Article Text

Abstract
AIMS To study the cardiac pathology of infants enrolled in the UK collaborative trial of neonatal ECMO (extra corporeal membrane oxygen) who died following random allocation to a trial arm.
METHODS During the trial, 81 infants died. The hearts of 26 babies were received and examined without knowledge of treatment regimen. The control group consisted of 14 infants who received conventional treatment. Twelve were allocated to ECMO; seven received this treatment.
RESULTS In the control group, four showed minor histological changes. The other hearts were histologically normal. In the group treated with ECMO, four had multiple foci of micro-infarction throughout both ventricles and papillary muscles. There was variable thrombotic vascular occlusion. Three were normal. There was no correlation between cardiac pathology and clinical features. There was a significant difference in the length of survival between the two groups.
CONCLUSIONS ECMO treatment seems to be associated with clinically significant cardiac pathology. The changes observed may reflect the longevity of survival in the ECMO group rather than an association with the treatment itself. Nevertheless, the findings have significant implications for those monitoring the development of infants surviving ECMO treatment and suggest that the monitoring of myocardial function will be crucial.
- ECMO
- cardiac pathology
Statistics from Altmetric.com
Extra corporeal membrane oxygenation (ECMO) can be used as a temporary supportive treatment in infants with severe respiratory or cardiac disease.1 It was first used successfully in an adult in 1972.2 In the UK an ECMO service was first established at Groby Road Hospital, Leicester, in 1989.3Four small randomised controlled trials of neonatal ECMO suggested reductions in mortality but the findings were not conclusive.4-7 Against this background, clinicians in the UK were reluctant to refer suitable infants for treatment because of concerns that any improved survival might be offset by high rates of long term disability. In view of this, all five ECMO centres in the UK agreed that ECMO would be offered only to newborn babies within a randomised controlled study. Between 1993 and 1995, 185 mature (gestational age 35 weeks, birthweight 2 kg) neonates with severe respiratory failure (oxygenation index 40) were enrolled from 55 hospitals in the randomised controlled trial of ECMOvs intensive conventional management. The trial was discontinued in 1995 on the advice of a data monitoring group as early results showed a clear advantage for ECMO.
Previous data had suggested that the myocardium would be particularly susceptible to the deleterious effects of reperfusion injury mediated by the production of free radicals.8 This in turn might cause diminished myocardial function or “myocardial stun,”9 a term currently used to denote extreme myocardial dysfunction in the presence of ischaemic damage. Within the confines of the UK trial it was decided to investigate whether myocardial ischaemia occurred more often in those infants receiving ECMO.
Methods
Patients were randomly allocated, according to published criteria.10 The ECMO centres followed an agreed protocol. Intensive conventional management was provided in the referring hospitals within trial guidelines. These guidelines included liberal use of oxygen, correction of acidosis, maintenance of adequate blood pressure, paralysis, and use of any available pulmonary vasodilators including nitric oxide (NO). The precise details of trial guidelines have been published elsewhere.10
When a death was notified to the coordinating centre, the clinician and pathologist at that centre were contacted to ascertain if a postmortem examination had been performed. If so, material was requested for further study. The preferred sample was the formalin fixed, complete heart. Failing this, formalin fixed tangential sections through both ventricles, to include papillary muscle, or representative paraffin wax embedded blocks, were requested. From the complete hearts or ventricles, blocks were cut at 3 mm intervals (veno-arterial valves to apex). Six sections were taken from each block and stained with haematoxylin and eosin (two sections), elastic Van Gieson, martius yellow-scarlet-blue, Masson trichrome and rhodamine light green. Selected sections were then stained with Von Kossa and Perls, if indicated. These sections were then examined microscopically to assess the presence of ischaemia, infarction, and vascular changes.
The tissue samples were examined blind. Clinical and histological data were correlated only after all trial material had been assessed.
Results
The results are summarised in tables 1 and 2. Following randomisation the infants in both arms were not significantly different in terms of descriptive data. The gestational age ranged from 35 to 42 weeks. Birthweights ranged from 2290 g to 4730 g and indices of disease severity at referral, as indicated by the oxygenation index, were not significantly different. No infant had received high pressure ventilation for longer than 10 days, in line with the trial guidelines. The principal diagnoses are as shown in tables 1 and 2. There was no significant difference in treatment administered after randomisation in terms of ventilation or use of vasodilators. Three infants in the ECMO group and two in the control group received nitric oxide (NO).
