Article Text

Abstract
Supplemental oxygen is a safe and effective treatment for infants with established chronic lung disease who are not at risk of further progression of retinopathy of prematurity (ROP). Oxygen saturations of < 92% should be avoided and a target range of at least 94–96% aimed for. The saturation target range for very preterm infants at risk of developing ROP is more controversial, but the therapeutic index is probably considerably narrower.
- chronic lung disease
- oxygen therapy
- retinopathy of prematurity
- premature
- lung
- CLD, chronic lung disease
- ROP, retinopathy of prematurity
Statistics from Altmetric.com
Infants with chronic lung disease of infancy (CLD) and hypoxaemia requiring supplemental oxygen are likely to be a problem as long as preterm deliveries continue to occur. Antenatal and postnatal corticosteroids have decreased the prevalence of respiratory distress syndrome, and the use of lower inspired oxygen tensions and reduced positive inspiratory pressures during mechanical ventilation has contributed to a lower prevalence of CLD. In infants surviving increasingly premature delivery, antenatal and postnatal infection and patent ductus arteriosus both contribute to the development of CLD.1 Discussed below is the rationale and aims of oxygen therapy in infants with CLD. The following article by Professor Abman focuses on cardiovascular aspects in children with CLD.
RATIONALE AND PHYSIOLOGICAL EFFECTS OF SUPPLEMENTAL OXYGEN
Although the potentially damaging effects of oxygen toxicity must be recognised and avoided, there are clear reasons why the administration of supplemental oxygen to hypoxaemic infants with CLD is beneficial. Alveolar hypoxia is a well described cause of pulmonary artery hypertension resulting from hypoxic pulmonary vasoconstriction. Supplemental oxygen reverses hypoxic pulmonary vasoconstriction, improving oxygen saturation, decreasing pulmonary vascular resistance, and improving right ventricular performance and peripheral oxygen delivery.2,3 Abman reported cardiac catheterisation findings of significant decreases in pulmonary artery pressure, from 48 to 25 mm Hg, in infants with CLD given 80% oxygen, and found that most of the benefit occurred at much lower oxygen concentrations which could be administered by nasal cannula at home.4 Some infants who do not respond fully to oxygen may have further decreases in pulmonary artery hypertension with the administration of hydralazine, although this appears to be contraindicated in infants with large systemic to pulmonary collateral vessels.5
Infants with CLD who are oxygen dependent can have a difficult first few years, often not growing well and requiring frequent readmission to hospital for respiratory exacerbations.6 Right ventricular hypertrophy resolves, but only gradually.3,6 Groothuis and Rosenberg7 found, however, that supplementation with oxygen at home enabled oxygen dependent infants to grow as well as healthy full term infants. Inappropriately early discontinuation of oxygen caused a significant deceleration in weight gain, which again improved when oxygen supplementation was restarted.
The effects of chronic hypoxaemia on growth of the central nervous system and its effects on developmental status have been studied. It is difficult to separate the long term consequences of adverse neurological events associated with premature delivery from those of chronic postnatal hypoxaemia. Lifschitz et al8 described a two year follow up of infants with CLD with birth weights of less than 1500 g: 20% had hearing impairment or were registered blind, 30% had cerebral palsy, and 46% had abnormal developmental scores. Whereas the requirement for oxygen at hospital discharge did not predict developmental score, a history of intraventricular haemorrhage and pulmonary air leak and the length of hospital stay did. Doyle et al9 performed an eight year follow up of infants with birth weights less than 1000 g. Contrary to the authors' expectations, children who had received less oxygen and ventilation had poorer growth and more severe cerebral palsy. Although this may have been surprising in that children who required more oxygen may have been expected to have more severe disease and therefore more adverse outcomes, it may indicate that programmes aimed at aggressively normalising oxygen saturations may help to avert adverse neurological outcomes.
