Article Text

Abstract
AIMS To determine if erythromycin given from birth reduces the inflammatory response and the incidence and severity of chronic lung disease.
METHODS Seventy five infants less than 30 weeks of gestation and ventilated from birth for lung disease were randomly assigned to receive erythromycin intravenously for 7 days or to no treatment. Ureaplasma urealyticum was detected in tracheal secretions by culture and polymerase chain reaction. Differential cell counts were obtained from bronchoalveolar lavage fluid collected daily for 5 days and concentrations of the cytokines interluekins IL-1β and IL-8, and tumour necrosis factor α (TNF-α) were measured. Chronic lung disease (CLD) was defined as oxygen dependency at 36 weeks of gestation.
RESULTS Nine infants (13%) were positive forU urealyticum. The inflammatory cytokines in the lungs increased over the first 5 days of life in all babies, but no association was found between their concentrations and the development of CLD. Those treated with erythromycin showed no significant differences from the non- treated group in the differential cell counts or concentrations of the cytokines. The two groups had a similar incidence of CLD. Babies infected with U urealyticum did not have a more pronounced cytokine response than those without infection. Chorioamnionitis was associated with significantly higher concentrations of IL-1β and IL-8 on admission: these babies had less severe acute lung disease and developed significantly less CLD.
CONCLUSIONS U urealyticum in the trachea was not associated with an increased inflammatory response in preterm infants. Erythromycin did not reduce the incidence or severity of CLD.
- chronic lung disease
- Ureaplasma urealyticum
- erythromycin
- cytokines
Statistics from Altmetric.com
Chronic lung disease (CLD), defined as a persistent oxygen dependence at 36 weeks equivalent gestation,1 is a persistent problem among preterm survivors who have received assisted ventilation. Its incidence has changed little despite improvements in neonatal care.2
The aetiology of CLD is multifactorial, with gestation, oxygen, and positive pressure ventilation being the most important factors. An association has been shown between infection of the lower respiratory tract with the genital mycoplasmas, particularly Ureaplasma urealyticum and CLD, although a definite cause and effect association has never been proved.3 These organisms are often found in the genital tract of pregnant women and have been implicated in the onset of preterm labour as well as with disease in the newborn.4 A pilot study in this unit showed an incidence of infection of 25% in babies under 30 weeks of gestation and an association between infection and CLD.5
During the first days of life there is an increase in the proinflammatory cytokines interleukin-1β (IL-1β), interleukin-8 (IL-8), and tumour necrosis factor-α (TNF-α) in the lungs of ventilated preterm infants.6 Ongoing lung damage may be caused by the failure of the premature baby to down regulate and control this inflammatory response.7 Oxygen and barotrauma from ventilation are potent triggers of inflammation, but evidence suggests that infection, particularly with organisms such as U urealyticum, may also be a factor in the persistence of this inflammatory response.8
This study was designed to determine if treatment with erythromycin from birth, to eradicate possible U urealyticum in babies with a high risk of developing lung damage, would reduce the early inflammatory response and influence the incidence and severity of subsequent CLD.
Methods
Babies less than or equal to 30 weeks of gestation and ventilated were randomised (using sealed envelopes containing random number table allocation) at birth to receive erythromycin (15mg/kg/dose three times a day intravenously for 7 days) or not. Those with major congenital abnormalities were excluded. No other changes were made to the unit’s protocols for the care of these infants. The study had received approval from Lothian ethics committee and signed parental consent had been obtained.
Tracheobronchial secretions were obtained on admission. These were transported immediately to the laboratory and cultured for all common pathogens. For U urealyticum a specific broth was used (Difco PPLO broth) enriched with 1% urea. This organism contains a urease that breaks down urea to ammonia and raises the pH of the broth which is detected using a phenol red indicator. Each sample was incubated at a temperature of 37°C for 5 days. Positive samples were recultured on to blood agar to detect possible contamination by other urea splitting organisms. Nucleic acid was extracted from 100 μl of the endotracheal aspirate and, if present, U urealyticumwas detected using polymerase chain reaction (PCR) amplification of the urease genes.9 The laboratory was unaware of the treatment group of the baby and the culture and PCR results were not made available to the clinical team until after completion of the study.
