Article Text

Abstract
Neonatal intubation is an essential but difficult skill to learn. Videolaryngoscopy allows the airway view to be shared by the intubator and supervisor and improves intubation success. Ideally, a videolaryngoscope (VL) should be usable as a conventional laryngoscope (CL). The aims of this report were to describe differences in the shape of currently available CL and VL blades and to compare the direct airway view obtainable on a neonatal manikin with different laryngoscope blades.
Three main differences were observed; compared with CL, the VL blades have a reduced vertical height, a curved tip and curved body. The direct airway view obtained by the VL is narrower than that obtained with the CL, although the corresponding view on the VL screen is maintained.
Minor adaptation of intubation technique may be required when using a VL. Modifying VL blades to reduce these differences may improve their usefulness as an intubation training tool.
- neonate
- videolaryngoscopy
- endotracheal intubation
Statistics from Altmetric.com
What is already known on this topic?
Neonatal intubation is an essential skill. It can be difficult to learn, and success rates, especially for inexperienced trainees, are low and falling.
Videolaryngoscopy improves intubation success rates when used as a teaching tool for inexperienced intubators.
What this study adds?
This report highlights key issues with the use of videolaryngoscopy in neonates relating to the shape of the blades available.
Users of videolaryngoscopy should be aware of the possible need to adapt traditional intubation technique until blades that are more tailored to neonates and infants are developed.
Introduction
Endotracheal intubation is an essential skill for trainees; however, it is difficult to learn. Intubation success rates are falling, especially for inexperienced trainees. This is due to the frequency of neonatal intubations decreasing and trainees not being exposed to the volume of practical experience required to achieve proficiency.1 The reasons for this are multifactorial, including evolving neonatal resuscitation practices, increasing reliance on non-invasive ventilation and increasing numbers of trainees. Neonatal intubation has the additional challenge of the intubator and their supervisor being unable to share the view of the infant’s airway during the attempt. Commonly, intubation failure is the result of lack of recognition of the anatomy of the infant’s airway by the trainee.2
Videolaryngoscopy is used by adult anaesthetists as the magnified view is beneficial, particularly for challenging airways.3 4 In neonates, the use of videolaryngoscopy has been shown to be clinically feasible and significantly improves intubation success rates.5 Its use is gaining popularity as an intubation training tool6 through providing a means of the intubator and supervisor sharing the airway view.7 This allows the supervisor to provide instruction and highlight important anatomical landmarks. However, until videolaryngoscopy is universally available, the skills learned by trainees should be transferrable to direct laryngoscopy. When using a videolaryngoscope (VL) to teach direct laryngoscopy, the experience for the intubator should be as similar as possible to the experience of using a conventional laryngoscope (CL) and the VL should be usable as a direct laryngoscope. As such, ideally, the VL blade should closely resemble the CL blade.
Aim
The aim of this report is to compare CL and VL blades and describe differences in their shape. Furthermore, we aimed to demonstrate the effect these differences have on the direct view of the vocal cords.
Method
This is an observational study comparing three brands of single-use CL Miller blades in sizes 00, 0, and 1; Callisto (TIMESCO, Essex, UK), Metal max disposable combi laryngoscope set (PROACT, Northamptonshire, UK) and Metal max 100 (PROACT), with three brands of VL Miller blades available in the UK; InfantView reusable blades, sizes 00, 0 and 1 (ACUTRONIC, Hirzel, Switzerland), C-MAC reusable blades, sizes 0 and 1 (Storz, Tuttlingen, Germany) and C-MAC single-use blades, sizes 0 and 1 (Storz). The shapes of the blades were compared in different aspects and the observed differences described with measurements made using ImageJ software (a public domain, Java-based image processing program developed at the National Institute of Health8).
The CL and VL blades were used to perform direct laryngoscopy on a preterm manikin (SimNewB, Laerdal medical, Stavanger, Norway) shown to have high physical and functional fidelity.9 Direct laryngoscopy was performed by both authors for all blades, and the best airway view obtained was photographed by placing a camera (Nikon D610) at the intubator’s eye level. When VL blades were used, the corresponding images on the VL monitors were also photographed.