IDEAL OXYGEN SATURATION TARGETS: RISKS AND BENEFITS OF OXYGEN
Within days of normal full term birth, arterial oxygen partial pressure approximates that seen in the normal adult. It is therefore logical to aim for saturations of 95–99% in the full term (or equivalent postconceptional age) and older infant. However, in premature infants with immature retinae, high inspired oxygen concentrations were clearly linked to the development of retinopathy of prematurity (ROP) in the 1940s and 1950s.10 (Oxidant injury may also play a role in the pathogenesis of CLD.) Most of the controversy about the saturation targets of oxygen therapy clearly surrounds the preterm infant who has not yet reached term postconceptional age. In reaction to the threat of ROP associated with unrestricted supplemental oxygen, many took the opposite approach, severely restricting supplemental oxygen. It has been estimated that, as a result, 16 children died or survived with severe disability for every child whose sight was saved.11 More recent approaches with cautious oxygen restriction found reduced incidence and severity of ROP without unduly increased death rates.12 Although until recently, oxygen saturations of 96–99% were considered unsafe for the retinal vessels of the premature infant, and values of 90–95% were targeted instead, new evidence on the safety of higher saturation targets has recently appeared. In the United States, a multicentre trial of 649 oxygen dependent premature infants with moderately severe ROP (“STOP-ROP” study) determined the effect on progression from prethreshold to threshold ROP of two different oxygen saturation targets: 89–94% and 96–99%.13 “Threshold ROP” is defined as ROP severe enough to warrant laser therapy or cryotherapy. This study found no adverse effect with the higher saturation targets, and in some cases risk of progression was even decreased (48% to 41%). Using similar number needed to treat analysis as above, it has been estimated that about 13 infants with prethreshold ROP need to be treated with supplemental oxygen to prevent one child needing retinal surgery. Of some concern, however, was the finding of a marginally higher incidence of pulmonary complications in the infants treated with the higher saturation targets.
In contrast, Tin et al14 retrospectively studied the records of 295 infants born before 28 weeks gestation and found that saturation targets as low as 70–90% were associated with significantly less threshold disease (4% incidence) than saturation targets of 88–98% (18% incidence). The STOP-ROP and Tin studies are difficult to compare because the STOP-ROP trial prospectively studied only infants with prethreshold ROP, in whom the risk for progression to threshold is understandably higher, whereas the retrospective study of Tin et al examined all preterm births. Both studies seem to agree that the risk of progression to threshold ROP is much reduced after 30–32 weeks postconceptional age.14,15 Tin et al have readily admitted that their paper generates a hypothesis that lower oxygen saturations may be acceptable. There is obvious concern about accepting lower oxygen saturations in view of potential cardiac, neurological, and growth consequences. The multicentre Australian “BOOST” study may go some way to addressing this issue. The trial, we believe, is studying the effects on growth, health, and development of infants with CLD (irrespective of their ROP status) randomised to the same two target oxygen saturation ranges used in the STOP-ROP trial.
One understudied risk factor is wide swings of oxygen saturation, irrespective of the absolute percentage saturation. There is some speculation that the vascular damage related to hypoxia or hyperoxia may be more a consequence of sudden decreases and increases in oxygen level, which are associated with episodic oxidant damage, rather than hypoxia or hyperoxia per se. Evidence for this exists for ROP but not for the lung.16 If this were true, it would argue for closer continuous saturation monitoring.
No matter what oxygen saturations are targeted for infants with CLD at home, it must be recognised that significant oxyhaemoglobin desaturation can occur during periods of feeding or sleep, and appropriate adjustments in supplemental oxygen levels should be made during these periods. Clinically unsuspected hypoxaemia often occurs in infants with CLD, and to a lesser extent with prematurity alone than in control full term infants.17 Desaturation seems more severe during feeding than during wakefulness, active, and quiet sleep. Singer et al18 described similar problems in infants with CLD but found that hypoxaemia was more severe after feeding than during. It has been speculated that such desaturation puts these infants at higher risk of sudden unexplained death.17 Sleep state related changes in control of breathing could also affect sleeping oxygen saturation levels. Sekar and Duke19 described more central apnoea and desaturation in sleeping infants with CLD than in preterm controls; oxygen saturation, central apnoea, and periodic breathing all improved with supplemental oxygen therapy, which may have improved central respiratory stability. Such sleep related decreases in oxygen saturation are worsened by certain positions—for example, sleeping in a “containing posture” or hammock, which has been proposed to have advantageous neurodevelopmental effects in preterm infants.20 Abnormal sleep architecture in infants with CLD helps to maintain oxygen saturation by increasing arousals.21 This sleep fragmentation and decreased REM sleep can be improved with supplemental oxygen. A targeted saturation of at least 93% optimises sleep architecture in these infants.22 In summary, oxygen saturations of < 92% should be avoided and a target range of 94–96% aimed for. Such a range will provide a buffer zone against desaturations during feeding and sleep.
