Article Text

Abstract
AIMS To prospectively evaluate the iron nutritional status of preterm infants fed either a term (0.5 mg/dl iron) or preterm (0.9 mg/dl) formulas fortified with iron after hospital discharge.
METHODS Healthy low birthweight preterm infants were randomly assigned into three groups at the time of hospital discharge. Group A were fed an iron fortified preterm formula (0.9 mg/dl iron) until 6 months corrected age; group B, a fortified term formula (0.5 mg/l iron) until 6 months corrected age group C, the preterm formula between hospital discharge and term, then the term formula until 6 months corrected age.
RESULTS Seventy eight infants were followed up to 6 months corrected age. Iron intake from formula differed significantly between the groups (A, 1.17 mg/kg/day (SD 0.32) > C, 0.86 mg/kg/day (SD 0.40) = B, 0.81 mg/kg/day (SD 0.23); p < 0.0001). Haemoglobin concentrations were similar to those of iron sufficient preterm infants of the same postnatal age, and term infants of the same postmenstrual age (after 3 months of age). There were no significant differences in haemoglobin concentration (p = 0.391), plasma ferritin (A vs B, p = 0.322), or in the incidence of iron deficiency (A vsB, p = 0.534).
CONCLUSIONS Iron fortified formulas containing between 0.5 and 0.9 mg/dl iron seem to meet the iron nutritional needs of preterm infants after hospital discharge.
- anaemia
- infant formula
- iron deficiency
- preterm infants
Statistics from Altmetric.com
Preterm infants have high iron requirements due to their rapid growth and relatively low iron stores at birth.1 2Without iron supplementation, iron deficiency anaemia is common.3-5 The American Academy of Pediatrics and the European Society of Pediatric Gastroenterology and Nutrition recommend that preterm infants receive at least 2 mg/kg/day of iron after hospital discharge to prevent the development of iron deficiency anaemia, either as medicinal iron drops or as a formula fortified with at least 1.2 mg/dl iron (1.5 kcal/ dl).6 7
Formula fed preterm infants at our institution have traditionally been discharged home receiving iron fortified formulas designed for term infants, without additional iron supplements. These formulas contain between 0.5 and 0.9 mg/dl iron,8 9 equivalent to one half or three quarters of the level recommended for preterm infants. To our knowledge, however, iron deficiency had not been a problem in these infants.
Recent studies have indicated that term infants have lower iron requirements than previously thought.10 11 This study therefore aimed to prospectively examine the iron nutritional status of preterm infants fed a term (0.5 mg/dl iron) or preterm (0.9 mg/dl iron) formula after hospital discharge until 6 months corrected age.
Methods
Preterm (gestational age ⩾ 32 weeks), low birthweight (birthweight ⩽ 1750 g) infants were recruited from the special care baby units of the Royal Victoria Infirmary, Newcastle-upon-Tyne and the Ashington General Hospital, Ashington. Infants were considered eligible if they were formula fed, growing normally (weight gain > 20 g/day), had no systemic disease, and were not receiving supplementary oxygen or any medications (other than vitamin drops). Informed parental consent was obtained, and ethical approval was given by the Newcastle and Northumbria Joint Ethics Committee. Subjects were part of a larger study of diet and growth in preterm infants.12
About 48 hours before discharge the infants were randomly assigned to one of three groups stratified by birthweight (⩽ or > 1250 g), using sealed envelopes. Group A were fed preterm formula (0.9 mg/dl iron, ≈ 1.13 mg/ 100 kcal) from discharge to 6 months corrected age. Group B were fed term formula (0.5 mg/dl iron, ≈ 0.76 mg/ 100 kcal) from discharge to 6 months corrected age. Group C received preterm formula from discharge to term, then the term formula until 6 months corrected age. Details of the composition of the formulas are given elsewhere.12 Recruitment began in October 1993 and continued until January 1997. A planned interim data analysis in June 1995 revealed no significant differences between groups A and C, and recruitment to group C was discontinued. After this time infants were randomly allocated only to groups A and B.
Infants were reviewed in the outpatient clinic at the Royal Victoria Infirmary every two weeks between discharge and term, then monthly to 6 months corrected age. At each visit blood was drawn by venepuncture for haemoglobin measurement (Coulter Counter Model STKS). After the interim data analysis infants in groups A and B also had plasma ferritin measured (Ferritin Mab, ICN Pharmaceuticals, Orangeburg, New York). All assays were carried out in the clinical haematology laboratory at the Royal Victoria Infirmary, Newcastle-upon-Tyne.
Formula was provided as pre-weighed boxes of ready to feed formula. Parents fed the infants freely, but saved all unused milk. The boxes of formula were returned at each clinic visit and re-weighed. Formula intake was calculated from the difference in weight of the boxes of formula, and averaged over the period from hospital discharge to term, then at each monthly visit. This was converted to an iron intake by multiplying by the iron content of the formula.