Bronchoalveolar lavage (BAL) was performed as soon after admission as possible and before any surfactant was administered. This was repeated daily for 5 days if the baby was still ventilated. Saline (0.5 ml) was instilled into the endotracheal tube, which was reconnected to the ventilator for 30 seconds. The fluid was recovered with a 6 FG UnoPlast suction catheter attached to a mucus extractor with a control suction connector (Vygon Ltd), using between 15 and 20 cm H2O suction pressure. Heart rate, transcutaneous oxygen, and carbon dioxide were monitored throughout the procedure.
The BAL fluid was spun immediately after collection to separate the cells and the supernatant fluid was frozen at −70°C for subsequent analysis. The cells were resuspended and counted using a counting chamber. A differential count was obtained on 300 cells following staining with Diff-Quick. IL-1β and TNF-α were measured in the supernatant fluid using commercially available high sensitivity enzyme linked immunsorbent assay (ELISA) (R&D Systems). IL-8 was measured using an inhouse radioimmunoassay. The results were expressed as absolute concentrations without any allowance for the volume of BAL fluid obtained. All analyses were done by one person who was unaware of the treatment group or infection status of the baby. None of these results was available to the clinical team until after completion of the study.
Chorioamnionitis was diagnosed by the presence of inflammatory cells in the placenta and fetal membranes. The pathologist was unaware of the clinical condition or treatment group of the baby.
CLD was defined as a persistent oxygen requirement with chestx ray changes at 36 weeks of gestational age. The severity of lung disease at this time was estimated using the alveolar arterial oxygen difference (AaDO2) which correlates with the degree of pulmonary dysfunction at 1 year of age in babies with CLD.10 AaDO2 was measured at 36 weeks of gestational age from an arterial blood gas while the baby was in a steady state breathing 50% oxygen in a head box.
The primary outcome of this study was to compare the concentrations of the inflammatory cytokines in the treated and non-treated (control) groups. The distributions of all the cytokine measurements were highly skewed and therefore the data were analysed after logarithmic transformation. Measurement values were compared between the groups for the following time periods: before surfactant (on admission); after surfactant (within first 24 hours); 24–48 hours, 48–72 hours, 72–96 hours. Statistical comparisons at each time point were made using Mann-Whitney U tests. From the pilot studies in this unit5 6 it was calculated that a sample size of 80 babies would give 90% power to detect as significant a mean five-fold reduction in IL-8 concentrations resulting from treatment.
The effect of treatment on the incidence and severity of CLD was studied by comparing the treated and control groups using Fisher’s exact and Mann-Whitney U tests, as appropriate. Stepwise multiple linear regression was used to determine the combined effects of treatment, infection, oxygen status, surfactant, chorioamnionitis, mode of delivery and antenatal steroids on the cytokine concentrations.
Results
During the study period, 172 infants of gestation ⩽30 weeks were admitted to the unit (table 1). Of the 75 randomised into the study, PCR and suitable cultures for U urealyticum were obtained for 60 of which nine (15%) were positive. No other organisms were isolated in these infants.
All infants <=30 weeks gestation admitted in study period
Table 2 compares the treated infants with those not given erythromycin (control group). There were more boys in the control group (p=0.04), but no significant differences for any of the other variables. The incidence of chronic lung disease was the same in both groups. The AaDO2 was greater in the control group, suggesting more severe lung disease, but this did not quite reach significance (p=0.051).
