Article Text

Abstract
AIMS To compare arterial blood gas (ABG) readings obtained with a multiparameter intra-arterial sensor with those from an ABG analyser.
METHODS An MPIAS with the ability to measure continuously pH, PaCO2, and PaO2 was introduced via an umbilical arterial catheter in 27 neonates requiring intensive care. They underwent 3260 hours of MPIAS monitoring, during which 753 ABG readings were performed.
RESULTS Overall bias (mean difference: MPIAS–ABG) and precision (standard deviation of differences) values were: −0.002 and 0.022, respectively, for pH; +0.26 and 0.52 for PaCO2 (kPa); and −0.19 and 0.99 for PaO2 (kPa). This gave 95% limits of agreement as: −0.047 to +0.042 for pH, −0.76 to +1.28 kPa for PaCO2, and −2.13 to +1.75 kPa for PaO2. For each variable, precision across readings from the same individual was better than overall precision for all data. No complications related to the use of the catheter were observed.
CONCLUSIONS Continuous MPIAS ABG monitoring is an exciting development, with the potential to reduce blood transfusions and improve ABG homeostasis.
- blood gas monitoring
- multiparameter intra-arterial sensor
Statistics from Altmetric.com
Blood gas monitoring is an essential part of neonatal intensive care, its primary aim being to maintain arterial blood gas homeostasis, with particular emphasis on avoiding large peturbations. Currently this is achieved using information obtained from intermittent arterial blood gas (ABG) analysis. This is still the gold standard in terms of accuracy and precision. Clinical usefulness is limited because ABG analysis is performed intermittently, with a frequency determined by either clinical condition or local neonatal intensive care practice. It is well known that even in stable intensive care patients sudden variations can occur. There are, therefore, potential clinical benefits in continuous ABG monitoring.
The need for continuous ABG monitoring has been addressed by the introduction of a number of non-invasive, indirect methods. In particular, transcutaneous CO2 and pulse oximetry are now part of routine neonatal intensive care monitoring. Unfortunately, transcutaneous monitoring requires frequent resiting and/or recalibration of the probe and is least reliable in the sickest infants.1 The limitations of information from pulse oximetry have been well described.2 3
Continuous intra-arterial PaO2 monitoring has been possible for more than two decades using an umbilical arterial catheter with a Clark electrode.4 These catheters are highly reliable, although accuracy does deteriorate with deposition of blood and protein on the catheter tip.4 5 More recently, continuous monitoring of intra-arterial pH, PaCO2, and PaO2 in paediatric and adult intensive care patients has become available6 7 using a multiparameter intra-arterial sensor (MPIAS), placed in a peripheral artery. An MPIAS has now been developed using new technology that allows it to be passed through an umbilical arterial catheter. We report the first evaluation of the Neotrend (Diametrics Medical Ltd, High Wycombe, UK) in newborn infants receiving intensive care.
We aimed to: compare the measurements of pH, pCO2, and pO2 from the MPIAS with those from the blood gas analyser; calculate bias and precision for each variable for the whole group and individual patients; and characterise the type, incidence, and severity of complications associated with the use of the Neotrend MPIAS.