The introduction of solids was left solely to the parents. They were advised to delay weaning until 3–4 months corrected age and asked to inform the research team once weaning began. After 6 months corrected age parents were advised to change to a commercially available term infant formula, or follow on formula (iron content typically 0.5–0.9 mg/dl).9 Infants did not receive pasteurised cow’s milk before 12 months corrected age.
Before hospital discharge infants were fed a low birthweight formula (0.9 mg/dl iron) or a mixture of low birthweight formula and breast milk. Some of the infants recruited at the Royal Victoria Infirmary returned to their referring unit before discharge, and contact was maintained by weekly visits or telephone calls. Six of these infants received iron supplements before hospital discharge. No infant received recombinant human erythropoietin during hospital stay, or iron supplementation after discharge.
Anaemia was defined as a haemoglobin concentration more than two standard deviations below the mean for preterm infants of the same postnatal age5 or a haemoglobin concentration more than two standard deviations below the mean for term infants of the same corrected age13 after 3 months corrected age. Iron deficiency was defined as a plasma ferritin less than 10 μg/l.14
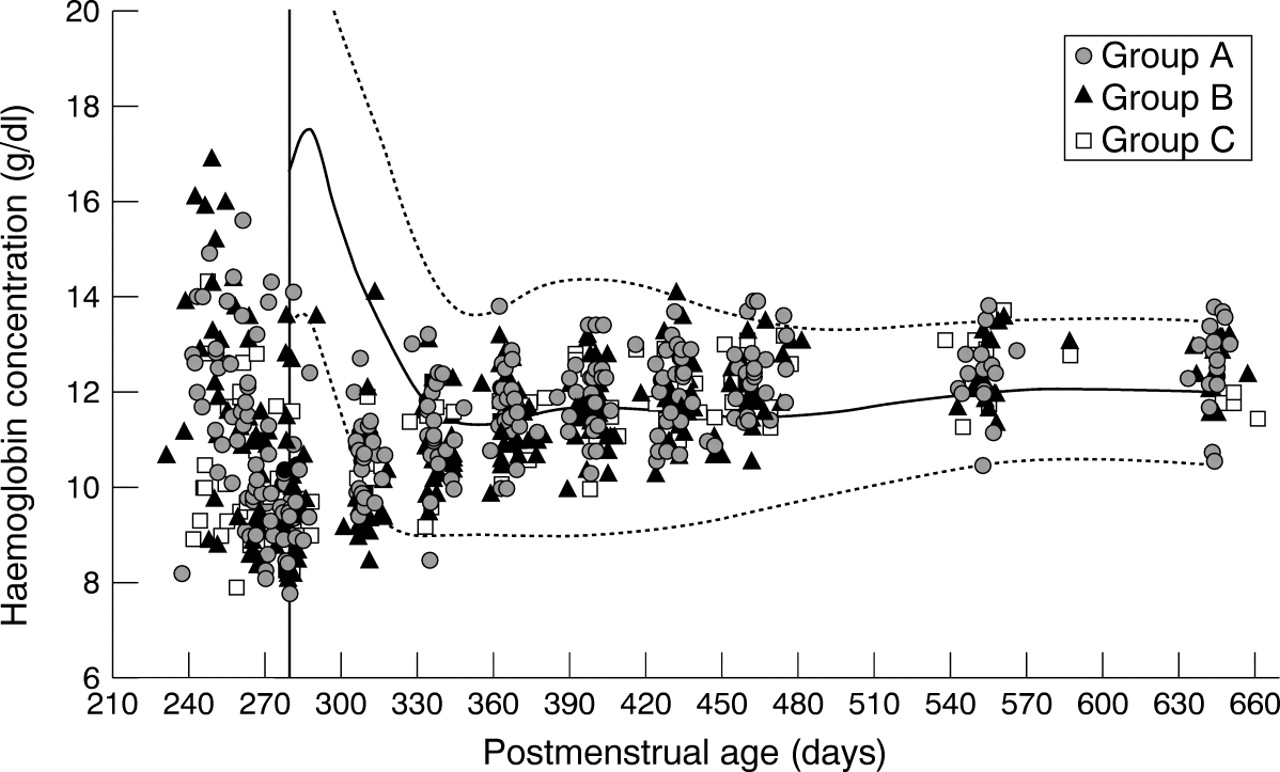
Haemoglobin concentrations for the study infants were compared with widely quoted reference data for iron sufficient term infants of the same postmenstrual age.13 The haemoglobin concentrations of study infants were compared with reference data for iron sufficient preterm infants5 of birthweights between 1000 and 1500 g, who did not receive blood transfusions while in hospital. Comparison was made with study infants of the same postnatal age who met these criteria.
