Article Text

Abstract
Objective: To compare the resistance in vitro of different devices used for the delivery of nasal continuous positive airway pressure (NCPAP) in neonates.
Design: Flows of 4–8 litres/min were passed through a selection of neonatal NCPAP devices (single prong, Duotube, Argyle prong, Hudson prong, Infant Flow Driver), and the resultant fall in pressure measured using a calibrated pressure transducer.
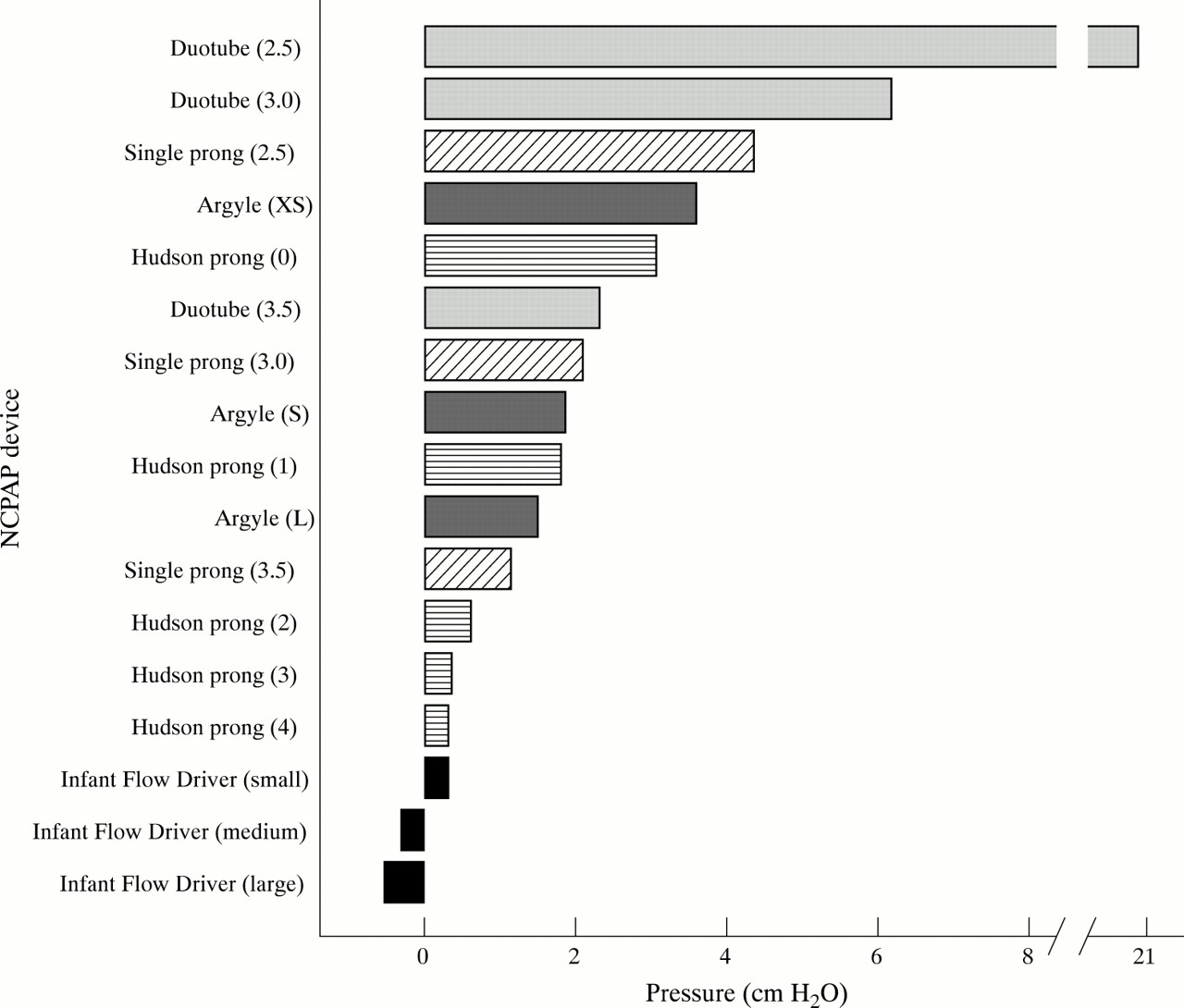
Results: The decrease in pressure (cm H2O) for each device (size in parentheses) at a constant flow of 6 litres/min was: Duotube: (2.5), 21; (3.0), 6.2; (3.5), 2.3; single prong: (2.5), 4.4; (3.0), 2.1; (3.5), 1.2; Argyle prong: (XS), 3.6; (S), 1.9; (L), 1.5; Hudson prong: (0), 3.1; (1), 1.8; (2), 0.6; (3), 0.4; (4), 0.3; Infant Flow Driver: (small), 0.3; (medium), −0.3; (large), −0.5.