EQUIPMENT FOR MONITORING OXYGEN SATURATION
Non-invasive monitoring of transcutaneous Po2 (Ptcco2) and percentage oxyhaemoglobin saturation has revolutionised our ability to accurately track oxygenation status. Pulse oximetry can accurately track changes in arterial blood gas saturation in the 80–100% range measured over a wide range of heart rate, blood pressure, packed cell volume, Pco2, and pH values in infants with CLD, and seems to be more accurate than Ptcco2.23,24 This is also true in very low birthweight infants.25 Other advantages of pulse oximeters over Ptcco2 monitors are that the instruments do not require calibration or cause skin burns. Accuracy of pulse oximetry does diminish in the lower ranges of oxygen saturation.26 More sophisticated use of pulse oximetry has enabled it to be used as more than simply a monitoring device. Bhutani et al27 described a system whereby feedback from a pulse oximeter provided online adjustment of Fio2 according to an adaptive programme. Such adaptive Fio2 control achieved a steady oxygen saturation of 94–96% for 81% of the time, compared with 54% of the time using a standard neonatal intensive care protocol. Such adaptive programmes may be particularly useful in not only achieving oxygen saturation target ranges, but in also preventing widely varying swings in oxygen saturation.
DISCHARGE PLANNING
Oxygen therapy does not require a hospital environment, and major benefits accrue from discharging stable infants with CLD while they are still receiving supplemental oxygen. The major benefit is promotion of normal development and parent-infant bonding, which is best achieved in the environment of the home. Considerable financial benefits are achieved for the health care system (not necessarily for the family), and the risk of nosocomial infection is eliminated, although counselling against exposure to viruses from ill relatives and friends at home must be given. Sending premature infants home while they are receiving oxygen therapy requires careful planning to ensure success, taking into account a number of patient, family, financial, home, and community factors. This is best done in the context of an organised programme of discharge planning and parent education.28,29 These have recently been discussed (ATS BPD statement; in review). The infant needs to be first and foremost medically stable, showing good growth and without frequent events leading to desaturation and CO2 retention.30 If chronic CO2 retention is present, it is preferably controlled at less than 50 torr or so, although higher levels may be acceptable if stable; some form of intermittent non-invasive or invasive, or continuous invasive ventilatory assistance aimed at resting the respiratory muscles may be occasionally required to achieve these goals.
The duration of home oxygen therapy has varied widely. Beca et al30 reported a mean duration of 71 days (range 7–339). The mean age of discontinuation of home oxygen therapy has been reported to be 13.4 months, but again varies widely. Baraldi et al32 reported that, in a prospective home oxygen therapy programme, infants with CLD were discharged at a mean age of 3.7 months, mean duration of oxygen therapy was 97 days (range 15–320), and the mean age of discontinuation of oxygen was 6.9 months (range 3–14.7). Infants improved at home; right ventricular hypertrophy resolved in most, and there was no further progression of ROP, but weight gain remained sluggish at the third centile.
EQUIPMENT FOR DELIVERING OXYGEN
A number of methods are available for delivering oxygen.33 Oxygen concentrators are best suited for infants with CLD who require low flows of between 0.06 and 0.8 litres/min.34 They work by filtering air through a series of filters to remove particulate matter (including bacteria) and nitrogen with the resultant oxygen stored in a reservoir before use. Usually two outlets are sufficient: one in the main living room area and another in the child's bedroom. Oxygen cylinders (PD size) are essential for mobility, and the newer cylinders made of aluminium are much lighter than the traditional steel ones. Liquid oxygen, which is stored at −183°C, is more suitable when the oxygen requirements are high. As most infants require less than 1 litre of oxygen per minute, this is only occasionally used in infants with CLD. The general practitioner currently prescribes these items, and the local oxygen company will provide both training and a 24 hour back up service for the parents or guardians. Low flow oxygen is delivered in most cases through a nasal cannula. In addition to back up provided for the equipment, access to 24 hour medical care is also essential especially at times of intercurrent viral illness.