Methods
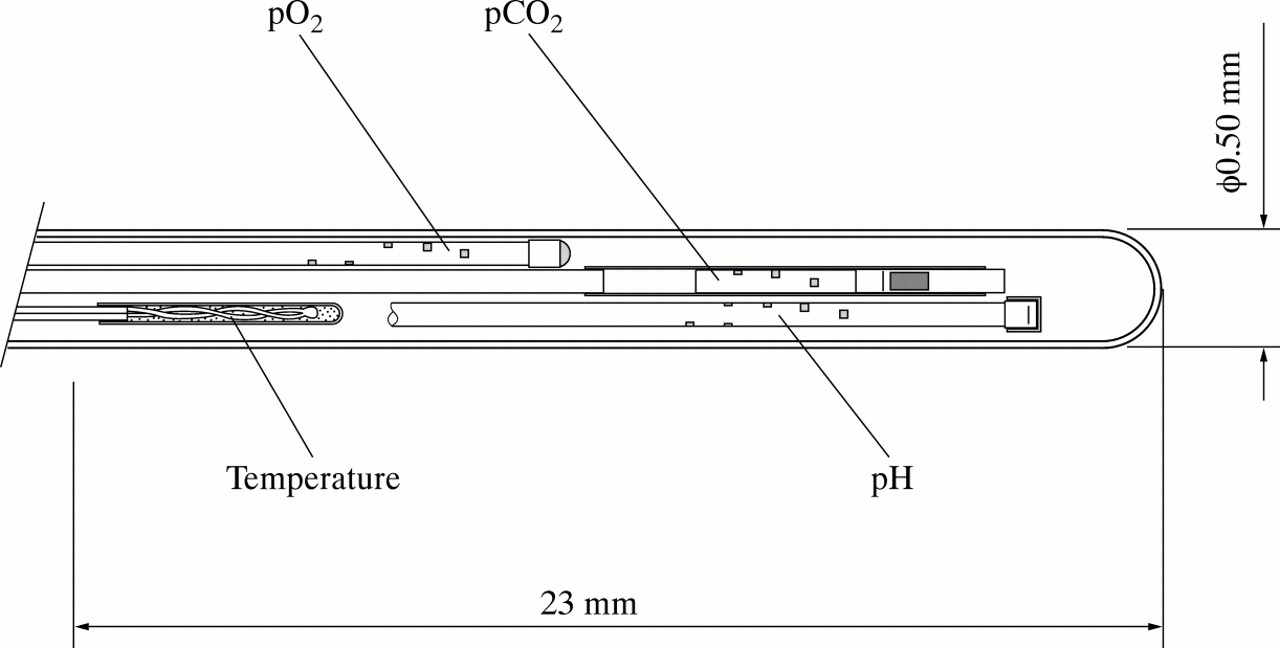
The Neotrend MPIAS has three optical sensors made of 175 μm polymethylmethacrylate fibres with radial holes drilled through the fibres (at the tip) to allow the appropriate indicators to be placed in the optical pathway (fig 1). A signal light beam is sent down the optic fibres. A stainless steel mirror is encapsulated within the end of each fibre. This reflects the altered light beam back along the optic fibre to the detectors. This arrangement effectively means that each fibre represents a miniature spectrophotometer.

Schematic of distal 23 mm of MPIAS, showing location of individual pH, PaCO2, and PaO2 sensors and thermocouple.
The design of the individual sensors is now described in brief. The holes in the pH sensor are filled with polyacrylamide gel containing immobilised phenol red dye. The dye changes colour (reversibly) in response to the concentration of hydrogen ions. By measuring the absorbency of green light by the red dye, the pH can be measured. The PaCO2 sensor is similar. The holes in the PaCO2sensor are enclosed within a gas only permeable membrane. Encapsulated within, is a bicarbonate solution containing phenol red dye as an indicator. CO2 diffuses across the membrane and alters the pH of the solution. The PaO2 sensor contains an entrapped fluorescent ruthenium based dye in a silicon rubber matrix. Blue light is absorbed by the fluorescent dye and emitted as light of a different wavelength. The emitted light intensity is altered by the presence of oxygen, allowing the PaO2 to be calculated. The three individual sensors are assembled with a T-type thermocouple to form the combined sensor bundle of the MPIAS (fig 1). All four components are contained within a microporous polyethylene outer sheath. The pores in the surface are filled with polyacrylamide gel, continuous with the gel of the individual sensors. The outer surface of the sheath is coated with covalently bound active heparin. The outer diameter of the MPIAS is 0.5 mm.
The MPIAS is sealed within a device to allow its introduction into the umbilical arterial catheter lumen. The Sensor Introduction System (SIS) consists of a sliding mechanism to introduce the sensor in and out of a sealed cable. At the distal end is a Y-connector. An “O-ring” seal, through which the sensor is introduced, prevents bleeding back when connecting to the umbilical arterial catheter. Improvement in the SIS and arterial catheter design continued during the study. SIS from five different batches were used in this group of patients. Each batch was modified according to clinical experience with the previous batch. These changes were implemented to facilitate clinical use and improve the method used to pass the sensor down the lumen of the umbilical arterial catheter. No modifications were made to the MPIAS itself. The problems encountered related to non-uniformity of umbilical arterial catheter length and difficulty in threading the sensor through the O-ring (resulting in sensor damage, usually to the thermocouple). The rate of successful MPIAS insertion was considerably improved in subsequent batches.
