Article Text

Abstract
Objective Since therapeutic hypothermia became standard care for neonatal hypoxic–ischaemic encephalopathy (HIE), even fewer infants die or have disability at 18-month assessment than in the clinical trials. However, longer term follow-up of apparently unimpaired children is lacking. We investigated the cognitive, motor and behavioural performances of survivors without cerebral palsy (CP) cooled for HIE, in comparison with matched non-HIE control children at 6–8 years.
Design Case–control study.
Participants 29 case children without CP, cooled in 2008–2010 and 20 age-matched, sex-matched and social class-matched term-born controls.
Measures Wechsler Intelligence Scales for Children, Fourth UK Edition, Movement Assessment Battery for Children, Second Edition (MABC-2) and Strengths and Difficulties Questionnaire.
Results Cases compared with controls had significantly lower mean (SD) full-scale IQ (91 [10.37]vs105[13.41]; mean difference (MD): −13.62, 95% CI −20.53 to –6.71) and total MABC-2 scores (7.9 [3.26]vs10.2[2.86]; MD: −2.12, 95% CI −3.93 to –0.3). Mean differences were significant between cases and controls for verbal comprehension (−8.8, 95% CI –14.25 to –3.34), perceptual reasoning (−13.9, 95% CI–20.78 to –7.09), working memory (−8.2, 95% CI–16.29 to –0.17), processing speed (−11.6, 95% CI–20.69 to –2.47), aiming and catching (−1.6, 95% CI–3.26 to –0.10) and manual dexterity (−2.8, 95% CI–4.64 to –0.85). The case group reported significantly higher median (IQR) total (12 [6.5–13.5] vs 6 [2.25–10], p=0.005) and emotional behavioural difficulties (2 [1–4.5] vs 0.5 [0–2.75], p=0.03) and more case children needed extra support in school (34%vs5%, p=0.02) than the control group.
Conclusions School-age children without CP cooled for HIE still have reduced cognitive and motor performance and more emotional difficulties than their peers, strongly supporting the need for school-age assessments.
- hypoxic-ischaemic encephalopathy
- therapeutic hypothermia
- cognitive
- motor
- behavioural outcomes
- school-age
Statistics from Altmetric.com
What is already known on this topic?
Prior to the routine use of therapeutic hypothermia for neonatal hypoxic–ischaemic encephalopathy, school-age children had cognitive and motor difficulties even in the absence of cerebral palsy.
Therapeutic hypothermia trials report variable IQ scores above or below the test mean at 6–7 years in cooled children with and without cerebral palsy.
Contemporary cohorts of infants cooled for neonatal hypoxic–ischaemic encephalopathy report reduced death and disability at 18 months compared with the clinical trials.
What this study adds?
School-age children who underwent therapeutic hypothermia for neonatal hypoxic–ischaemic encephalopathy since it became standard practice have significantly lower cognitive scores and on average 14 IQ points lower than matched peers even in the absence of cerebral palsy.
Motor scores were lower than their peers particularly affecting manual dexterity skills.
Cooled children without cerebral palsy have behavioural scores lower than those of their peers and a 10-fold increased odds of requiring additional support at school.
Introduction
Therapeutic hypothermia (TH) is the standard neuroprotective intervention for neonatal hypoxic–ischaemic encephalopathy (HIE).1 In the prehypothermia era, children who had HIE were reported to have impaired cognitive2 and motor3 abilities and school readiness scores and delayed expressive language4 even in the absence of cerebral palsy (CP). Two trials of TH that had similar definitions of HIE have reported markedly differing results for cognitive scores at 6–7 years, with mean IQ scores of cooled children (including those with CP) nearly 4 points higher5 or 19 points lower6 than the test mean score of 100. The studies do not report cognitive abilities of children without CP separately. This discrepancy in IQ indicates the need for a matched control comparison group to determine how children cooled for HIE perform compared with peers who did not have HIE. While the clinical trials reported motor outcomes pertaining to functioning of children with CP5 and simple neurological examination,6 motor performance in children without CP is unknown.
Furthermore, contemporary cohorts of infants cooled for HIE differ from infants cooled in the clinical trials: they are cooled earlier (0.757–3.98 hours vs 4.79–4.910 hours), cooling is administered using servo-controlled mechanism of core temperature regulation11 rather than manual technique,9 healthcare providers are likely to be more experienced with TH and contemporary cohorts have reported a lower incidence of death or disability (26.31%12–33.0%7 8 13 vs 44.0%–53.1%)1 and reduction in the incidence and severity of CP14 than the clinical trials. Therefore, reanalysis of TH trials data to identify the cognitive abilities of cooled children without CP may not be generalisable to contemporary cohort of infants cooled for HIE.
In this study, we aimed to determine the cognitive, motor and behavioural outcomes and educational provision among children aged 6–8 years who were cooled for HIE and did not develop CP by comparing them with age-matched, sex-matched and socioeconomic class-matched control children.
