal saturation. Attention was drawn to one further baby by the fact that, although the highest stable saturation was greater than 95%, low levels of 70% were also seen. This baby had a normal echocardiogram, but a cerebral ultrasound scan showed a midline shift with haemorrhage into an arachnoid cyst which required surgical drainage. The intermittent low saturation was possibly related to subclinical fits. This baby later developed fits before surgery.
Diagnoses and age at identification in 19 babies first identified as unwell by routine measurement of postductal fractional saturation
In four babies, an antenatal scan had showed a severe cardiac malformation. These four had postductal saturation measured in the same way as the routine measurements to find out if we would have been alerted to the problem had the antenatal diagnosis not been made. Their diagnoses were simple transposition, complex transposition, complex pulmonary atresia, and coarctation of the aorta with ventricular septal defect (VSD) (fig 2). In all four the “routine” saturation measurement was less than 95%.

{kind=link}
{kind=link}
Flow chart showing the signs exhibited in the first days of life in the 50 cases of congenital cardiac malformation. The letters A, B, C, D next to those cases listed in the dysmorphic and preterm groups indicate which other group (low saturation with no murmur etc) they would have been in had attention not already been drawn to them by their dysmorphism or preterm status. Babies are classed as having a murmur if a murmur was detected before discharge home or in the first week of life in babies discharged after 7 days of age. ASD, Atrial septal defect; VSD, ventricular septal defect; TGA, transposition of the great arteries. * denotes antenatal diagnosis.
Cardiac malformations
During the study period 50 babies born in Sunderland were found to have a structural cardiac malformation (8.1 per thousand).
Isolated VSDs
There were 26 babies with isolated VSD, of which two were also dysmorphic (anal atresia, trichorhinophalangeal syndrome) and three were significantly preterm (29, 32, and 33 weeks). Of these five, four were detected before discharge. In two of the three preterm infants, the diagnosis was made once a murmur was heard during their stay. In the third preterm baby, the diagnosis was made when a systolic murmur was heard on readmission with late onset Group B streptococcal meningitis after initial discharge home. In the two dysmorphic babies, scans were performed because of their dysmorphism, although one also had a low postductal saturation. Of the remaining 21, 15 were identified in the newborn period because of a murmur (all saturations normal), one with normal saturation and no murmur was discovered incidentally while being scanned for a research project, and five were referred back by their general practitioners with a murmur at ages varying from six weeks to four months. In these five cases, no murmur was noted in the newborn period and saturations were recorded as normal.
Three babies required surgical closure of their VSD during the first year of life; all were detected before discharge home. One baby, who was referred by the general practitioner with a murmur at four months, was thought to require surgery for a subaortic VSD at 22 months.
Cardiac malformations other than isolated VSD
There were 24 babies with structural heart disease, other than isolated ventricular septal defect, three of which were also dysmorphic (cleft lip and palate, Apert’s syndrome, and CHARGE association (colobama, heart defects, atresia of choanae, retarded growth, genital hypoplasia, and ear anomalies)). Three, including one of these dysmorphic babies, were significantly preterm (33, 33, and 30 weeks).
In 10 babies the postductal fractional saturation was found to be below 95%. They included three with transposition of the great arteries, two with coarctation and VSD, two with Fallot’s tetralogy (one at 33 weeks gestation), two with pulmonary atresia (one with a VSD and one with an intact ventricular septum), and one with a persistent ductus arteriosus (closed surgically at 9 months).
Only four of these 24 babies were not diagnosed before initial discharge home; one with pulmonary valve stenosis was referred by her general practitioner with a murmur at six weeks, another with a secundum atrial septal defect was referred by his general practitioner with a murmur at 10 months, a third with anomalous origin of the left coronary artery from the main pulmonary artery presented with recurrent chest symptoms and mitral regurgitation at 9 months, and a fourth with anomalous origin of the right pulmonary artery from the aorta was referred by her general practitioner with failure to thrive at 10 months. This last baby had an initial saturation measurement of 92% at 7 hours of age, but a repeat measurement at 9 hours was 96% and no murmur was heard on examination. She was therefore discharged home without further investigation. The other three had normal saturations on first measurement and no murmurs on examination in the newborn period.
Age at measurement
For the first 4230 babies measured, we have data on the age of measurement and saturation on all babies, whatever saturation was recorded. Data from these babies gave a mean (SE) value for postductal fractional saturation of 98.04 (0.032)%. The mean age at measurement was 11.7 hours. In those measured before 24 hours of age, the proportion of first measurements below 95% was 4.7% (95% confidence interval (CI) 4.04 to 5.40), whereas in those measured after 24 hours it was only 2.8% (95% CI 1.42 to 5.02). Although this would suggest a tendency to higher measurements in the second day of life, with the small number measured after 24 hours of age in our sample, this difference does not reach statistical significance.
Cot deaths
There were six cot deaths in the first year of life among the 6166 births. They were born at 34, 36, 38, 38, 39, and 39 weeks gestation and died at 17, 28, 12, 10, 44, and 7 weeks of age respectively. All had had saturation measurements performed and all had recorded levels of 95% or more on the first measurement.