The calibration procedure is automated and lasts 35 minutes. Each MPIAS is provided with its tip in a tonometer containing buffer solution. During calibration, sterile mixtures of gases with known concentrations of CO2 and O2 are passed through the solution. With simultaneous measurement of the barometric pressure, the concentration of CO2 and O2, as well as pH, can be changed. The signals from the individual sensors are recorded and used to generate equations that predict the response of the sensor signals to changes in analyte concentration. These are stored within the patient data module.
The MPIAS and calibrated module are transferred to the display monitor at the cotside. The MPIAS is then connected to, and passed down, the umbilical arterial catheter. The tip of the sensor lies 23 mm distal to the catheter tip. This ensures that the active tip of all four individual sensor components sit in arterial blood within the lumen of the descending aorta. The clinical monitor graphically displays the change in blood gases together with aortic temperature continuously over time. Current blood gas status is digitally displayed along with temperature and calculated values for base excess, bicarbonate and oxygen saturation. The monitor can be adjusted to show up to 24 hours of data.
Local hospital ethics committee approval was obtained at all centres. Patients were recruited at St James’s University Hospital, Leeds, All Saint’s Hospital, Chatham, and Addenbrooke’s Hospital, Cambridge. Informed consent was obtained before sensor placement. All patients admitted to neonatal intensive care and requiring an umbilical arterial catheter were eligible for study. The study was designed as a prospective trial with sequential patient enrolment. Only patients with more than 24 hours of continuous monitoring and over 10 complete datasets were eligible for analysis. A complete dataset consists of pH, PaCO2, and PaO2.
Umbilical arterial catheters (4F) were placed at the level T10. The Neotrend MPIAS was then calibrated and inserted. Time was then allowed for the MPIAS to adapt from reading the calibration solution to displaying stable ABG values (less than 5 minutes). Stable ABG was confirmed by the presence of tick symbols above each digital display before collecting data. It was established that all four components of the MPIAS tip were distal to the catheter tip and reading ABG (and not umbilical arterial catheter flush), by sampling the catheter. Displayed values should remain stable during ABG sampling. Each time an ABG sample was taken for analysis, a hard copy of the current Neotrend MPIAS clinical display was printed. The ABG samples were analysed using a Radiometer 510 (SJUH), Ciba Corning 565 (ASH), or Chiron Diagnostics 865 (AH) blood gas analysers. The ABG and Neotrend printouts were then collected. Complete datasets (pH, PaCO2, and PaO2) for both methods at each sampling time were retained for analysis.
The indwelling MPIAS can be recalibrated on the basis of any ABG result. Such calibrations were kept to a minimum. Recalibrations only took place where there was either a large offset in one or more variables from insertion, or there was evidence of progressive and consistent drift over the previous 24 hours. All such recalibrations were documented. The study was concluded in each patient when either the umbilical arterial catheter was no longer required clinically or when removal was clinically indicated. The reasons for removal were recorded.
The terms bias and precision are used throughout, and are defined as:
-
bias: mean difference between MPIAS and ABG readings (for each variable)
-
precision: standard deviation of the differences between MPIAS and ABG readings.
Bland and Altman plots8 were prepared for each variable, for combined patient data. This enabled calculation of overall bias (mean difference: MPIAS–ABG) and precision (standard deviation of differences). Individual patient data were analysed using bias/precision plots of individual patients for each variable.