Conclusions: A large variation in the potential fall in pressure may occur in the clinical setting. Devices with short double prongs had the lowest resistance to flow. These results have implications in the selection of the optimal device/s for clinical application and for future comparisons in randomised trials of NCPAP in neonates.
- positive pressure respiration
- airway resistance
- CPAP, continuous positive airway pressure
- NCPAP, nasal continuous positive airway pressure
Statistics from Altmetric.com
Continuous positive airway pressure (CPAP) was first used to support the breathing of neonates in the early 1970s. The initial mode of delivery through an endotracheal tube or headchamber1 was superseded by the use of nasal prongs which could deliver CPAP in a simpler and less invasive manner.2,3
Nasal continuous positive airway pressure (NCPAP) is now an established mode of respiratory support for neonates in the period after extubation4 and is often used as the primary treatment for respiratory distress5 and apnoea of prematurity.6,7 As a consequence of further developments8–11 and a continuing clinical need, there is now a broad range of prongs used to deliver NCPAP. There is little information to guide clinicians or researchers seeking to compare the effectiveness of these devices.
One important characteristic of a NCPAP device is its resistance to airflow. This determines the fall in pressure from that measured in the delivery circuit to that transmitted to the respiratory tract. Although previous work has analysed the resistance of neonatal endotracheal tubes,12,13 there have been no direct comparisons of the resistance of NCPAP devices. Our objective was to measure the pressure drop across a variety of NCPAP devices used in current neonatal practice.
METHODS
We selected a series of NCPAP devices of different sizes currently used in neonatal intensive care units. These were:
Hudson prong (Hudson-RCI, Temecula, California, USA), sizes 0 to 4;
Argyle prong (Sherwood Medical, St Louis, Missouri, USA), sizes large (L), small (S), and extra small (XS);
Flow Driver generator (EME, Brighton, UK), prong sizes small, medium, and large;
Duotube (Parker Medical, Melbourne, Australia), sizes 2.5, 3.0, and 3.5 mm (outer diameter);
Mallinckrodt endotracheal tube (Mallinckrodt Medical, Athlone, Ireland) cut to a length of 5 cm (internal diameters of 2.5, 3.0, and 3.5 mm) with a connector (RPS; Sims, California, USA).
Prong dimensions (table 1) were measured using digital calipers accurate to ± 0.03 mm.
Dimensions of nasal continuous positive airway pressure devices and pressure drop with various flows
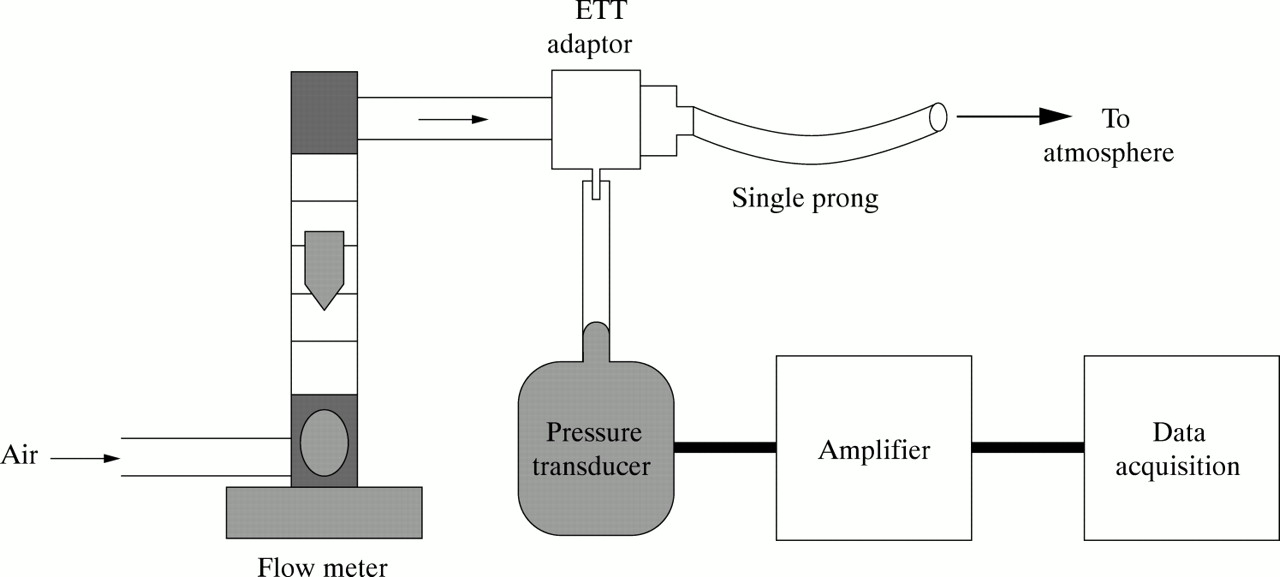
Flows of 4–8 litres/min were applied to the device so that the entire flow passed through the prong/s. These flows were selected because they encompass the typical range of flows observed to flow through Hudson prongs in our unit. The flow was measured using a Platon flow meter (G A Platon Ltd, Sheffield, UK) with a range of 0–10 litres/min and an accuracy of ± 1.25% of full scale. Air was used for all measurements, and room temperature during the study varied from 24 to 26°C. Figure 1 shows the apparatus connected to a single prong.