CARE IN THE COMMUNITY
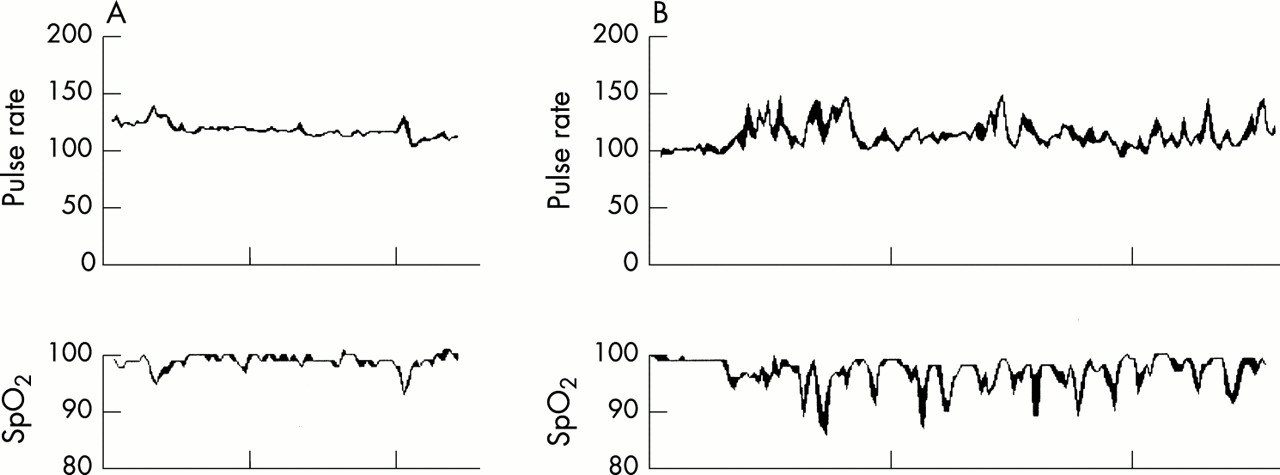
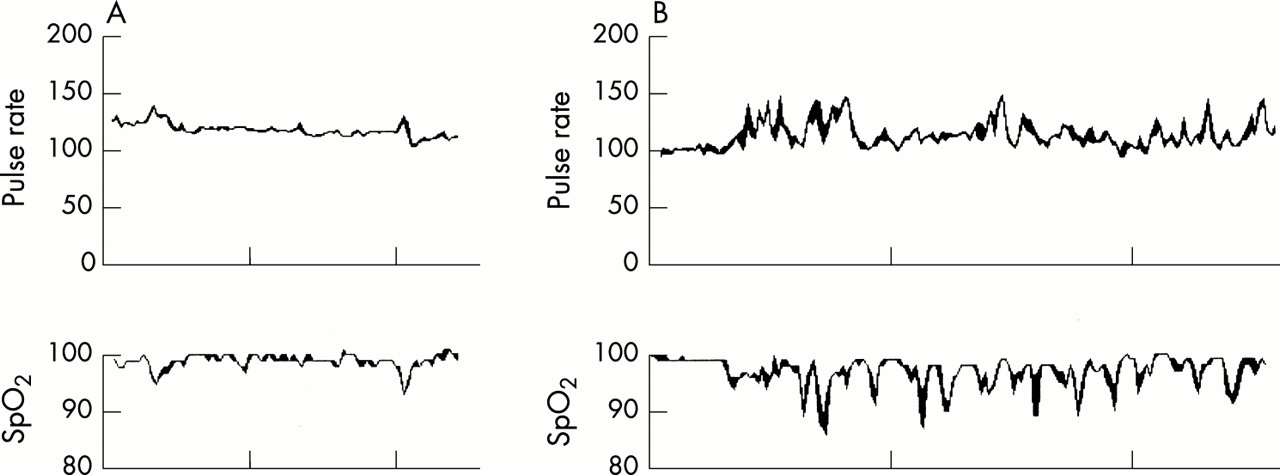
Many centres in the United Kingdom have developed the use of specialist respiratory nurses for monitoring children at home on oxygen, although a number of other people are essential for the service. These include dieticians, health visitors, general practitioners, hospital and community paediatricians, social workers as well as other professionals such as physiotherapists and speech therapists. Initially, after discharge, the infant is seen frequently especially as parental anxiety is likely to be high. At each visit, the child's progress is monitored with particular attention to the respiratory, cardiovascular, and neurological systems, and to the growth of the child. Any parental anxiety is addressed, and the children are also seen within the hospital setting on a regular basis. “Spot” checks of oxygen saturations are insufficient to guide oxygen therapy, and prolonged monitoring of oxygen saturation by pulse oximetry while the child is awake, feeding, and asleep is likely to provide a more accurate picture of the child's respiratory status. Modern software will rapidly analyse the data stored in pulse oximeters, and, according to preset parameters, identify episodes of hypoxaemia as well as the average oxygen saturation (fig 1). Arterial or indeed capillary blood gases are rarely performed in the stable situation, and transcutaneous monitors are rarely used. Management of the cardiovascular system is discussed in more detail in the following article.