DISCUSSION
In our experience, about 5% of babies not admitted directly to the neonatal unit have an initial postductal fractional saturation of less than 95%, but this only persists in 1%. Our study also shows that routine measurement of postductal fractional saturation can result in timely recognition not only of cyanotic congenital heart disease but also other serious illness (table 1). This may be particularly relevant for babies with “persistent pulmonary hypertension of the newborn” who may require considerably more treatment if recognition were delayed until the baby was clinically cyanosed. A similar argument can be made with respect to transposition of the great arteries, where early diagnosis is known to improve prognosis.10
Examination of fig 2 may suggest that saturation measurement was only necessary for the diagnosis of three children with congenital heart disease—those in group D—in whom there was no clinical sign other than a low saturation to prompt recognition. Furthermore, antenatal diagnosis had already identified one of these. However, the four cases in group C who were not antenatally diagnosed had attention drawn to them within hours of birth by a low saturation measurement and only then was a murmur listened for and detected. Had the antenatal diagnosis not been made in the remaining two cases in group C, then a saturation measurement would have triggered investigation within hours of birth. Similarly, two of the dysmorphic cases had attention drawn to the possibility of an additional cardiac problem by saturation measurement. It should also be remembered that most hospitals are not able to offer echocardiography to babies with murmurs before discharge. If an echocardiogram is not immediately available, then the noting of a low saturation in addition to a murmur would almost certainly lead to an urgent rather than a routine referral for a cardiological opinion.
It has been previously reported that left heart obstructive lesions are the most likely to result in death before diagnosis.2 It is disappointing to see that, of the six babies with coarctation in this report, only three had an early low saturation. A case of coarctation figures in each of the four groups (A–D) in fig 2. Others have had similar experience with coarctation.11,12
Of the nine babies with congenital cardiac malformations discharged home undiagnosed (all but one of group A in fig 2), none would have had appreciable right to left shunting in the newborn period. Furthermore they were neither dysmorphic nor preterm and none had murmurs noted on routine examination.
The use of routine measurement of oxygen saturation in an attempt to detect respiratory or cardiac problems in newborn babies was probably first suggested by Katzman in 199513 in response to an article reviewing technical and other aspects of oximetry.6 The obstacles to this suggestion were highlighted by the authors of the original article in their reply.14 These obstacles were principally related to the two differing measurements displayed by pulse oximeters of different makes, namely fractional or functional saturation, and how the data for displaying the measurement was gathered from the patient. Some workers have now taken up this challenge.
Byrne et al15 measured oxygen saturation in upper and lower limbs of 22 babies with known cyanotic congenital heart disease and found that the difference in saturation between upper and lower limbs in babies with obligatory right to left ductal shunts was at least 7%, implying a postductal saturation of at most 93% in these cases. They also reported that the same babies had reduced saturation overall, with either upper or lower limb saturation being less than 88% compared with the norm of 97.6% (upper limb) or 97.3% (lower limb) measured in 3896 term infants. Only four of the term infants had similar low measurements, three of whom had congenital heart disease (hypoplastic left heart, Fallot’s tetralogy, coarctation of the aorta). Whether fractional or functional saturation measurements were used is not stated in this report, which has only been published as an abstract.
Kao et al11 measured fractional saturation in 45 normal term infants less than 48 hours of age, 25 infants with uncomplicated VSDs, and 21 infants with congenital cardiac malformations warranting surgery or catheterisation. They found that normal term infants had fractional saturation levels of mean (SD) 97.7 (1.27)%, and those with uncomplicated VSDs had a slightly lower mean of 96.5 (3.12)%. Those with more severe cardiac malformations had an even lower mean level of 88.3 (9.23)%. They concluded that the normal range of fractional saturation in the newborn period was narrow and that pulse oximetry may be useful in screening newborn babies for congenital heart disease requiring early intervention. They further mentioned that four of the infants in the group with more serious cardiac malformations had normal saturation measurements. Three of these had coarctation of the aorta, and the fourth had critical aortic stenosis. They concluded that pulse oximetry was not an effective screening tool for aortic stenosis or coarctation. Although it is likely that most of the measurements reported were postductal, this is not stated in the report which has only been published in abstract.
Koppel et al12,16 performed postductal fractional saturation measurements in over 11 000 babies at over 24 hours of age in a population with a high rate of antenatal screening for cardiac malformations. After birth they found three cases of “critical cardiovascular malformation” not previously identified, two cases of total anomalous pulmonary venous drainage, and one truncus. Four other babies with critical lesions became symptomatic before the time for screening. Two others were not detected before discharge home, one with a coarctation and one with a hypoplastic left pulmonary artery with aortopulmonary collaterals. In only one infant was the test falsely positive. This study has only been published in abstract.
Gnanalingham et al17 measured postductal fractional saturation in 1421 of 3218 deliveries (44%) at between 30 minutes and 6 hours of age (mean 1.7 hours) over a 12 month period. They found a mean (SD) saturation of 96.6 (3.8)%. In 2% of cases (31), saturation was 90% or below, 13 of whom had clinical problems. Two had early onset group B streptococcal infection, and one had a pulmonary artery anomaly. This study has only been published in abstract form.