Apparatus connected to a single prong device.
The pressure generated by the resistance to flow in each device (pressure drop) was measured using a Sensym pressure transducer (Sensortechnics, Puchheim, Germany) with an operating range of 0–13 cm H2O and a typical combined accuracy of ± 0.2% of full scale. The transducer was connected to the pressure port of the device, if one was present, or to a pressure port on a connector (with negligible intrinsic resistance at these flows) attached directly to the device. The pressure was measured twice at each flow, with variation between values in the transducer operating range not exceeding 0.1 cm H2O and typically less than 0.05 cm H2O. The transducer was calibrated before each study using a water manometer. The analogue output from the pressure transducer was amplified (PC Polygraph HR; Synectics Medical, Stockholm, Sweden), digitised, and recorded using Spectra software.14 Pressures greater than 15 cm H2O have been rounded to the nearest cm H2O.
The bar graph (fig 2) was created using SPSS.15 The study was carried out in the Department of Neonatology at the Royal Women's Hospital, Melbourne, Australia.
{kind=link}
{kind=link}
Pressure measured in nasal continuous positive airway pressure (NCPAP) devices at a flow rate of 6 litres/min. Device sizes are given in parentheses.
RESULTS
Table 1 summarises the device dimensions and decrease in pressure measured on passing different flows through the NCPAP devices. Figure 2 shows the pressure measured in the devices at a constant flow of 6 litres/min represented as a bar graph.
Of all the double prong devices, the Infant Flow Driver, medium and large sizes, showed the lowest decrease in pressure, with increasing flows generating an increasingly slightly negative pressure. The pressure generated in the Infant Flow Driver with small prongs was equivalent to that generated in the size 4 Hudson prong. The largest falls in pressure were evident in the size 2.5 and 3.0 Duotube.
The single prong device (Mallinkrodt tube plus connector), at a length of 5 cm and internal diameter of 2.5 mm, showed a greater fall in pressure than all the short double prongs assessed. The small Argyle prong was equivalent to the size 1 Hudson prong, and the extra small Argyle prong showed a large pressure drop, smaller only than the Duotubes and the single prong of internal diameter 2.5 mm.
DISCUSSION
Resistance to flow is a significant factor when selecting the most appropriate device to deliver NCPAP. However, data on the impact of different NCPAP devices on clinical outcomes and physiological parameters are limited.
A study by Goldman et al16 showed the increased resistance and imposed work of breathing with Argyle prongs compared with a face mask for the delivery of CPAP to neonates. Courtney et al17 examined the effect of three different nasal devices on lung volume, showing better recruitment when using increased flow, via the Flow Driver system, to increase pressure compared with fixed flows through Inca prongs and modified nasal cannulae. A short term randomised study comparing the Flow Driver system with conventional nasal prongs showed no difference in the incidence of apnoea, bradycardia, and desaturations.18 Others compared the Flow Driver system with the single nasal prong and found no significant difference in various physiological parameters over short time periods.19,20
Randomised trials have compared the impact of different double nasal prong devices on rates of extubation failure in preterm neonates.21,22 Other randomised trials have shown a reduced rate of extubation failure with use of double nasal prong devices compared with single nasal prongs.23,24
Although the resistance of a NCPAP device is important, other factors may contribute to the effectiveness of different devices in the neonatal intensive care setting. These include the characteristics of the pressure source. Underwater bubble CPAP, for example, delivers to the circuit an oscillatory pressure waveform that may have its own clinical effect. The ease of use, patient comfort, and avoidance of trauma to the nares and columella25,26 when nasal prongs are used are important factors which also require further evaluation.
Although other factors must be considered, we have shown that there is significant variation in resistance between different nasal prongs, which is likely to result in different degrees of transmission to the airway if the pressures and flows in the CPAP delivery system are equal. Resistance in the medium and large sized Infant Flow Driver prongs is sufficiently low to create a negative pressure within the device by virtue of the Venturi effect. The fall in pressure in the size 2.5 and 3.0 Duotube is high relative to the other devices, even at low flows. Despite these findings, it is important to note that they do not establish the clinical superiority of one device over another.
Further studies using meaningful clinical outcomes are required to define the optimal method and interface for NCPAP administration. We recommend comparisons in future trials of the short, double prong devices with low resistance identified in this study.
Acknowledgments
This study was supported by: the Royal Women's Hospital Foundation and the Division of Research and Education, Royal Women's Hospital, Melbourne; Murdoch Children's Research Institute.
REFERENCES
Linked Articles
- Fantoms