Article Text

Abstract
Background Nasal continuous positive airway pressure (NCPAP) can be applied via binasal prongs or nasal masks; both may be associated with air leak and intermittent hypoxia. We investigated whether the latter is more frequent with nasal masks or prongs.
Methods Continuous 24 hours recordings of inspired oxygen fraction (FiO2), pulse rate, respiratory rate, pulse oximeter saturation (SpO2) and CPAP level were made in preterm infants with respiratory insufficiency (n=20) managed on CPAP in the NICU at the Royal Hobart Hospital. As part of routine care, nasal interfaces were alternated 4-hourly between mask and prongs. In each recording, the first two segments containing at least 3 hours of artefact-free signal for each interface were selected. Recordings were analysed for episodes with hypoxaemia (SpO2 <80% for ≥10 s) and bradycardia (pulse rate <80/min for ≥4 s) and for episodes of pressure loss at the nasal interface. Data were compared using Wilcoxon-matched pairs test and are reported as median (IQR).
Results Infants had a gestational age at birth of 26 (25-27) weeks and postnatal age of 17 (14–24) days. There was no difference in %time with interface leak between prong and mask (0.9 (0–8)% vs 1.1 (0–18)%, p=0.82), %time with SpO2 <80% (0.15 (0–1.2)% vs 0.06 (0–0.8)%, p=0.74) or heart rate <80/min (0.03 (0–0.2)% vs 0 (0–0.2)%, p=0.64). Three infants had interface leak for >10% of the time with prongs and 5 with the mask.
Conclusion Both interfaces resulted in a similarly stable provision of positive airway pressure, and there was also no difference in the occurrence of intermittent hypoxia.
- monitoring
- neonatology
- sleep
Statistics from Altmetric.com
What is already known on this topic?
Continuous positive airway pressure is more effective in preventing treatment failure if applied binasally rather than mononasally.
Nasal masks seem to be more effective than nasal prongs in the first postnatal days, but may be more difficult to keep in place.
What this study adds?
In infants studied beyond the first 3 postnatal days, oxygen requirements and intermittent hypoxia rates were similar with masks or prongs.
Both interfaces may thus be used interchangeably in these infants.
Background
Nasal continuous positive airway pressure (NCPAP) is increasingly used to support preterm infants after birth. Putative benefits of CPAP application include increase in lung volume, stabilisation of the breathing pattern and maintenance of upper airway patency.1–3 These mechanisms are also thought to contribute to the effectiveness of NCPAP in reducing the rate of apnoea or intermittent hypoxia (IH), with the latter being associated with death and impaired development, particularly if episodes last for more than 1 min.4
CPAP can be applied mononasally via a shortened endotracheal tube or binasally using various prongs or nasal masks. While superiority of binasal prongs over a shortened tube has been proven in meta-analysis,5 the situation is less clear for masks versus prongs. The latter may be easier to keep in place, thus potentially allowing for the provision of a more stable positive airway pressure, but may be associated with a higher risk of nasal trauma.6 In a recent systematic review, however, the use of nasal masks instead of prongs was associated with less CPAP failure, defined as the need for mechanical ventilation within 72 hours of initiating CPAP (relative risk 0.63; 95% CI 0.24 to 0.72), suggesting better effectiveness of nasal masks.7 Kieran et al also reported less CPAP failure (28% vs 52%), defined as worsening respiratory distress, recurrent apnoea, FiO2>0.4, pH <7.2 or pCO2>9 kPA within 72 hours of starting therapy, for masks compared with prongs, in their randomised controlled trial involving 120 infants <31 weeks gestational age (GA) who had CPAP started as soon as possible after birth/extubation.8 A recent single centre study randomising 72 infants born at 26–32 weeks GA to nasal prongs or masks at birth, while reporting similar FiO2 requirements throughout the first 24 hours, confirmed that there was less nasal trauma with masks.9 None of these studies, however, reported on CPAP pressure loss or cardiorespiratory instability.
As part of a study comparing automated with manual control of inspired oxygen fraction (ACTRN12616000300471), we performed continuous recordings of oxygen saturation measured by pulse oximetry (SpO2), heart rate and airway pressure at the nasal interface in extremely preterm infants receiving additional inspired oxygen via CPAP. The study was performed in a unit where it was routine practice to alternate the nasal interface used for CPAP application between nasal prongs and masks approximately every 4 hours. We used these data to investigate whether episodes of IH or bradycardia were more frequent with either nasal interface.