ECMO
Conventional management
Eleven infants were initially allocated to receive ECMO; seven received it. One infant was allocated to conventional treatment, but due to a mix up at the referring centre, was re-entered and received ECMO, and was subsequently included in the ECMO arm in this study. Five infants did not receive treatment, despite allocation, because of death before transport (n=2) or contraindications: intraventricular haemorrhage (n=1), complex congenital heart disease (n=1), and withdrawal of parental consent (n=1).
The tissue submitted varied, according to the referral centre; most submitted a single 3 mm section of the ventricles (n=12 with two of these including sections of atria); others submitted ventricular tissue of varying depth which was the sliced into 3 mm sections for study; 2 × 3 mm sections (n=7) 3× 3 mm sections (n=2, with one including a cross section of the atria), 4 × 3 mm sections (n=3) and whole hearts were received from two cases (one in the ECMO group and one in the conventional management group). The overall distribution of tissue submitted for pathological assessment was thus similar in the two study groups.
In the ECMO group, pathological features were identified in cases with limited sections (five cases) and in one case where the whole heart was submitted. In the conventional management group clinically significant pathology was identified only in the cases where the whole heart was submitted.
In the ECMO group, four had multiple foci of microinfarction, defined as areas of increased eosinophilia of myocytes, loss of nuclei, and infiltration by neutrophil polymorphs, throughout the left ventricle and papillary muscle (fig 1), with varying degrees of thrombotic vascular occlusion. In our laboratory we found that rhodamine light green was not useful in delineating early infarcts. Although it is difficult to be precise as to the age of infarcts in the neonatal period,11 it is generally accepted that, in contrast to adults, infiltration by neutrophil polymorphs is a relatively late event and occurs after 24 hours; thus all those infarcts showing polymorph infiltration are days old while those with fibrosis are somewhat older (fibrous tissue taking weeks to develop).
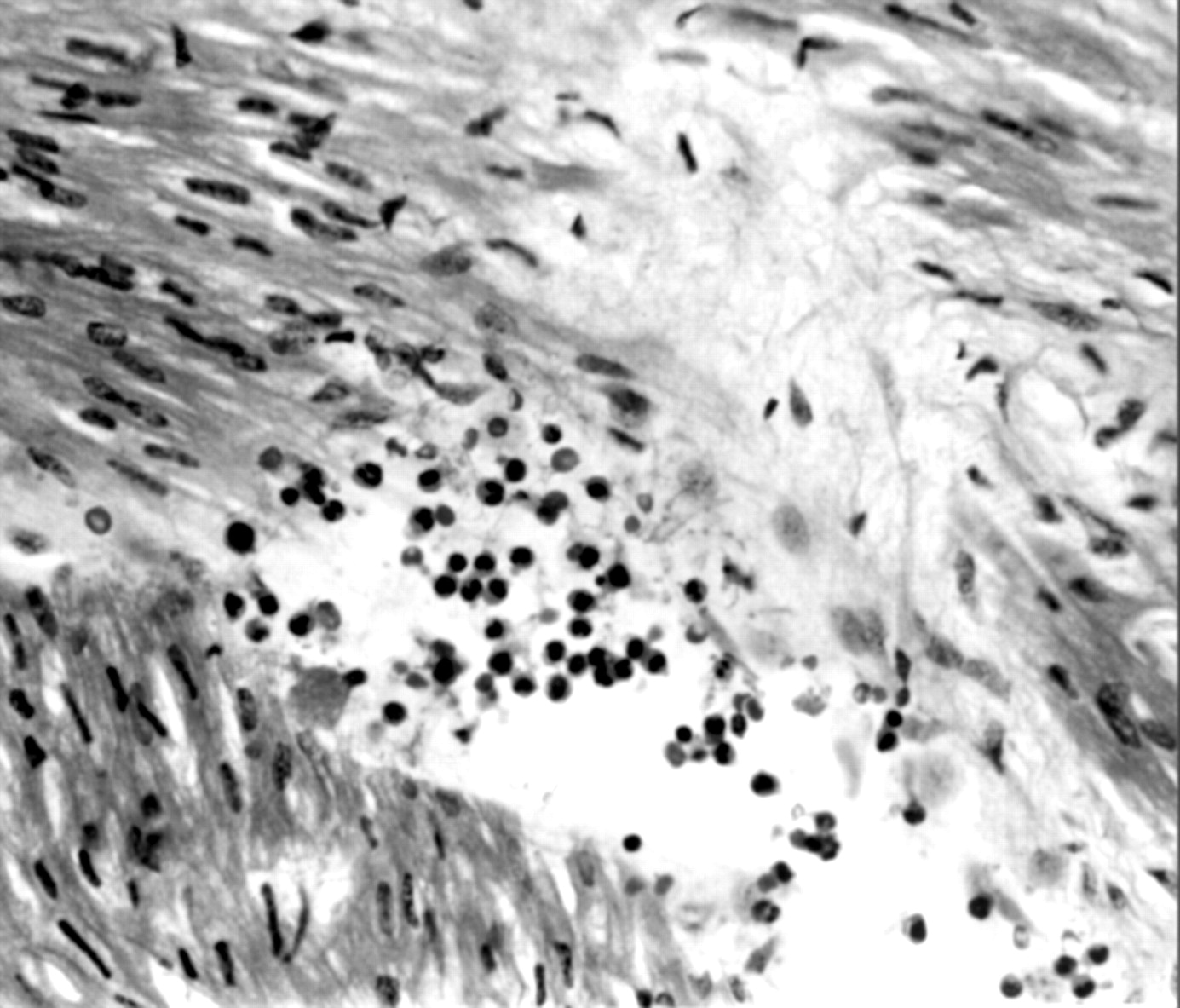
Case 9, showing focus of necrosis, loss of monocytes, and infiltration by neutrophil polymorphs.