{kind=link}
Continuous monitoring of oxygen saturation of infants. (A) Trace from an infant recently weaned off oxygen. Note that the average oxygen saturation in air is consistently > 95%. (B) Trace from an oxygen dependent infant with chronic lung disease (CLD). Note the numerous desaturations falling consistently below 90%. Although there was no clinical evidence, oesophageal pH monitoring showed appreciable gastro-oesophageal reflux. After treatment for reflux, the oxygen desaturations improved, but oxygen dependency continued for several more months because of CLD. The x axis shows time with 20 minute intervals.
WEANING FROM HOME OXYGEN
No uniform standards are used in weaning infants from home oxygen. Most commonly, prolonged pulse oximetry (fig 1) is used to determine when it is appropriate to wean infants from supplemental oxygen, using target saturation values similar to those used during oxygen supplementation. Weaning is also likely to be influenced by other factors, including associated medical problems (for example, pulmonary hypertension), somatic growth, and sometimes the weather. It should also be remembered that saturation measurement when the infant is awake may not reflect sleeping saturations. Moyer-Mileur et al35 compared saturations during short term (20–30 minute) awake studies with prolonged sleeping studies in infants with CLD, and found no correlation. Furthermore, they compared infants whose supplemental oxygen was discontinued on the basis of normal short term studies, but who had saturations of 88–91% during prolonged sleep studies, with infants who had saturations of greater than 92% during prolonged sleep studies. The infants with lower saturations had a significant decrease in weight gain (from 17.3 to 3.7 g/kg/day), z scores for weight gain, and weight for height compared with the infants with higher saturations.
Longer awake studies using higher saturations as targets may allow more accurate prediction of which infants will tolerate discontinuation of oxygen at home. Vermeulen et al36 showed that infants who could be weaned from oxygen had awake median saturations of 97% during one hour awake studies, spent only 14% of time with saturation ≥95% and 2% of time ≥ 92%. Two hour room air challenges were used by Simoes et al37 to determine suitability for weaning from room air. They found that in most infants, the lowest saturation levels were reached by 40 minutes after the discontinuation of oxygen and that all infants receiving oxygen flow rates ≥ 20ml/kg were able to maintain room air saturations ≤ 92%. Such infants were able to maintain weight and height centiles six months after oxygen had been discontinued.
Whether oxygen is weaned early or late after discharge home is not as important as weaning while maintaining target oxygen saturation levels.38 Gradual weaning does seem preferable to abrupt weaning in terms of ROP risk, independent of the duration of oxygen therapy.39
CONCLUSIONS
Supplemental oxygen is a safe and effective treatment with a wide therapeutic index in the infant with established CLD who is not at risk of further progression of ROP. In such infants, oxygen saturations of < 92% should be avoided and a target range of at least 94–96% aimed for. Recent studies have shown the safety of higher oxygen saturation targets (95–99%) in appropriate infants. Such a range will provide a buffer zone against desaturations during feeding and sleep. This target is consistent with current recommendations.40 Maintenance of oxygen saturations in this range reduces complications from pulmonary artery hypertension and promotes growth. The saturation target range for very preterm infants at risk of developing ROP is more controversial, but it seems clear that the therapeutic index is considerably narrower. Pulse oximetry monitoring can be an accurate and effective way to maintain oxygen saturations within target ranges, especially during sleep, when oxygen saturation is likely to fall to suboptimal levels.
REFERENCES
Linked Articles
- CORRECTION