Differences between the groups at birth and hospital discharge were assessed by one way analysis of variance (ANOVA) for continuous normally distributed data, and the χ2 test or Fisher’s exact test for nominal data. Non-normal variables were analysed using the Mann-Whitney U test, and Kruskal-Wallis tests for data with two, or more than two levels, respectively. Differences in haemoglobin and plasma ferritin after discharge were assessed by ANOVA and analysis of covariance (ANCOVA) for the visits 38 weeks to 6 months corrected age. Ferritin values were log transformed before analysis. Fisher’s PLSD test was used to correct for multiple testing. Results were considered significant at p < 0.05. All values are expressed as mean and standard deviation (SD) unless otherwise stated.
Statistical analysis was carried out using StatsView version 4.51 for Macintosh (Abacus Concepts Inc., Berkeley, CA) and SPSS version 6.2.1 for Windows. Smoothed curves were drawn for the haemoglobin reference data by interpolation using CA-Cricket Graph III version 1.51 (Computer Associates Inc., Islandia, NY).
Results
Eighty one infants were recruited and followed up to 6 months corrected age. Three infants, one from each group, received a blood transfusion after hospital discharge and were excluded from subsequent analysis (p = 0.999). Two of these infants were considered to have anaemia of prematurity, and responded promptly to a single blood transfusion. The third infant had been re-admitted