Results
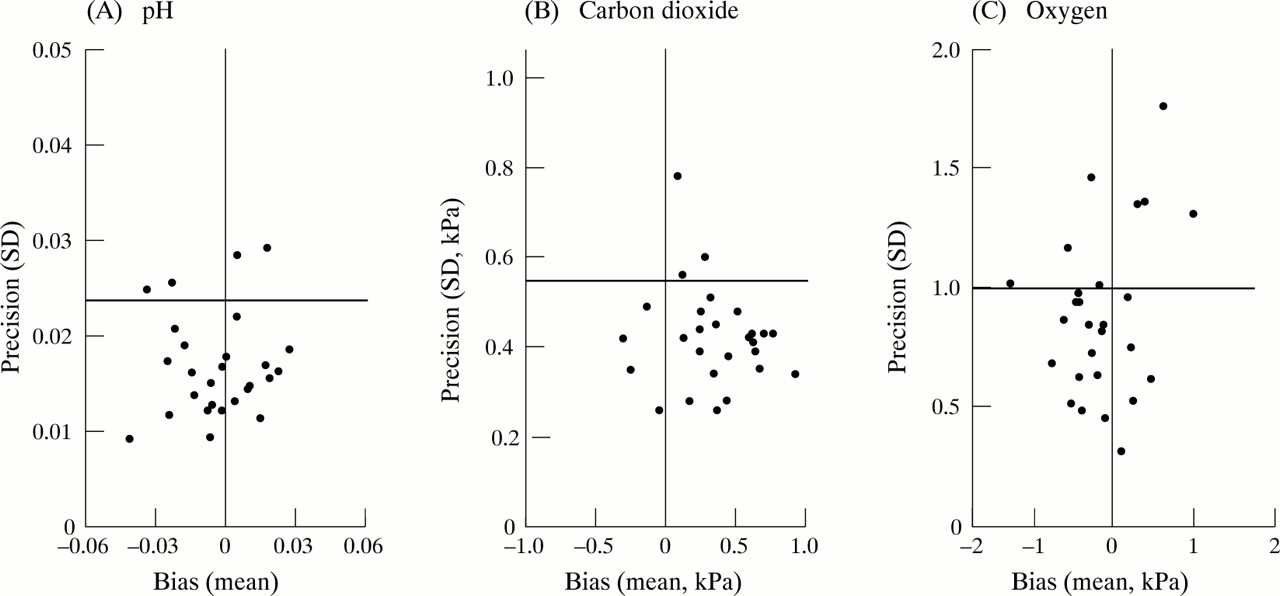
Data were analysed from all 27 patients (14 girls) successfully monitored in the three study centres. Median (range) birthweight and gestation were 1170 (560–3200) g and 28 (24–40) weeks, respectively. Median (range) time for MPIAS monitoring was 93.9 (24.1–428.8) hours. Nine patients were monitored for more than 7 days. Median (range) of complete datasets per patient was 25 (12–75). There was a total of 3260 hours of monitoring time, generating 753 complete datasets. Bland and Altman analyses8 were performed on the data from all patients. Bland and Altman plots are shown for pH (fig 2A), PaCO2 (fig 2B), and PaO2 (fig 2C). Overall bias (mean difference: MPIAS–ABG) and precision (standard deviation of differences) for pH, PaCO2, and PaO2 are shown in table 1.

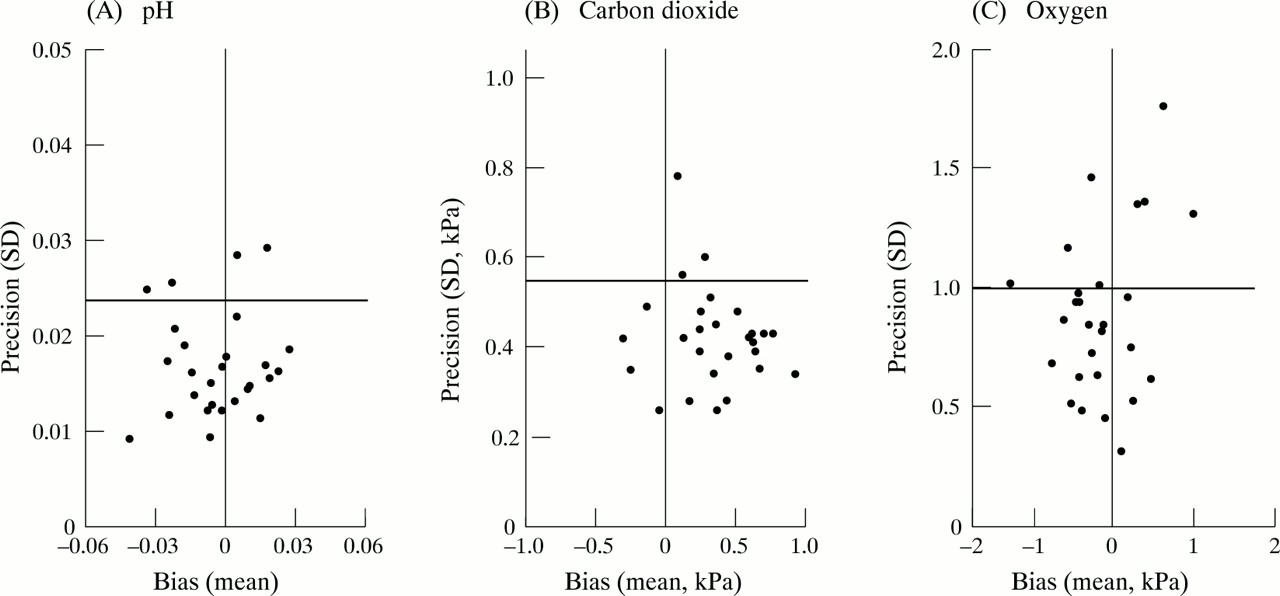
Bland and Altman plots for combined data, for each variable. Overall bias is shown as bold horizontal line. 95% upper and lower limits of agreement are shown as thinner horizontal lines.
Overall bias (mean difference: MPIAS-ABG) and precision (standard deviation of differences) values for each variable; LLA: 95% lower limit of agreement. ULA:95% upper limit of agreement
There was a tendency for the MPIAS to over read the PaCO2. Indeed, the bias was positive in 23 out of 27 patients, although the range of mean bias for individual patients was −0.3 to +1.0 kPa. This wide range in bias is apparent for the other variables and has an important effect on interpreting overall precision values when data from different patients are combined. This is of particular significance in continuous ABG monitoring, where bias can be reduced or eliminated by recalibration against a true ABG and trend analysis is clinically important. To address this difficulty in interpreting the overall precision figure, we have produced bias/precision data for individual patients. These are shown for pH (fig 3A), PaCO2(fig 3B), and PaO2 (fig 3C). For each variable, the precision value for most individual patients is below that of the overall precision figure: pH (23 patients), PaCO2 (24 patients), and PaO2 (19 patients). This clearly shows that precision is much better within individual patients than in the overall data, for all three measurements.