There was fibrin and antemortem thrombus attached to the endothelial lining of the right atrium in one infant with a veno–arterial catheter (fig 2) and haemorrhage within the central zone of a papillary muscle in one infant.

Case 41, showing fibrin and antemortem thrombus attached to the right atrial wall.
Those not receiving ECMO despite randomisation displayed no abnormality of the ventricle or papillary muscles, although there was fibrin and antemortem thrombus attached to the endothelial lining of the right atrium in one infant with no history of arterial catheterisation. Diffuse calcification was present throughout the ventricle in the infant with uncorrected total anomalous pulmonary venous drainage (survival time 201 days) (fig 3) and interventricular septal haemorrhage in the infant in whom ECMO was contraindicated owing to intracranial haemorrhage. There was no significant difference between these two groups and thus no clinical features which might predict susceptibility to injury.

{kind=link}
{kind=link}
{kind=link}
Case 93, showing extensive calcification of ventricular wall.
Within the control group there were no significant pathological features in 10 infants and mild myocardial oedema in four.
There was a significant difference in the length of survival between the two treatment groups. The ECMO group, as a whole, survived an average of 43.5 days, with those that actually received ECMO surviving an average of 45 days, and those who did not receive ECMO surviving, on average, 41 days (time ranging from 7 hours 15 minutes to 201 days). The control group survived an average of 7.4 days.
Discussion
Over the years several studies have documented several different complications of ECMO treatment. These include cerebral, cortical, and cerebellar haemorrhage and thromboembolism. Intracranial haemorrhage was initially described by Cilley et al 12 in 10 patients, following a retrospective study of 35 neonates treated with ECMO. This complication was observed primarily in those neonates of less than 35 weeks of gestation. In view of this it was suggested that ECMO was contraindicated in infants of less than 35 weeks gestation. However, a further study13again noted that haemorrhage remained a problem in neonates greater than 34 weeks of gestation, as evidenced by follow up cranial computed tomography of 100 consecutive infants treated with ECMO. Bleeding was considered severe in 12% with large parenchymal haemorrhages and infarcts, cerebellar haemorrhages, and diffuse oedema; these complications have a 50% mortality. However, not all these data were corroborated by postmortem examination studies. Cerebellar haemorrhages featured in an earlier study, with four out of 12 infants showing cerebellar pathology,14 although it should be noted that these infants were extremely acidotic before treatment. These results must be set against the study of Andrews et al 15 which looked at the neurodevelopmental outcome of ECMO survivors and showed that most (71%) had developed normally when assessed at 3 years. Notably, all infants in their study were older than 34 weeks gestation, confirming the findings of Cilley in his original study. Despite the fact that many authors12 15have suggested that carotid artery ligation and dilution with heparin contributed to the development of intracranial haemorrhage, Weber16 noted that intracranial haemorrhage was a particular problem in infants who were more acidotic, smaller for gestational age, and hypotensive before ECMO. The advantage of this study was the ability to correlate a number of clinical features with pathological outcome.
Other studies have concentrated on other types of complication, such as thromboemboli in response to a perceived clinical problem—iatrogenic injury, air or foreign body type emboli, for example.17 In this postmortem examination study of 23 infants treated with ECMO, 22 had thromboemboli, with 12 of these showing emboli containing aluminium. These emboli seemed to be related to the presence of friable aluminium concretions adhering to the heat exchangers, and following the findings of this study the circuitry used was extensively modified. The use of moderate amounts of heparin to effect anticoagulation has greatly diminished the incidence of thrombo-embolic phenomena though it was seen in four out of 12 neonates in our earlier study14(in two of these it related to endothelial damage at the site of cannulation).