to the paediatric intensive care unit at the Royal Victoria Infirmary with bacterial pneumonia, and was transfused during that admission. All three were transfused before 1 month of corrected age, none was iron deficient ( plasma ferritin < 10 μg/l) or microcytic (mean cell volume < 72fl).1
Seventy eight infants are therefore included in this report: 29 infants in group A, 34 in group B, and 15 in group C. The haemoglobin concentrations of 46 (59%) infants were measured at 9 months corrected age, and in 40 (51%) at 12 months corrected age.
The characteristics of the groups at birth and at the time of hospital discharge are shown in table 1. Most infants (56 %) received no blood transfusion before hospital discharge. The remaining infants received between one and five transfusions (median 1). Group C tended to receive fewer blood transfusions before hospital discharge, and had a lower haemoglobin concentrations at discharge (group Bvs group C, mean difference = 1.058 g/dl, p = 0.007).
Characteristics of group at birth and at discharge
Iron intake from formula is shown in fig 1. This differed significantly among the groups (group A, 1.17 mg/kg/day (SD 0.32) > group C, 0.86 mg/kg/day (SD 0.40) = group B, 0.81 mg/kg/day (SD 0.23); ANOVA p < 0.0001). Solids were introduced at a similar postnatal age (group A 119 days ( SD 32), group B 125 days (SD 33), group C 119 days (SD 29); ANOVA p = 0.680) and postmenstrual age (group A 336 days (SD 30), group B 339 days (SD 30), group C 334 days (SD 30); ANOVA p = 0.850) in the three groups.