Comparison of babies given erythromycin (treatment group) with those not treated (control group) Figures are numbers or*medians (range)
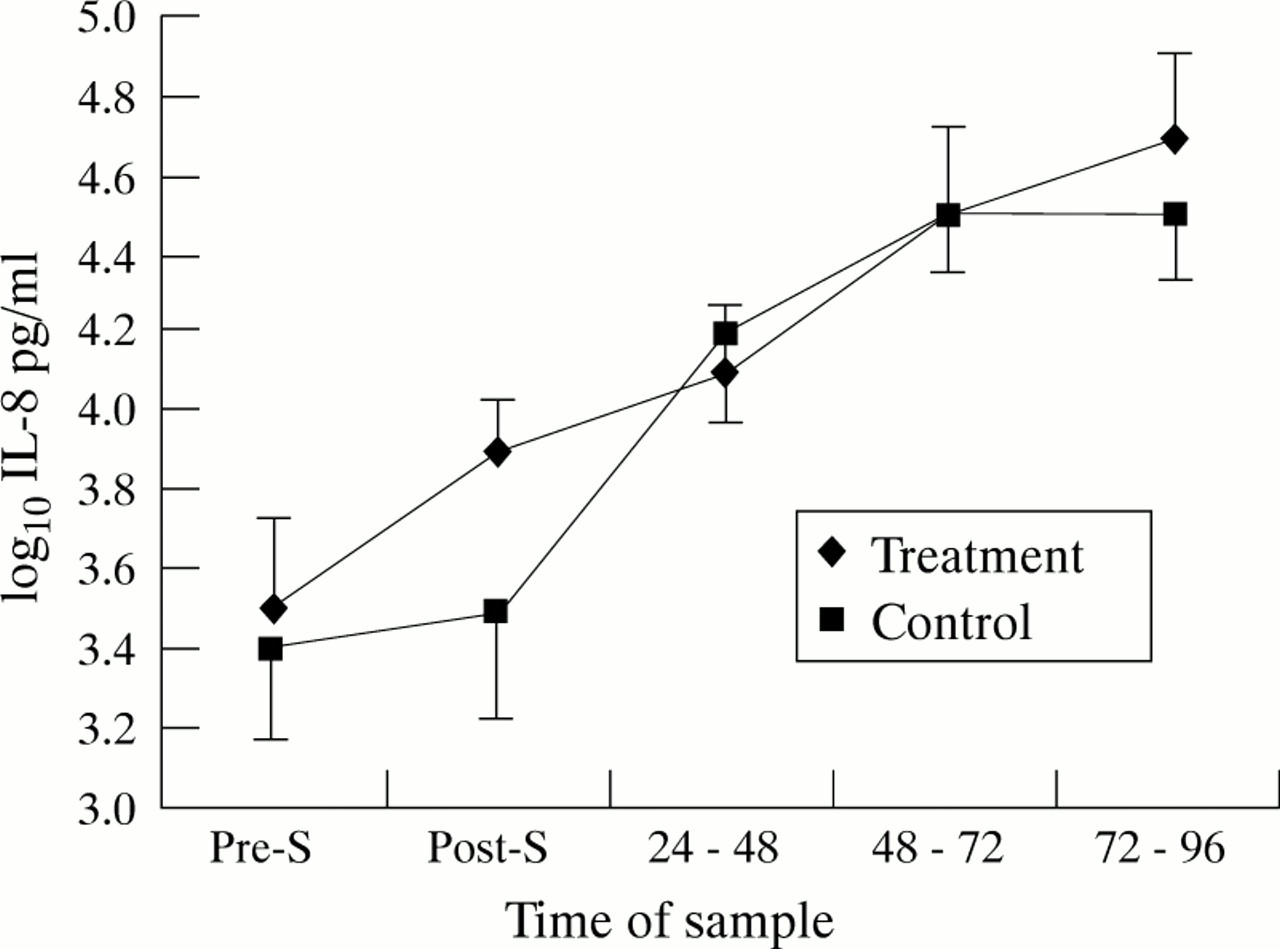
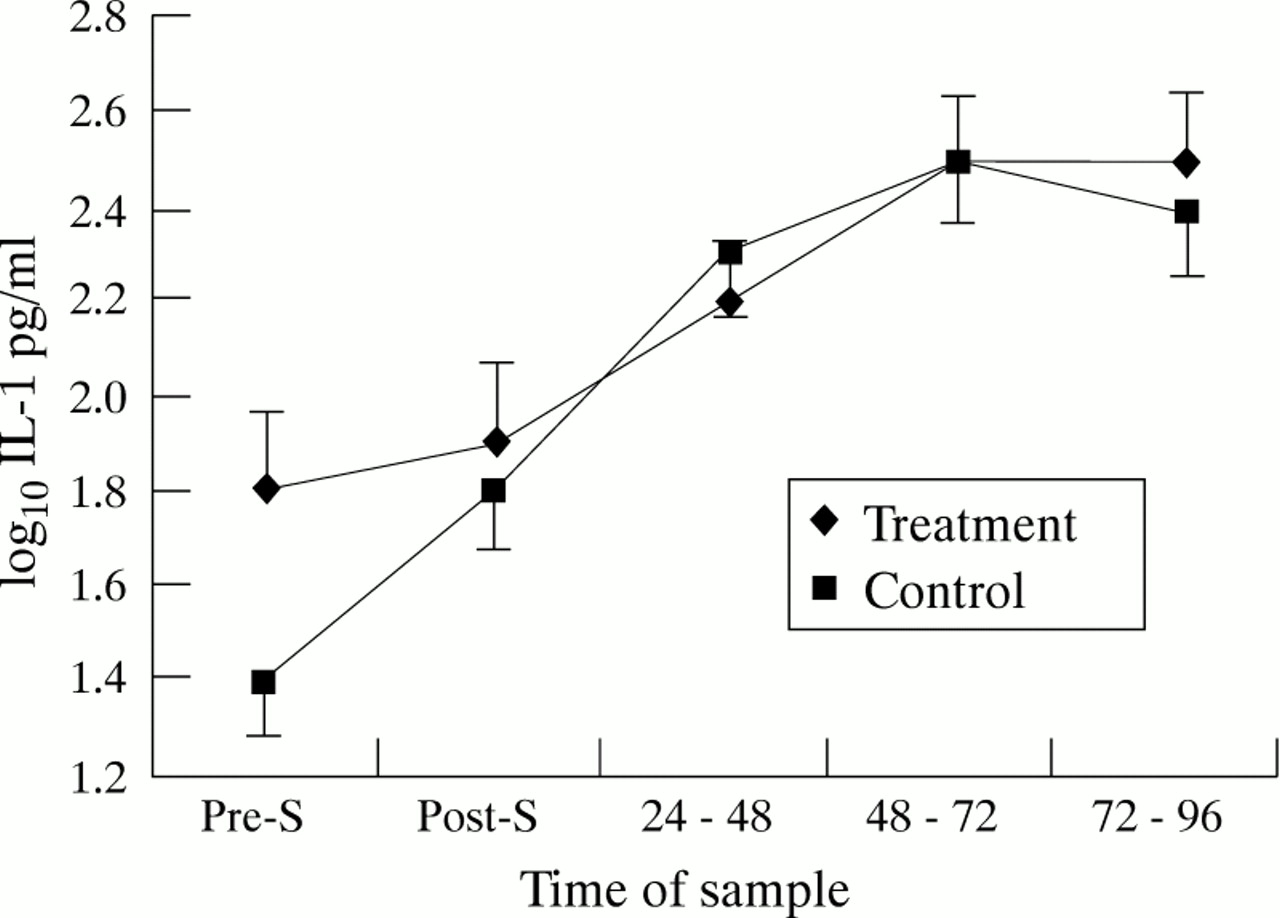
Figures 1 and 2 show the changes in IL-1β and IL-8 over time for the treated and control groups. In both groups the cytokines rose over the first 48 hours and then levelled out. There were no significant differences at any time between the groups for either cytokine. TNF-α was almost undetectable in all samples, with median values of zero on all days.