{kind=link}
{kind=link}
{kind=link}
Bias/precision plots for 27 patients, for each variable. Overall precision (1 SD) for each variable is shown as bold horizontal line.
Recalibrations were kept to a minimum: 17 patients did not require any recalibration. The variables recalibrated in the remaining 10 patients were: pH (four patients), PaCO2 (five patients), and PaO2 (eight patients). All were single recalibrations. Thus a total of 17 recalibrations (any variable) were made over 3280 hours of monitoring. This indicates that there was a minimal tendency for the MPIAS to drift with time. The most common scenarios leading to a need for calibration were: a drift down in PaO2 over the first 24 hours (then stopping) or a very slow drift up in PaCO2after 5 to 7 days of monitoring. Clearly, these were not consistent findings and affected only a few patients.
Any adverse events during monitoring were recorded, as were the reasons for removal of the umbilical arterial catheter. No problems with blood pressure transducer monitoring were observed and there was no damping of the trace with the current SIS design. In 16 patients the catheter was removed because it was no longer required; in eight the catheter stopped sampling. Two patients died because of severe lung disease. The remaining patient had the catheter removed after 25 hours because of haematuria. This was related to Escherichia coli septicaemia, disseminated intravascular coagulation (DIC), and a catheter that had migrated from T10 to L1 onx-ray picture. Renal and Doppler ultrasonography remained normal and the patient made a complete recovery. One patient (24 weeks gestation, 770 g) had an extremely difficult delivery, with cord prolapse and the need for rotation before assisted breech delivery. Examination of the placenta revealed a large retro-placental clot. At delivery there was a severe metabolic acidosis. She was very ill with evidence of a coagulopathy. This infant developed signs of paraplegia. Magnetic resonance imaging revealed three areas of spinal cord haemorrhage between the mid thoracic and lumbar regions consistent with trauma rather than vascular accident. This was confirmed by an independent neurological and neuroradiological opinion.