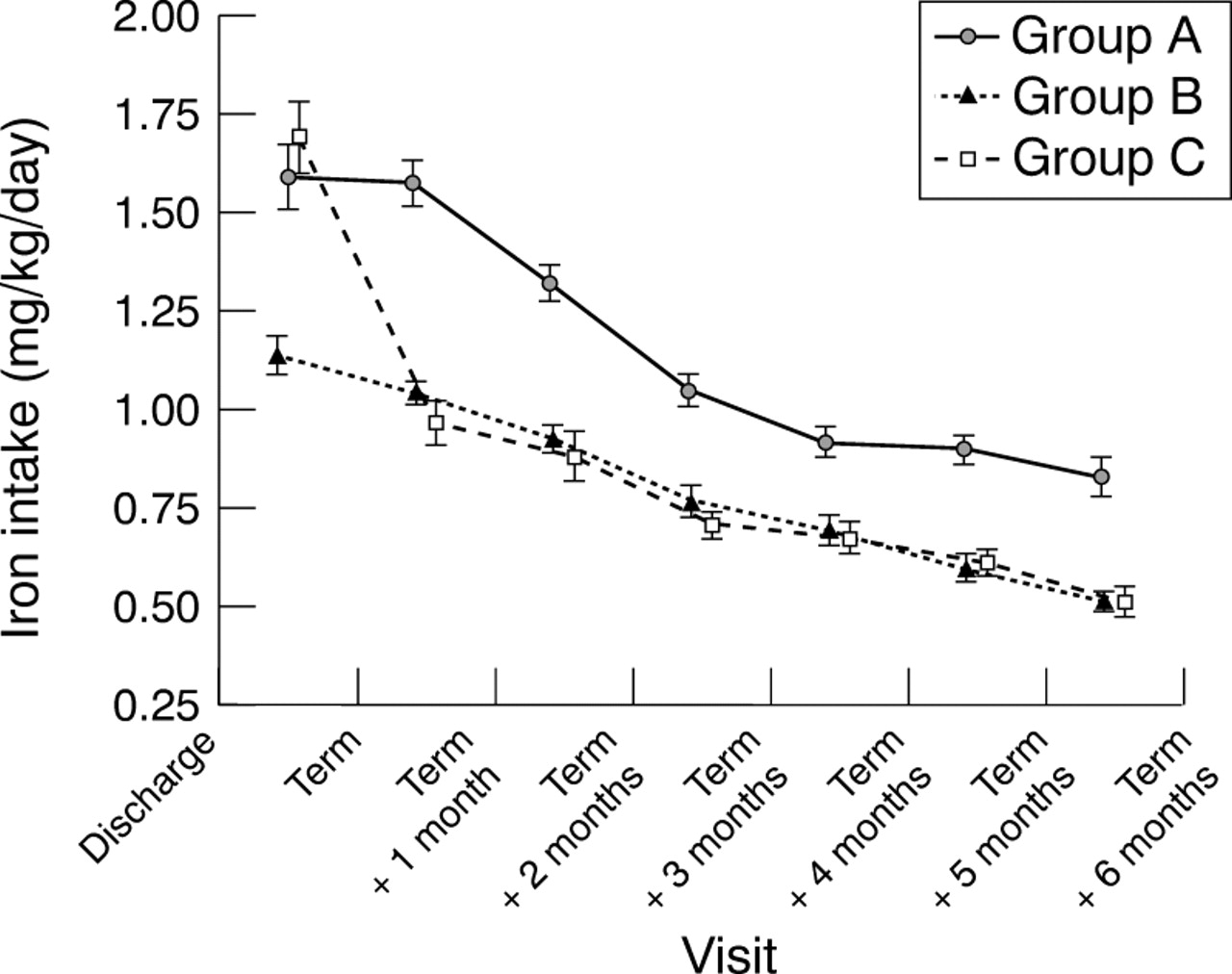
Mean iron intake (mg/kg/day) from formula for the three groups at each clinic visit. Error bars represent ± 1 SEM. If error bars are not visible, they are smaller than the symbol width.
A total of 677 of haemoglobin measurements were made. Haemoglobin concentrations of the study infants were compared with reference data for preterm infants of the same postnatal age5 and term infants of the same postmenstrual age13 (figs 2 and 3, respectively). In no instance was the haemoglobin concentration in study infants less than the lower limit of normal for reference preterm infants. At 1 month of corrected age about one third of study infants had a haemoglobin concentration below the lower limit of normal for term infants; by 2 months corrected age this had fallen to a single individual. After 2 months corrected age, study infants compared well with reference infants, and no infants were anaemic.
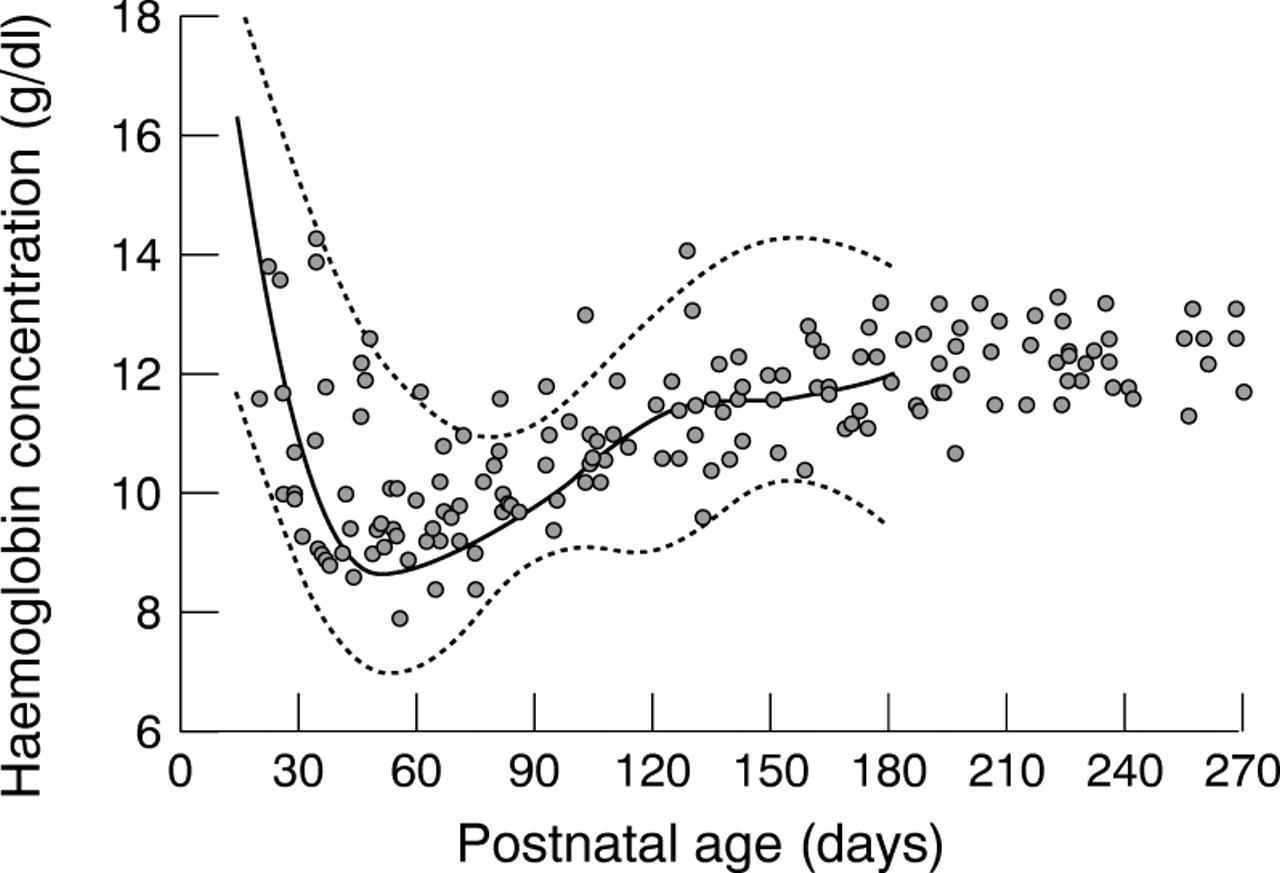
Haemoglobin concentration (g/dl) in study infants of birthweight 1–1.5 kg who were never transfused, compared with data (mean ± 2SD) for preterm infants of similar postnatal age.5
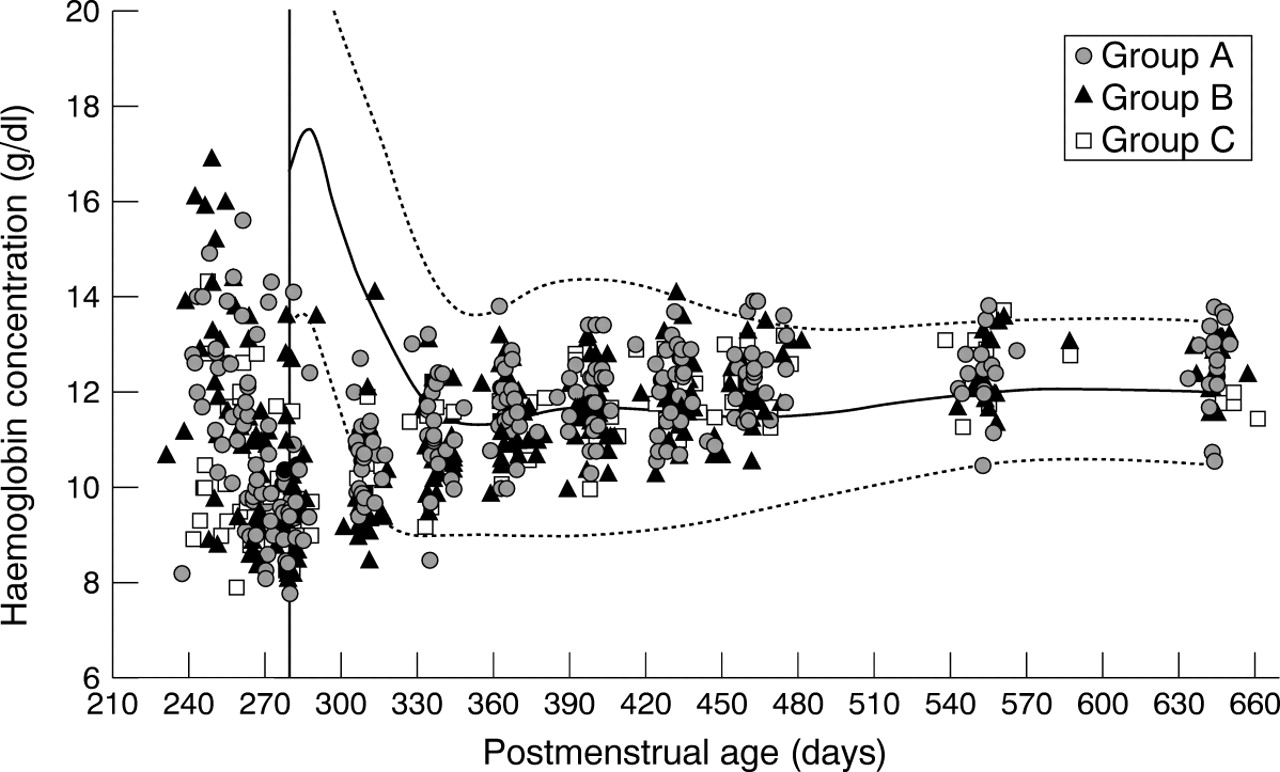
Haemoglobin concentration (g/dl) in study infants, compared with data (mean± 2SD) for term infants of similar postmenstrual age.13 Solid vertical line represents expected date of delivery (280 days of postmenstrual age).