Changes in Il-8 over time in treated and control groups. Points are mean and standard errors of the mean.

Changes in Il-1β over time in treated and control groups. Points are means and standard errors of the mean.
Table 3 shows the cell counts for the two groups in the first 5 days of life. The total cell count rose over the first 24 hours and then remained high. Epithelial cells predominated at birth and then fell over the first 48 hours. Macrophages and neutrophils increased after 24 hours, with the latter being the predominant cell type. There were no significant differences between the two groups in differential cell counts on any of the days.
Cell counts (medians and ranges) for babies given erythromycin (E) and those not treated (NT)
Table 4 compares the infants who were positive for U urealyticum with those who were not infected. Those with infection were less likely to receive surfactant (p=0.04), but there were no other significant differences. Figures 3 and4 show the changes in IL-1β and IL-8 over time. The non-infected babies had significantly higher IL-8 concentrations at 48–72 hours of age (p<0.05), but there were no other significant differences. The cell counts showed a similar pattern to that in table 3 and there were no significant differences at any time between the two groups.
Comparison of babies positive for Ureaplasma urealyticum compared with those not infected Figures are numbers or*median (range)

Changes in Il-8 over time in the infected and non-infected groups. Points are means and standard error of the means: *p<0.5.

Changes in Il-1β over time in infected and non-infected groups. Points are means and standard errors of the means.
The placenta was studied in 68 cases and chorioamnionitis was found in 20 (table 5). U urealyticum was isolated in four, but no other organisms were found in the babies. No cultures were done in the mothers. Cases in whom chorioamnionitis was found were less likely to receive surfactant and, of those still alive at 36 weeks gestation, significantly fewer developed CLD.
Surfactant use and incidence of CLD in association with chorioamnionitis
Table 6 compares the infants with CLD with those who were alive at 36 weeks of gestation and no longer oxygen dependent. As expected, those with CLD were ventilated longer (p<0.0001) and were more likely to have received surfactant (p=0.004). There was a significant difference in the AaDO2 (p=0.037).
Comparison of infants who developed CLD with those still alive at 36 weeks and no CLD. Figures are numbers or *median (range)
Figures 5 and 6 show the changes in IL-1β and IL-8 over time for the two groups. The babies not developing CLD had significantly higher IL-1β (p<0.05) and IL-8 (p<0.01) on admission, but there were no significant differences at other times. The pattern of change in cell counts was the same as that shown in table 3, with no significant differences between the groups on any day.

Changes in Il-8 over time in babies who developed CLD and those who did not. Points are means and standard errors of the mean: *p<0.01.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in Il-1β over time in babies who developed CLD and those who did not. Points are means and standard errors of the mean.
Stepwise multiple linear regression analysis showed that only chorioamnionitis was significantly correlated with the initial cytokine concentration (p<0.001). If allowance was made for the presence of chorioamnionitis then there was no significant difference between the two groups for IL-1β or IL-8 on admission.
Discussion
The incidence of infection in the babies ⩽30 weeks of gestation was 15% compared with 25% found in the pilot study.5 The use of PCR as well as culture made it less likely that cases were missed, and this probably reflects the true incidence of infection in this unit. There has been an increase in the proportion of mothers in preterm labour who have received antenatal steroids but no changes in antenatal management that would have affected infection rates. In particular, none of the mothers was given erythromycin before delivery. Samples for culture were taken before surfactant was given as this may have an inhibitory effect on the growth of U urealyticum.11 The small numbers made it impossible to analyse the infected babies alone. However, to be effective erythromycin would have to be given from birth, before culture results were available. The data were therefore analysed to compare all treated infants with those who did not receive erythromycin.