During the trial, a further 19 patients underwent attempts to insert an MPIAS. The rate of successful placement was specificallynot an aim of this study, because it was anticipated that the SIS would require modification when clinical use started. We have reported it because it is clearly clinically important. In 11 patients the insertion was either unsuccessful (n=8) or resulted in an incorrectly placed sensor (n=3). As indicated in the methods, this did not result from difficulties in passing the MPIAS down the lumen of the umbilical arterial catheter, but related to difficulties with the seal mechanism (O ring) between the catheter and the SIS. The proportion of successful insertions increased as the SIS was modified. In the remaining eight patients the catheter had to be removed before generating enough data (all underwent two or more ABG samples). This group included patients who developed transient lower limb duskiness (n=2), or who had catheters that stopped sampling (n=2), or were no longer required (4 samples). No other complications were seen in this group.
Discussion
There are several reasons why continuous ABG monitoring in neonatal intensive care may be clinically beneficial. The effects of changes in PaCO2 on cerebral blood flow in preterm infants have been well described.9 Both hypercapnia and hypocarbia are associated with the development of intraventricular haemorrhage and periventricular leucomalacia.10-13 Therefore, in preterm infants PaCO2 has to be kept within strict limits, particularly in the first 72 hours of intensive care. The need to avoid hyperoxia as well as hypoxia has similar implications for PaO2. Moreover, rapid changes in ABG can occur after surfactant administration, especially natural surfactants,14 and during high frequency oscillatory ventilation. Indeed, some workers have suggested patients receiving the latter should always have continuous PCO2monitoring.15
The Neotrend MPIAS provides pH sensor readings that agree closely with those of ABG analysis, with negligible bias and good precision. The PaCO2 sensor showed positive bias in most individuals with acceptable precision. Finally, the PaO2 sensor showed an inconsistent bias with acceptable precision. The fourth variable, aortic temperature, was not studied, as there is no standard for comparison available, although it is a potentially useful clinical indicator in sepsis. The biases shown for individual sensors are similar to the pattern reported for the Paratrend MPIAS in adult1 16 17 and paediatric7 intensive care patients. However, the precision is better than demonstrated in most of these studies, particularly for PaO2. This is partly because the earlier Paratrend sensor monitored the PaO2with a Clark electrode. Furthermore, there are difficulties with peripheral arterial lines because of artefacts resulting from limb movement and changing blood flow.16 The neonatal descending aorta does not create these difficulties.
It is also important to consider the precision of ABG analysers. A recent study18 found negligible variation within instruments, where precision (SD of the differences) values of 0.03 and 0.06 kPa were reported for PaCO2 and PaO2, respectively. Comparison of 10 different analysers gave precision values of 0.13 and 0.18 kPa for PaCO2 and PaO2, respectively, although the full clinical range of PaCO2 and PaO2 values was not tested. Other comparisons between two ABG analysers, using the whole ABG range, have shown less precision, with 0.011, 0.18, and 2.8 kPa reported for pH, PaCO2, and PaO2, respectively.19 These figures are similar to those found for portable ABG analysers, although PaCO2 precision varied from 0.26–0.48 kPa in recent studies.19-21
Clearly, it is useful to consider the variation between two ABG analysers (two gold standards) when interpreting the ABG analyser/Neotrend MPIAS precision figures. The level of overall precision for the Neotrend MPIAS is not sufficient to eliminate the need for ABG sampling. Nevertheless, the precision of the MPIAS will considerably reduce the frequency of ABG sampling and therefore the need for blood transfusion. Our clinical experience also suggests that MPIAS monitoring facilitates earlier detection of endotracheal tube obstruction and pneumothorax than current monitoring methods. Similarly, MPIAS monitoring seemed to have beneficial effects on the speed of ventilator weaning and the avoidance/reduction of periods of hypo/hypercapnia. Such anecdotal findings point to the need for controlled trials to assess both the potential short and long term benefits.