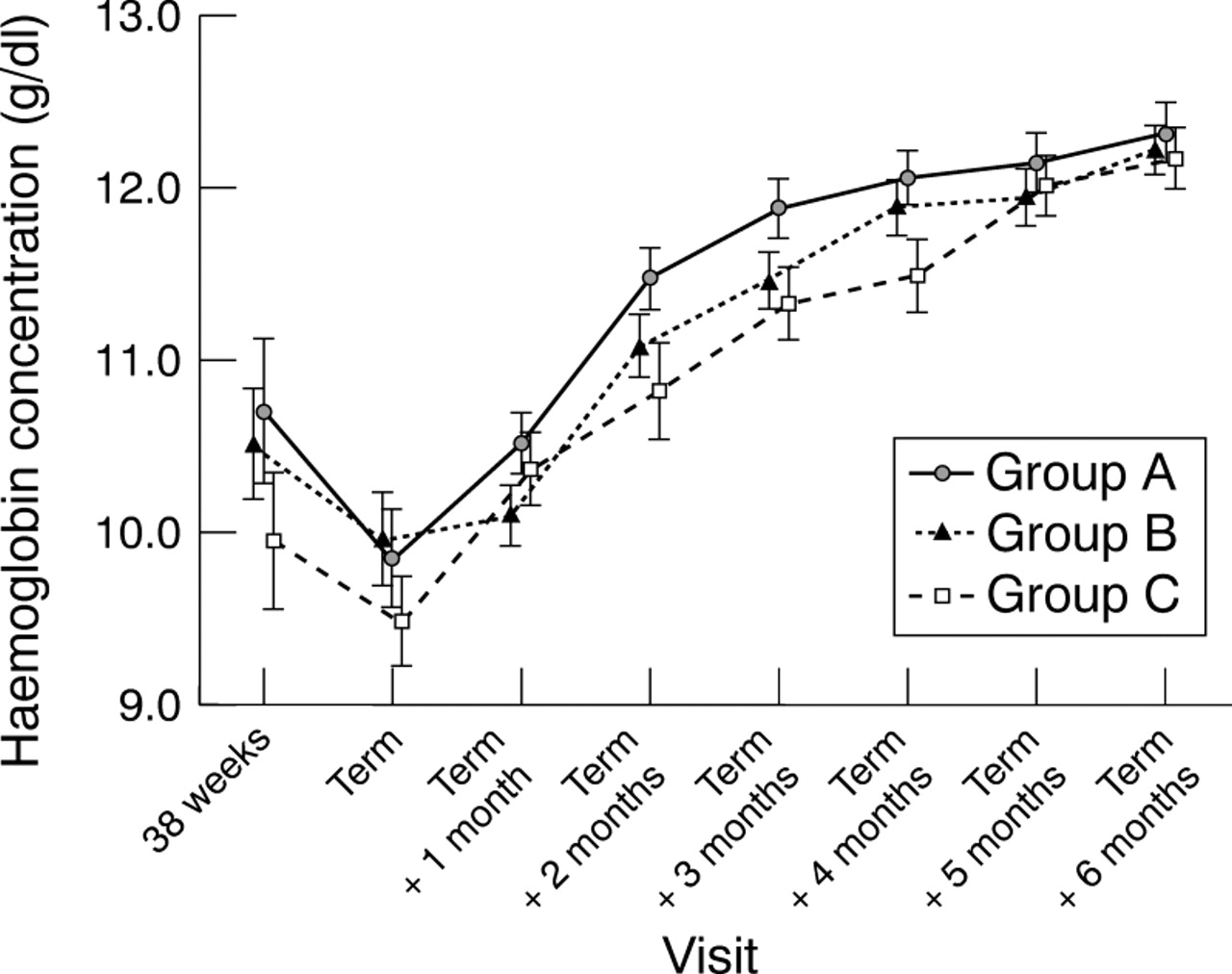
There was no significant difference in haemoglobin between the groups (ANOVA, p = 0.128) (fig 4). The analysis had a power of greater than 90% to detect a difference in haemoglobin concentration between groups of 0.5 g/dl, the smallest difference that we felt was clinically relevant. The data were also analysed using ANCOVA, with haemoglobin concentration at discharge as a covariant. Once again there were no differences among the groups (ANCOVA, p = 0.391).