Erythromycin had no effect on the concentrations of IL-1β, IL-8, or TNF-α in the first 5 days of life and did not seem to influence the incidence or severity of CLD. This was despite the significantly fewer boys among the treated babies which would have acted to improve outcome for this group.12 Erythromycin not only has antibiotic activity but also acts as an anti-inflammatory agent, reducing IL-8 release in adults with chronic airways disease13 and neutrophil activity in diffuse panbronchiolitis.14 This effect was not seen in the lungs of preterm babies. This anti-inflammatory effect is related to initial internalisation by phagocytes, resulting in an effect on polymorph function.15 Neutrophils in preterm infants have reduced phagocytic powers due to a lack of surface Fc receptors,16and this may limit the ability to internalise erythromycin and hence reduces the drug’s anti-inflammatory abilities.
The rise over the first days of life in IL-1β, IL-8, and the changes in differential cell counts were similar to those reported before.17 TNF-α remained unexpectedly low. This cytokine is quickly recycled and it may be that our sampling regimen, which was only a small window in a 24 hour period, was unsuitable to detect TNF-α. There were no significant differences in the concentrations of IL-1β or IL-8 between the babies who developed CLD and those who did not. The pilot study had shown that higher concentrations of IL-8 were associated with the development of CLD,6 but infants more mature than 30 weeks were included and CLD was defined as oxygen dependency at 28 days. There has been no change in the management of these babies since that pilot, other than the introduction of high frequency oscillatory ventilation during the latter part of this study. No baby was treated with steroids during the first week of life.
High concentrations of inflammatory cytokines in the airways soon after birth may be due to a local host response to various triggers, and do not necessarily signify invasive respiratory disease. Of more importance in the aetiology of chronic lung damage will be a persistence of this inflammation beyond the first days of life, but no study has been able to measure the inflammatory response over a longer period of time. There is a suggestion that in preterm infants some of the mechanisms that control inflammation are impaired. These infants cannot produce IL-10, an anti-inflammatory cytokine known to regulate the proinflammatory cytokines IL-1β, IL-8, and TNF-α18and this could result in persistence of the inflammatory response.
The presence of chorioamnionitis has been associated with preterm onset of labour and an increased risk of infection in the baby.19 The commonest cause of these changes is ascending infection. Chorioamnionitis induced an inflammatory response in the baby with significantly higher concentrations of IL-1β and IL-8 at birth. These infants had less severe acute lung disease, with significantly fewer being treated with surfactant. Stress in utero can result in maturation of the lungs and this could explain the better early progress in these babies. An association between CLD and chorioamnionitis has been shown, suggesting that, although infection may initially have a maturing affect in the lungs, in the longer term it may induce a damaging inflammatory response to persist.20 In our study, the high cytokine concentrations were seen only on admission, with the concentrations in the lungs on subsequent days being similar to those in babies where there was no evidence of chorioamnionitis. Defining CLD as oxygen dependence at 36 weeks of gestation, the babies born to mothers with evidence of chorioamnionitis had a significantly lower incidence of lung disease.
As a group, the babies colonised with U urealyticum did not have higher concentrations of inflammatory cytokines in their lungs. Increased values were seen when U urealyticum was associated with chorioamnionitis. The infected infants had less severe acute lung disease, as shown by the decreased need for surfactant, but there was no significant difference in the incidence or severity of CLD when compared with non-infected infants.
In the population studied the incidence of infection with U urealyticum was low. There was little evidence that the presence of the organism in the trachea of preterm babies affected the initial inflammatory response. Early treatment with erythromycin in a group of babies at high risk of developing CLD did not reduce the concentrations of the inflammatory cytokines or affect the incidence or severity of subsequent lung damage.
U urealyticum may well be a factor in the development of CLD, but its effect is likely to be minimal compared with that of ventilation and oxygen. A larger study would be needed to study the effects of treatment in infected babies alone, but it seems unlikely that erythromycin from birth will have any significant impact on the development of long term lung damage in preterm infants.
Acknowledgments
We are grateful to Dr Rob Elton for statistical advice and Dr Nick Smith for the placental histology. J McColm and L Middlemist were supported by a grant from the Scottish Office Home and Health Department.