One striking feature of the series reported by Koppel is the very low false positive rate, one case in 11 000. Part of the reason for this may be that all measurements were taken after 24 hours of age in this series and in many cases not until 48 hours of age. There is a suggestion from our data that the proportion of false positives is higher if measurements are taken before 24 hours of age as against those taken later. In our series, the mean age of measurement was 11.7 hours and the mean saturation was 98.04%. In Gnanalingham’s series, the mean age of measurement was only 1.7 hours, and it is interesting to note that this series also reports the lowest mean saturation at 96.6%. This adds some weight to the argument that the earlier after birth the measurement is made the greater the risk of false positive results. Some balance needs to be struck, however, between the reduction in false positive results that occurs by waiting for 24–48 hours after birth and the problems caused by late appreciation of severe hypoxaemia in babies caused by persistent pulmonary hypertension of the newborn or cyanotic congenital cardiac malformation. Furthermore, a test that required measurements to be made after the age of 24 hours would be of limited value in the United Kingdom, where a significant and increasing proportion of asymptomatic term babies are discharged home before that time.
Judgments about any screening endeavour should really be made with a knowledge of the sensitivity and specificity of the process. Suppose we define the process as, where necessary, two measurements of postductal fractional saturation and the trigger level for action as failure to achieve 95% on the first and, failing that, on the second of these measurements. Suppose we further define the object of the screening process as the identification of congenital cardiac malformation other than isolated VSD in asymptomatic infants of 35 weeks gestation or more who are without obvious dysmorphism. In this study, 10 infants out of a possible 19 were detected as a result of saturation measurement (if one allows the antenatally diagnosed infants to be initially identified by saturation where this was possible). However, 51 babies had two measurements of saturation at less than 95%. If one adds to this 51 the nine babies about whom concerns were raised by the first examination (who therefore did not have a second measurement) and the four babies in whom antenatal scans had already raised concerns, this total rises to 64 babies who “failed” the screen. These 64 babies included 10 with congenital cardiac malformations other than isolated VSDs. The true positives are thus 10, the false positives are 54, the false negatives are nine (fig 2 groups A and B excluding VSDs), and the true negatives are 5626−10−54−9 = 5553. If one accepts these assumptions, then the sensitivity of such a process is 53% and the specificity is 99%.
It should be remembered also that this calculation fails to take account of the 13 babies without cardiac malformation but with other appreciable problems who were also brought to light by this process (table 1). Furthermore, the specificity of this test is “exaggerated” by the rarity of the condition in question. In a condition such as congenital cardiac malformation, which (if one excludes isolated VSD) has a birth prevalence of about 3.5 per 1000, the specificity falls by about 1% for every 50 false positives in a sample of this size.
The midwives performing this test felt that measuring postductal saturation required, on average, five minutes of their time per baby over and above their other duties. Clinical examination and scanning of babies with low saturation measurements were reckoned to require 20 minutes of a consultant’s time if the baby proved to have no cardiac malformation. If employing a midwife costs about £25 000 per year for a 36 hour week and a 44 week year, her time costs £14.46 per hour worked. Midwifery costs are thus about £1205 per 1000 babies screened, increasing to £1261 to allow for the few babies who require a second measurement. About 11 babies per 1000 screened will require ultrasound examination. Assuming consultant time costs three times as much as midwifery time, then this adds a further £160 per 1000 babies screened giving a combined cost of around £1450 per 1000 babies screened. If it is accepted that in our study saturation measurement facilitated the early diagnosis of six cases of congenital heart disease (or perhaps 10 if antenatal diagnosis had not already occurred) among a population of 5626 babies screened, this amounts to about £1450 (or perhaps £850) per case of congenital heart disease identified. This very simplified and amateur costing compares with the more professional cost assessment of screening for phenylketonuria, which found a cost of £3160 per 1000 babies screened or £26 827 per case identified.18
In summary, it is possible to establish a routine whereby measurement of postductal fractional saturation in asymptomatic term infants is achieved in over 98% of those eligible before discharge home after birth. Such a measurement brings to light important pathology in a timely fashion without causing concern to the families of large numbers of healthy infants. In a situation where there is easy access to echocardiography, it allows early diagnosis of severe congenital cardiac malformation that might otherwise be missed, or delayed, to the detriment of the babies concerned. We plan to expand the study to a larger population base to explore its possibilities further.
Acknowledgments
We are particularly grateful to Dr Jonathan Wyllie who first suggested that we should explore oximetry screening. We are indebted to the Children’s Heart Unit Foundation for their support of the cardiological database and to all our colleagues in the northern region and at the Maternity Survey Office whose continued support maintains the Northern Congenital Abnormality Survey and the Regional Perinatal Mortality Survey. We would also like to thank the families of Sunderland who allowed us to make measurements on their babies and to acknowledge the hard work and organisational skills of the midwives at Sunderland Royal Hospital who made the measurements.
REFERENCES
Linked Articles
- Fetal and Neonatal this issue