Results
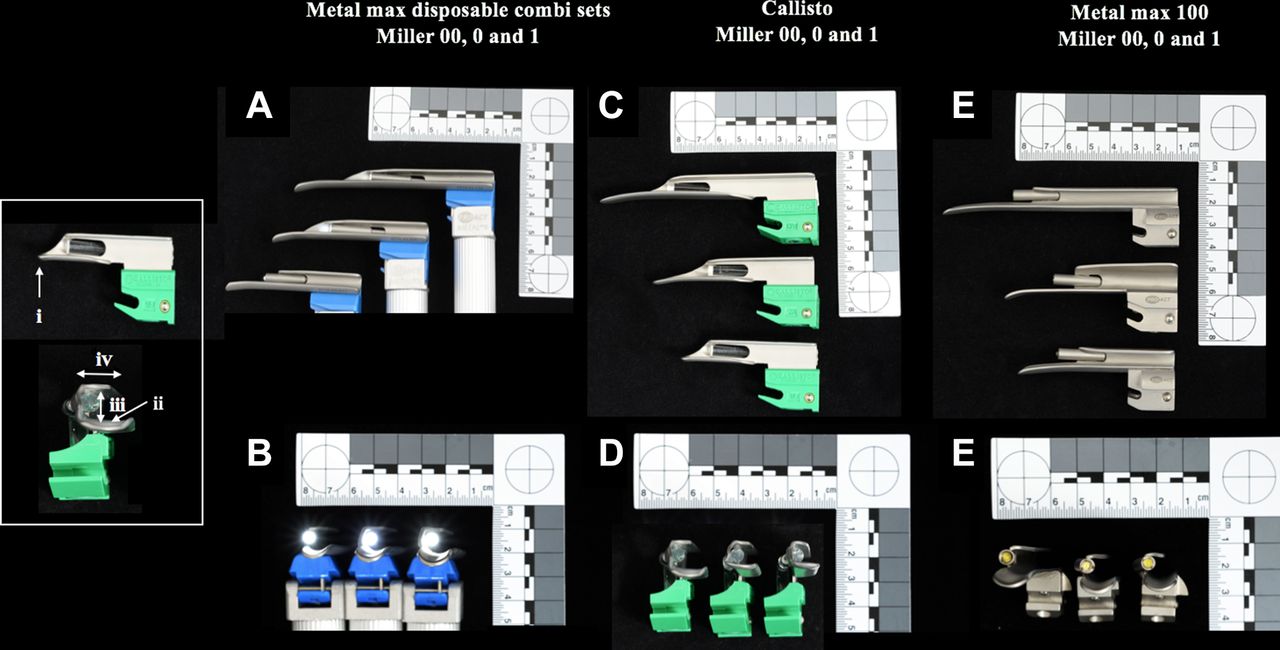
The CL blades are demonstrated in figure 1, and the VL blades are demonstrated in figure 2. On comparison of CL with VL blades, three main differences were observed that were consistent across the brands studied. Firstly, the tips of the VL blades (figure 2.i) are more curved compared with the CL blades’ straighter tips (figure 1.i). Secondly, the floor of the body of the VL blades has a midline trough running the length of the blade (figure 2.ii), whereas the floor of the body of CL blades is flat (figure 1.ii). Thirdly, the overall vertical height of the VL blades (figure 2.iii) is less than that of the CL blades (figure 1.iii), due to the presence of a ledge above the light source in the CL blades (figure 1.v), which is missing in the VL blades. Table 1 demonstrates measurements of the vertical height of all the studied blades.
Measurement of blade vertical height
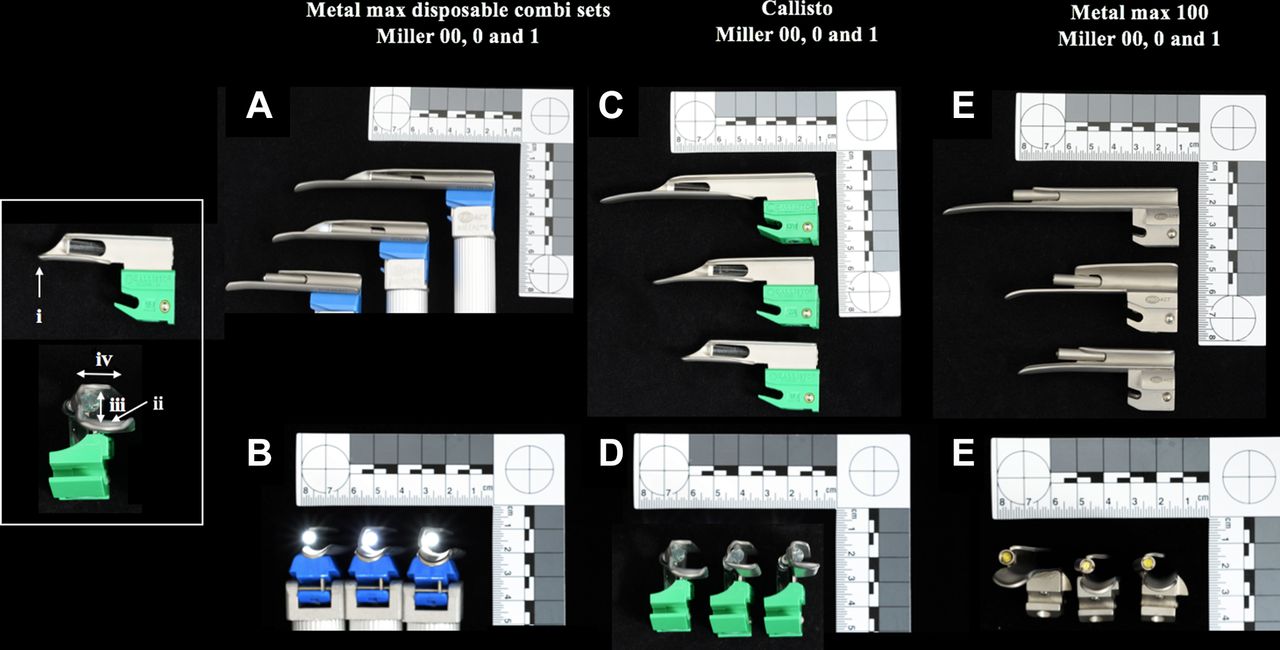
Conventional laryngoscope Miller blades in two aspects: (A and B) PROACT Metal max disposable combi laryngoscope set, (C and D) TIMESCO Callisto single-use blades and (E and F) PROACT metal max100 single-use blades. (i) Blade tip, (ii) blade body, (iii) vertical blade height and (iv) ledge above light source.