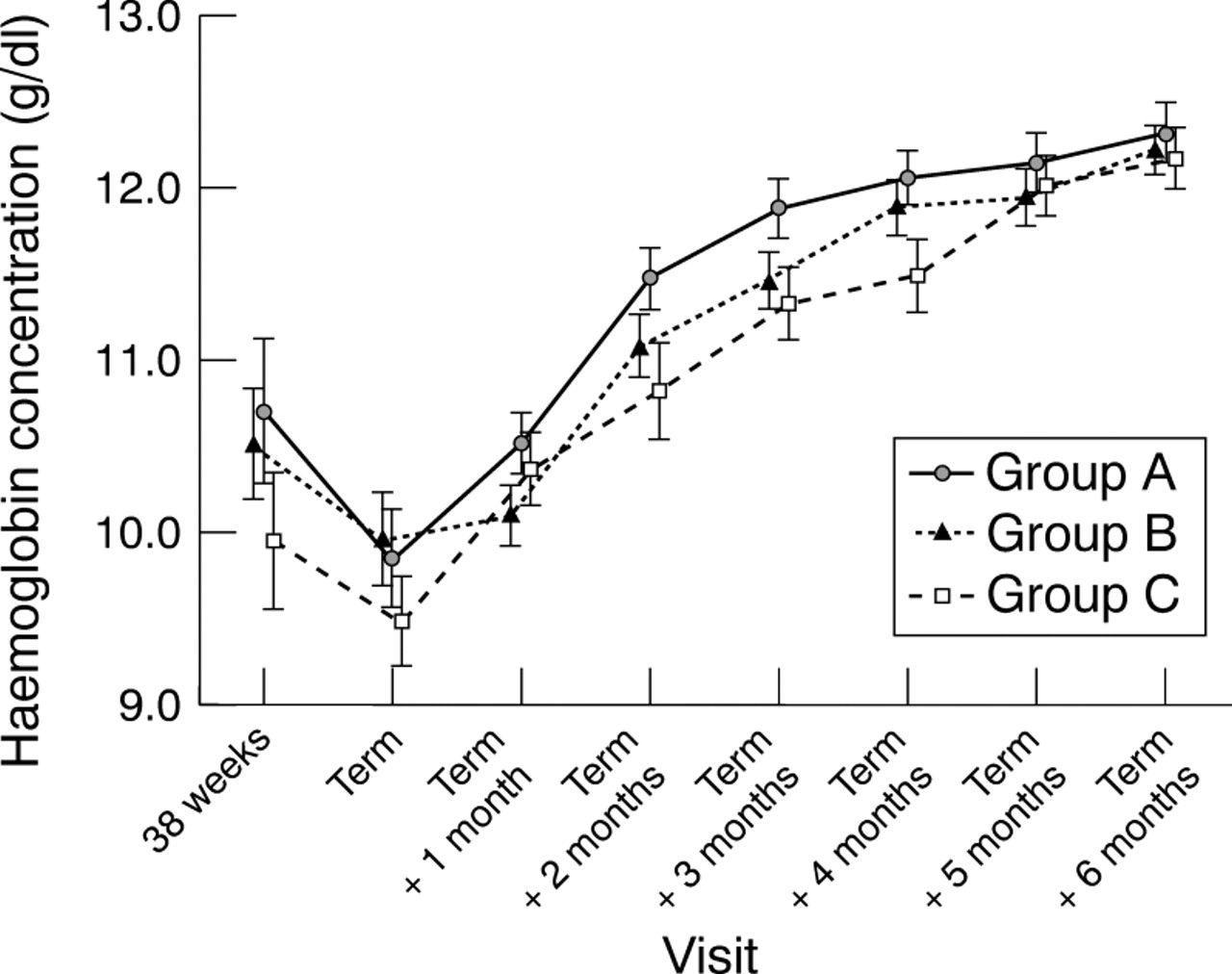
Mean haemoglobin concentration (g/dl) in three study groups at each clinic visit. Error bars represent ±1 SEM.
Haemoglobin concentration was 12.49 g/dl (SD 0.74) at 9 months corrected age (n=46, range 10.5 to 13.8 g/dl) and 12.47 g/dl (SD 0.75) at 12 months corrected age (n= 40, range 10.6 to 13.8 g/dl).
Two hundred and seventy two determinations of plasma ferritin were made in groups A and B. Multiple regression analysis showed that plasma ferritin was significantly related to postnatal age (p < 0.001), but not to postmenstrual age (p = 0.147). Figure 5 shows a scattergram of plasma ferritin for study infants against postnatal age. In 21 instances plasma ferritin was less than 10 μg/l, nine of 121 determinations (7.4 %) in group A, and 12 of 151 (7.9 %) in group B. The ferritin concentration was measured in 28 infants in group A; five (18%) were iron deficient on at least one occasion compared with eight out of 30 (27%) in group B (Fisher’s exact test, p =0.534). None of the iron deficient infants was anaemic. There was no difference in plasma ferritin between groups A and B (ANOVA p = 0.322).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Plasma ferritin for study groups against postnatal age. Solid horizontal line represents plasma ferritin concentration of 10 μg/l which suggests iron deficiency.