Previous studies have tended to concentrate on the cerebral complications and there are few published data on the cardiac pathology in this group of patients. A recent series18 investigated cardiac changes in ECMO non-survivors (n=20) compared with an age matched control group (n=8). They found significant haemorrhage in the right atrium, sino-atrial, and atrioventricular nodes, right ventricle and endomyocardium of the left ventricle. Only one heart in this group was normal compared with all the hearts in the control group. It is unclear from the data presented as to the precise characteristics of the control group. Clearly, this is important when comparing such lesions and attempting to attribute the changes to a particular treatment.
The great benefit of the UK collaborative randomised trial was the large number of infants recruited, the availability of a control group, and access to clinical data. In this study we concentrated on cardiovascular changes. The results of this study suggest that ECMO is associated with clinically significant cardiac pathology in the form of microinfarcts scattered throughout the ventricular wall and involving papillary muscle, but in none of these cases was the infarction associated with emboli. A previous study had indicated similar changes but lacked the benefit of a control group.14
Many studies have emphasised the difficulties of attempting to age myocardial infarction in neonates, but the histological appearance of all hearts in this study suggested that the injuries were longstanding—in the order of weeks—with areas of myofibre necrosis, deposition of loose fibrous tissue, and foci of calcification. Three of the hearts had additional foci which were suggestive of more recent injury with neutrophil polymorph infiltration (probably >24 hours duration). In this context it is important to note the prolonged survival time of those that received ECMO. As the observed infarcts are old they probably developed during the period of ECMO treatment. The damage may arise secondary to reperfusion injury, mediated by liberation of oxygen free radicals. Infants who are acidotic, hypotensive, and poorly perfused might be at risk of widespread free radical production during reperfusion. This mechanism has been implicated in the aetiology of “myocardial stun”9 and importantly, none of this group showed compromise during treatment. All the infants, however, received inotropic support during ECMO and so the effects of “myocardial stun” may have been masked by the ECMO itself.
If we accept “reperfusion injury” as a possible mechanism for myocardial damage, we might anticipate differences between the two modes of cannulation. Veno-venous and veno-arterial cannulation differ in their impact on the myocardial circulation, haemodynamics, and oxygen delivery. Veno-arterial cannulation at high flow rates reduces the pulsatility of the systemic circulation and creates high arterial oxygen tensions, whereas veno-venous cannulation raises the mixed venous oxygen content and, in the face of negligible pulmonary function, perfuses the patient with pulsatile flow at a lower oxygen tension. Systemic oxygen delivery is assured by a compensatory rise in native cardiac output. Myocardial perfusion is probably best during veno-venous flow, as there is evidence to suggest that coronary blood flow is still largely derived from pulmonary venous return, irrespective of cannulation.19 The oxygen tension of this blood is highest during veno-venous perfusion. In view of this it is interesting to note that there was no clinical correlation between mode of cannulation and cardiac pathology although the numbers are too small to permit statistical analysis.
It is important to note that despite the limited sampling of hearts which may have compromised the study, the conventional management group and the ECMO group had a similar distribution of whole hearts and limited ventricular sections available for study. It is therefore significant that the ECMO group showed greater pathology in the form of microinfarcts. Indeed, this may be an underestimate of the problems caused, owing to the limited material submitted.
As ECMO involves the use of heparin, it might be expected that complications related to haemorrhage may arise. In this study only one infant receiving ECMO showed papillary muscle haemorrhage. This is in sharp contrast to a series where haemorrhage was the most frequently observed pathological change along with extensive necrosis.18 Right atrial haemorrhage occurred in 17 out of 20 cases with left ventricular haemorrhage occurring in nine. As in our study, the authors observed one case of right atrial thrombus. Unfortunately, they included no details of survival times. Weber also drew attention to haemorrhage as a potentially serious complication of ECMO treatment but included few data relating to cardiac lesions.16 In none of our patients was there any evidence of foreign body emboli or other types of iatrogenic injury, in sharp contrast to the findings of Vogler.17
Addendum
The findings of this study are important for those clinicians involved in the ongoing management of infants surviving ECMO therapy. The UK trial showed the clear benefit of ECMO in the treatment of certain conditions, but if we are to extrapolate from the results shown here, cardiac function may be compromised in the survivors. Disappointingly, few hearts were received (<50%), but despite this, the results of this randomised trial show that pathology has much to contribute to the clinical evaluation of modern treatment options. Future therapeutic trials should include pathological assessment.
Acknowledgments
We thank all those who participated in the UK Collaborative ECMO trial without whom this study would not have been possible.