Patients and methods
This was a secondary analysis of data from the above study, performed in the Neonatal and Paediatric Intensive Care Unit at Royal Hobart Hospital from May 2017 to September 2018. Infants born at <32-week gestation were eligible if aged less than 4 months, receiving non-invasive respiratory support via a bubble CPAP device (Fisher and Paykel, Auckland, New Zealand) and showing the need or potential need for supplemental oxygen. Signals recorded were pulse rate, respiratory rate (based on impedance plethysmography), pulse oximeter saturation (SpO2; Masimo Radical with 2–4 s averaging, Masimo, Irvine, California, USA), FiO2, and CPAP circuit pressure measured immediately proximal to the nasal interface. A webcam was used to record nursing staff’s interventions allowing identification of nursing care times. The study protocol included 2×12 hours of manual O2 control flanking a 24 hours period with automated control. As part of routine nursing care, infants were changed from mask to prongs or vice versa with each episode of neonatal care, that is, approximately every 4 hours. It was routine practice on the unit to attach chin straps while infants received CPAP.
Clinical data were taken from electronic hospital records. We recorded data at a frequency of 1 Hz using custom-built software and identified episodes of IH (a fall in SpO2 to <80%, lasting for ≥10 s), bradycardia (a fall in pulse rate to <80 beats/min, lasting for ≥4 s) and loss of pressure at the nasal interface (defined as a decrease in mean airway pressure by at least 1 cm H2O, lasting for ≥30 s or a 50% reduction in the mean amplitude of the oscillations in pressure at the nasal interface originating from the bubble CPAP, compared with the preceding 20 s, also lasting for ≥30 s). Analysis was done only on data meeting the following criteria: (i) recorded during periods of manual oxygen control, (ii) recorded during the first 3 hours while on CPAP via mask and during the first 3 hours while on CPAP via prongs, as well as (iii) being artefact-free (ie, having good signal quality, no missing signal) and (iv) not recorded from 1 min before to 30 min after periods of nursing care. We determined the number of episodes and the duration of each episode and summed all episodes to determine their total duration, calculated as the proportion of the total duration of artefact-free recording.
Statistical analysis
The aggregated data for each interface are reported as median (interquartile rage) and compared using Wilcoxon matched pairs test. We estimated that we required a minimum of 14 sets of recording containing at least 3 hours of data recorded with either interface to detect (or exclude) a difference in IH rates in the magnitude of one SD with 80% power and a p<0.05.
Results
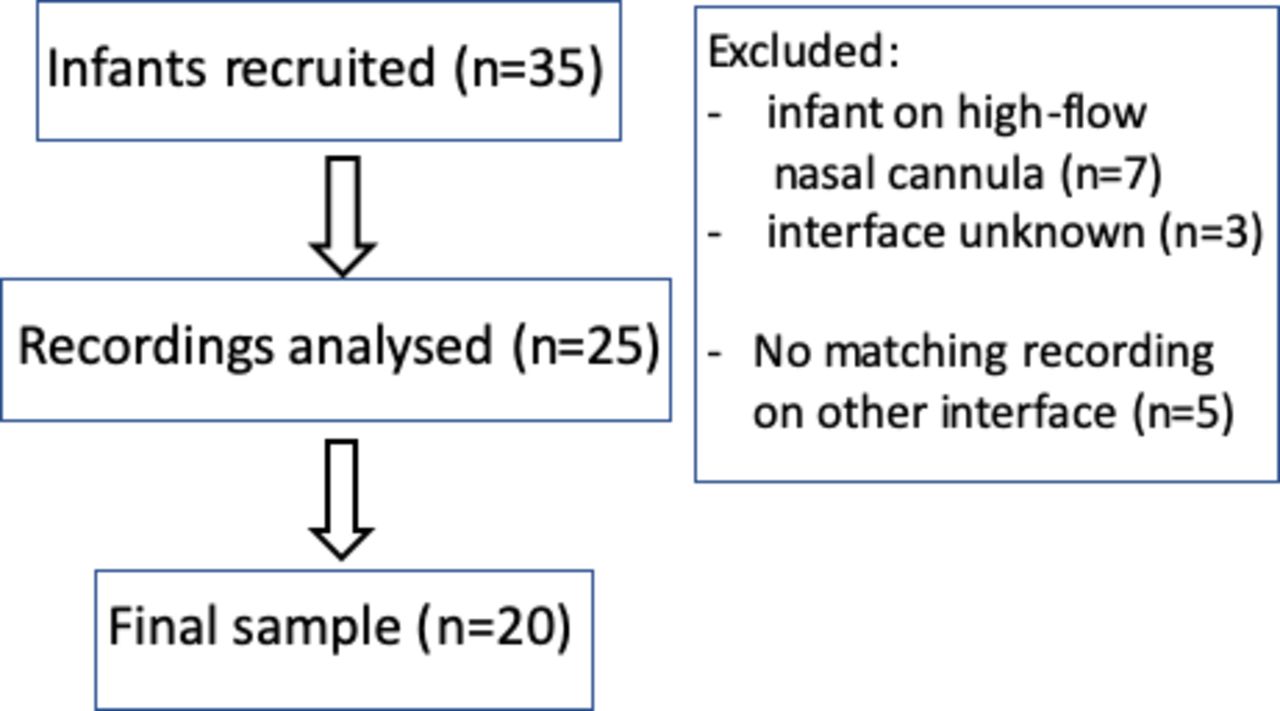
Patient flow for the analyses done in this study is shown in figure 1. All in all, of 35 infants originally enrolled, 20 contributed a sufficient amount of data to be included in this analysis. Their clinical data are summarised in table 1. Fifteen of the 20 infants meeting inclusion criteria received CPAP via a mask during their first 3-hour epoch, the remaining 5 received it via nasal prongs.