Before 4 months of postnatal age, only 2.5% of 121 ferritin measurements showed evidence of iron deficiency. This increased to 14.3% between 4 and 8 months (105 measurements) and 9.1% between 8 and 12 months (31 measurements). After 12 months of postnatal age none of 15 measurements showed evidence of iron deficiency. The geometric mean plasma ferritin at 9 months corrected age was 22.1 μg/l (n = 15, minimum 6 μg/l), and 40.9 μg/l at 12 months corrected age (n = 15, minimum 21 μg/l).
Discussion
It has been estimated that preterm infants need to absorb 0.8 mg/day iron to meet the requirement for growth during the first year of life.2 Current recommendations are that preterm infants receive 2 mg/kg/day of iron either as iron drops, or a formula containing 1.2 mg/dl iron.6 7 Randomised clinical trials had shown that such levels of supplementation effectively prevent the development of iron deficiency anaemia,5 15 with no benefit to be derived from higher levels of supplementation.16 17 Little information is available on the efficacy of lower levels of iron supplementation in preterm infants.
Our study suggests that a mean iron intake of about 1 mg/kg/day, and formulas containing 0.5–0.9 mg/dl iron, also prevent the development of iron deficiency anaemia in preterm infants. After the formulas were discontinued at 6 months corrected age there was no fall in haemoglobin concentration, which remained similar to those of infants born at term. Although the iron intake differed by 50% among the three groups, no differences in haemoglobin or ferritin concentrations were noted.
Current estimates of iron requirements assume that iron stores at birth are sufficient to meet the iron needs of preterm infants until 2 months of age. After this infants become dependent on dietary iron. Infants in this study were fed iron containing formulas throughout their hospital stay, possibly maintaining iron stores during the first two months and decreasing subsequent requirements.
It is also assumed that only 10% of dietary iron is absorbed.6 7 This is based on work in term infants18 which may not be applicable to preterm infants. Dauncey et al 19 measured iron absorption in preterm infants using nutrient balances and found that iron absorption averaged 34% of intake once iron supplements were started. Cooke et al measured iron absorption using nutrient balances in preterm infants receiving a formula providing 1 mg/kg/day iron. Iron absorption increased rapidly in early postnatal life from 12% (SD 19) at 4 weeks of postnatal age to 25% (SD 17) at 5 weeks.20 Preterm infants may therefore be able to absorb more than 10% of iron from their diet. If this is correct iron intakes less than those currently recommended could be expected to prevent iron deficiency anaemia.
Iron deficiency occurs in three phases: storage iron depletion, iron deficiency without anaemia, and iron deficiency anaemia. No infant in our study had iron deficiency anaemia. Iron deficiency (plasma ferritin < 10 μg/l) without anaemia was seen most commonly between 4 and 8 months of age where 14.3% of ferritin measurements revealed evidence of iron deficiency. This is similar to the preliminary data for low birthweight infants receiving higher levels of iron fortification (1.2 mg/dl or 2.1 mg/dl).17 In our study low ferritin concentrations corrected without intervention and did not progress to iron deficiency anaemia. This may reflect decreased iron requirements with increasing age, increasing iron intake from solid foods, or adaptation through increased iron absorption from the diet.
In term infants the mean haemoglobin concentration at 8 months of age is about 11.7 g/dl, with a geometric mean ferritin of 38.5 μg/l.21 These are similar to our values at 9 months corrected age (mean haemoglobin 12.5 g/dl, geometric mean ferritin 22.1 μg/l). Infants in our study therefore seem to have similar iron status to that of their peers born at term, by 8 to 9 months corrected age.
In Europe most formula fed preterm infants are discharged home on formulas containing 0.5–0.9 mg/dl iron, and additional iron needs to be given as drops to meet the current recommendations.9Compliance with medicinal iron is poor8 22and siblings are exposed to the risks of accidental ingestion of iron supplements.23 Concern also exists about the possible detrimental effects of excessive iron intake.24-28 Data from this study indicate that the use of iron fortified formulas containing 0.5–0.9 mg/dl prevented iron deficiency anaemia. The theoretical concerns about excess oral iron intake do not seem to be balanced by any detectable benefit.
Iron deficiency is, however, a serious health issue. Twelve per cent of British children aged 1.5 to 2 years have low haemoglobin concentrations, and 28% have low ferritin concentrations.29 30 In this age group iron deficiency anaemia may lead to developmental delays that do not respond to subsequent iron supplementation.31 Data from our study suggest that preterm infants fed formulas containing 0.5 mg/dl to 0.9 mg/dl iron had an iron status by the first year of life similar to that of their peers born at term.
This study should, however, be interpreted with caution and the findings may not be universally applicable. Iron status is affected by placental blood transfusion at birth, transfusion and phlebotomy practices in hospital, iron intake before hospital discharge, and growth rate of the infant.2 32 33 After discharge iron status is affected by iron intake from other dietary sources, and the intake of cow’s milk.34-36 These factors will vary, and iron status must be closely monitored in rapidly growing preterm infants.