MPIAS monitoring also has to be considered in the light of non-invasive alternative techniques. Clearly, non-invasive methods of continuous monitoring are still appropriate in infants in whom umbilical arterial catheter insertion is unsuccessful or not clinically indicated. However, MPIAS monitoring is a highly attractive option in those who do merit a catheter. Intra-arterial PaO2 monitoring via the Clark electrode is well established in neonatal intensive care.4 5 Precision of the Clark electrode has not been subject to Bland and Altman analysis. The reported correlation coefficients are similar to that of the MPIAS, particularly if an allowance for the Clark electrode response time is made when it is calibrated.22 Moreover, the use of a fluorescence sensor instead of a Clark electrode for PaO2 monitoring, seems to avoid the drift with time, associated with the latter.5
With intra-arterial PaO2 monitoring already available, the justification for MPIAS monitoring has to come from monitoring the other variables. This essentially asks: how well does PaCO2monitoring compare with transcutaneous PCO2(TcPCO2) monitoring? This comparison is not straightforward. The initial validation studies for TcPCO2monitoring were performed before the limitations of using correlation coefficients for such purposes were evident.8 These studies indicated a positive bias (over reading) and reasonable precision.23 24 While it was suggested that a correction factor could be used,23 it became apparent that the error increased with higher PaCO2 25 and electrode temperature.26 Some studies also experienced large drifts.27 28 Most importantly, TcPCO2monitoring seemed to be least reliable in the sickest patients, particularly in the presence of hypotension.1 More recently, the validation of TcPCO2 has been reappraised using the methods of Bland and Altman. Carter et al 29 reviewed two newer devices, demonstrating bias (precision) values (kPa) of +0.05 (0.33) and −0.13 (0.47). These values seem impressive, but both groups lost patients to analysis, either as outliers or because of excessive drift. Moreover, while over a quarter of the patients received inotropes, the demographic details (median birthweight 2.3 kg, gestation 34 weeks) are not those of the sickest intensive care infants. The greatest disadvantage of TcPCO2 monitoring, however, remains the need to recalibrate and resite at least 4 hourly, more so in the smallest infants.30 The MPIAS demonstrated minimal drift and so rarely needed recalibration. MPIAS monitoring avoids excess handling, loss of monitoring time and retains precision, even in sick infants.
As well as providing an advantageous alternative to current continuous PaO2 and PaCO2 techniques, the MPIAS has two novel features. It permits continuous arterial pH monitoring. This advance has the potential to provide early warning of deteriorations in the metabolic component of arterial blood gas status. The method of introducing the MPIAS after umbilical arterial catheter placement also allows the clinician to defer MPIAS insertion. Thus in those infants in whom it is not clear whether continuous intra-arterial blood gas monitoring is justified, the decision can be deferred (for the first few hours of intensive care) without losing the opportunity to establish umbilical arterial access.
It is important to understand that the purpose of this study was to validate the sensor (MPIAS) in vivo and not the mechanism used to introduce it (SIS). The SIS was modified five times during the study and this substantially improved the success rate of insertion. Thus the failure rate in this study does not reflect the reliability of the current design. In those infants in whom the catheter had to be removed “before clinically indicated,” seven out of eight had been in place for more than 7 days. We did not find evidence of thrombus formation in the catheter tips. We did not find any complications associated with using the MPIAS. The complications following the breech delivery were unusual, but so is the combination of tractional and rotational forces on the spinal column in association with intrapartum asphyxia in a preterm infant. We were sufficiently concerned to arrange for an independent opinion which confirmed that this was not an event associated with use of the catheter.
In conclusion, the Neotrend MPIAS represents an exciting development in the field of continuous monitoring in neonatal intensive care. Bias/precision data indicate that it is a valuable clinical tool. It will not eliminate the need for ABG sampling, but the potential benefits of reduced blood transfusions and earlier intervention in adverse events are clear. Whether this translates into long term patient benefits, needs to be examined in randomised controlled trials.
Acknowledgments
We thank Selina-Jane Walker and the neonatal intensive care staff in all three units for their support during the study. We are grateful to Diametrics Medical Ltd for their contribution to the funding of this project.