{kind=link}
Patient flow.
Clinical data of infants included in this study
Recordings showed rather similar results with either nasal interface, that is, both baseline values (heart and respiratory rate, FiO2 and SpO2) were almost identical, as was the number of events where SpO2 had fallen to <80% (found in 10 infants during CPAP via mask and 11 while on nasal prongs) or heart rate to <80 bpm (found in 8 and 10 infants, respectively; table 2). This may have been related to the fact that there were no differences in the proportion of time with air leak between the mask or prongs and the infant’s face. There were eight infants with leak for >10% of the time; in three, this occurred with prongs, in five with the mask.
Recording results
Discussion
In this small study, CPAP applied via nasal masks resulted in a similarly stable provision of positive airway pressure than with the use of nasal prongs; concomitantly, there was also no difference in the stability of SpO2 or in bradycardia rates between these two nasal interfaces in the very low birth weight infants studied here. Our data thus suggest that nasal masks and prongs can be used interchangeably as nasal interfaces when providing CPAP to preterm infants beyond their first 72 hours of age, as both appeared equally effective in maintaining a constant pressure at the nasal interface and avoiding IH. However, given our study design, these findings should not be extended to the first 1–2 days after birth, at which time less treatment failure within 72 hours of starting therapy has been observed with nasal mask CPAP.8
This being a secondary data analysis, we need to emphasise that our results can only be hypothesis-generating. Nonetheless, they add another aspect to the data from a large randomised controlled trial and a systematic review that showed superiority of nasal masks in preventing CPAP failure7 8 such that we found no difference between either nasal interface in this slightly older patient population. Further limitations include that the sequence of the interventions studied was not randomised, but this is unlikely to have biased results as nurses were following a strict protocol to change between mask and prong with each care round. Also, some differences in mask leak may have been related to change of bedside staff member, but we have no information on this aspect. We used two definitions and methods to identify mask leak: a reduction in bubble amplitude on the nasal pressure signal and a fall in mean airway pressure. Neither method has been validated, but in our experience they are both suitable for identifying mask leak. Also, although infants had chin straps attached to minimise pressure loss through the mouth, we cannot exclude that some periods of pressure loss occurred through the mouth.
In conclusion, this small observational study in infants studied beyond 3 days of age supports the use of either nasal mask or prongs for CPAP support in infants <32-week gestation. Randomised controlled studies are needed to prove that truly either nasal interface can be used when applying CPAP in such infants.
Footnotes
Contributors CFP was involved in data analysis and wrote the first draft of the manuscript, KL, AM and TJG analysed the data and revised the manuscript for important intellectual input, HJ was involved in supervising recordings and revised the manuscript for important intellectual input, and PAD initiated and supervised this study and revised the manuscript for important intellectual input. All authors approved the submitted version of this manuscript and agree to be accountable for all aspects of this work and take full responsibility for it.
Funding Supported by a grant (16-203) from the Royal Hobart Hospital Research Foundation. Circuit pressure monitoring equipment was kindly loaned by Fisher & Paykel Healthcare Ltd, East Tamaki, New Zealand.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study had been approved by the institutional ethics committee as an audit of clinical practice.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.