Videolaryngoscope Miller blades in two aspects: (A and B) ACUTRONIC InfantView re-usable Miller blades, (C and D) Storz C-MAC reusable Miller blades, (E and F) Storz C-MAC single-use Miller blades. (i) Blade tip, (ii) midline trough and (iii) vertical blade height.
The differences described impact on the direct vocal cord views obtainable with a VL compared with the views obtainable using a CL (figure 3A–C). The reduced overall vertical height of the VL blades in particular results in a shorter, narrower and more restricted view of the oropharynx on direct laryngoscopy with a VL (figure 3D–F), although the view on the monitor is well maintained (figure 3G–I).

{kind=link}
{kind=link}
{kind=link}
Laryngoscopy on preterm manikin. (A–C) Direct laryngoscopy with conventional laryngoscopes. (D–F) Direct laryngoscopy with videolaryngoscopes. (G–I) Associated videolaryngoscopy images. (J–L) Direct laryngoscopy with videolaryngoscopes and manikin’s top lip lifted.
Discussion
This comparison demonstrates differences in the shape of available VL blades when compared with CL blades and the effect these have on the direct airway view obtainable. The result is a constricted direct view with reduced space to pass an endotracheal tube under direct vision, while the image on the VL monitor remains adequate. Through clinical experience using the available Miller videolaryngoscopes in the UK, we have identified that with help of an assistant lifting the infant’s top lip, the direct airway view can be expanded, and the space available for passing an endotracheal tube increased (figure 3J–L).
Videolaryngoscopy is increasingly considered standard practice by adult anaesthetists due to its ability to provide a magnified airway view and reduce intubation failure.10 Its application for direct laryngoscopy in adult practice is less important as the view on the monitor is used as the primary visualisation of the airway. In neonates, videolaryngoscopy’s main use and benefit lie in the fact that it enables an intubator and their supervisor to share the airway view. To maximise this benefit, the direct view should be as similar as possible to that on the video screen.
There is a limited variety of videolaryngoscopes available in the UK. The InfantView is designed for neonates and has Miller 00, 0 and 1 blades. The C-MAC is suitable for infants, children and adults. It has Miller 0 and 1 blades but no 00 blade; therefore, its use is problematic in extremely preterm infants. The McGRATH MAC (Medtronics, Minneapolis, Minnesota, USA) has a curved Macintosh 1 blade. Most neonatologists are inexperienced with curved blades, and they are not suitable for smaller infants. The Airtraq (Prodol Meditec, Vizcaya, Spain) and Glidescope (Verathon, Washington, USA) were designed as alternative methods of intubating. They do not resemble traditional laryngoscopes, and direct laryngoscopy with them is not possible.
As technology improves, videolaryngoscopy may become routine for neonatal intubation. Until then, when videolaryngoscopes are not universally available where neonatal intubation may be required (i.e. labour ward rooms, theatres, neonatal transport service and emergency departments), trainees need to achieve proficiency intubating using a direct airway view. To maximise transferability of skills when teaching with a VL, the blade should resemble that of a CL and the direct airway view should be similar to that on the monitor. We have identified a straightforward technique to optimise the direct view obtainable with a VL. Modifying the intubation technique being taught does, however, carry the risk of reduced transferability of the learned skill. There is a lack of literature on modifying intubation technique when using a VL in the neonatal population; therefore, this is an area requiring ongoing research.
New users of videolaryngoscopy in neonates should be aware of these differences in blade design. The technique described to widen the direct airway view is useful in increasing the effectiveness of currently available models for teaching. Nonetheless, while videolaryngoscopy is being used as an aid for teaching and maintaining direct laryngoscopy skills, it should mimic conventional laryngoscopy as closely as possible, and the shape of the blade is integral to this. Manufacturers of videolaryngoscopes should be attuned to these observations to adequately tailor the technology to neonates and infants.
Conclusion
VL blades available in the UK have several important differences in their design when compared with CL blades. These differences impact on the direct airway view obtainable with a VL. Ideally, neonatal VL blades would be functionally the same as CL blades to optimise the use of videolaryngoscopy in teaching neonatal intubation.
Acknowledgments
Many thanks to Miss Lisa Miller (medical photographer, Medical Illustrations department, QEUH Glasgow) for assistance with photography.
Footnotes
Contributors Both authors contributed equally to the design, undertaking, writing and editing of this report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No unpublished data available from this study.