Methods
Study design and participants
We conducted a prospective case–control study at the University of Bristol, UK, between October 2016 and October 2017. We investigated a cohort of children who underwent TH for HIE using a standard protocol at St Michael’s Hospital, Bristol.15 TH, using servo-controlled whole-body cooling, was commenced in infants born at ≥36 weeks’ gestation with evidence of perinatal asphyxia and subsequent moderate to severe HIE assessed by clinical and amplitude integrated electroencephalogram (EEG) assessment scored based on voltage pattern.9
Case definition
Children from this cohort who were aged 6–8 years (born between April 2008 and February 2010) and did not have a diagnosis of CP comprised the cases. We excluded children who: (1) were cooled outside the standard criteria; (2) had an additional diagnosis, for example, a metabolic disorder; and (3) did not have English as their primary spoken language.
Control definition
We recruited controls from schools around Bristol. We included children who were born at ≥36 weeks’ gestation, had not had HIE and had English as their primary spoken language and were best matched to the case by age, sex and social class. It was emphasised to parents that they would not be given the results of individual assessments to minimise the chance of recruiting children about whom parents had concerns. Social class was defined as A, B, C1, C2, D and E groups based on the national readership survey.16
Developmental and educational history
We obtained a detailed educational, developmental, medical and social history. We measured height, weight and head circumference and performed a physical examination to rule out CP; no children were excluded. We collected data on the age when the child started walking (defined as the age at which the child was able to take five steps independently),17 the provision of additional support in the classroom (defined as having a 1:1 classroom assistant for a portion of the school day, receiving additional classes or being part of a catch-up group) and the need for statements of special educational needs/educational health plan.
Psychometric and motor assessments
A psychologist (JT), blinded to case–control status, assessed the cognitive abilities of the children using the Wechsler Intelligence Scale for Children – Fourth UK Edition (WISC-IV)18 including subscales of working memory, processing speed, verbal comprehension, perceptual reasoning from which full-scale IQ (FSIQ) is derived. A researcher (RL-K) assessed their motor abilities using the Movement Assessment Battery for Children – Second Edition (MABC-2),19 which was videotaped, and double-scored by a separate assessor (SJ). Scoring differences in three children were agreed by consensus. The MABC-2 gives three subscales (manual dexterity, aiming and catching, and balance) standard scores with a mean (SD) of 10 (3). The sum of the subscales scores provides a total score, which when ≤56 or ≤67 places a child at ≤5th or ≤15th centile (high-risk for or at risk of motor impairment).19
Behavioural assessments
Parental perception of behavioural difficulties was recorded using the Strengths and Difficulties Questionnaire (SDQ).20 The SDQ comprises five scales (emotional, conduct, hyperactivity, peer problems and prosocial) of five items each with a maximum score of two per item. The total difficulties score ranges from 0 to 40 and is the sum of the scales excluding the prosocial scale. A higher score indicates increasing difficulties, aside from the prosocial subscale where a higher score indicates better behaviour. Parents also completed the impact supplement that evaluates the effect of the child’s difficulties on the family resulting in an ‘impact score’ with a range of 0–10.
Outcomes
We defined the primary outcome as the mean (SD) FSIQ and the total MABC-2 standard scores. Secondary outcomes included: subscale scores from the WISC-IV and MABC-2, percentage of case children with IQ <1 or 2SD below the test mean and the control group mean compared with controls, total MABC-2 scores ≤15th or ≤5th centile19 and SDQ scores.
Statistical analysis
Normality was tested with Q–Q plot and Shapiro-Wilk’s test. Normally distributed variables are summarised as mean (SD), and variables with skewed distribution are summarised as median (IQR). We compared proportions including the amplitude integrated electroencephalogram (aEEG) pattern before TH, abnormal neonatal MRI defined as moderate or severe lesions in the basal ganglia and thalami or abnormal posterior limb of the internal capsule or severe white matter lesions between cases included and excluded in the study;;21 social class, need for educational support, children with a FSIQ <1 or<2 SD and MABC-2 total score ≤15th and fifth centiles between the case and control children using χ2/Fisher’s exact test. We used the independent samples t-test to compare the normally distributed variables including the WISC-IV FSIQ and total MABC-2 scores, subscales of WISC-IV and MABC-2 between case/control groups and to compare FSIQ scores between children who received additional support at school and those who did not. Mann-Whitney U test was used to compare the variables with skewed distribution including height, age of independent walking and SDQ scores. A probability of <0.05 (two-sided testing) was considered significant. We performed the analysis using IBM SPSS V.24.
Results
Recruitment of study cohort
We had 40 eligible children. Eleven families did not participate (seven were not-contactable and four refused) (figure 1). The neonatal background characteristics, including aEEG background activity and evidence of neonatal MRI brain injury21 and 18-month developmental status were similar between the case children who did and did not participate in the study (see online supplementary table 1). Among cases, 26/29 had a moderately abnormal aEEG (Sarnat grade II encephalopathy) and 3/29 had a severely abnormal aEEG (Sarnat grade III). No case children had a known diagnosis of visual, hearing or speech impairment nor were such problems apparent during testing.
Supplemental material
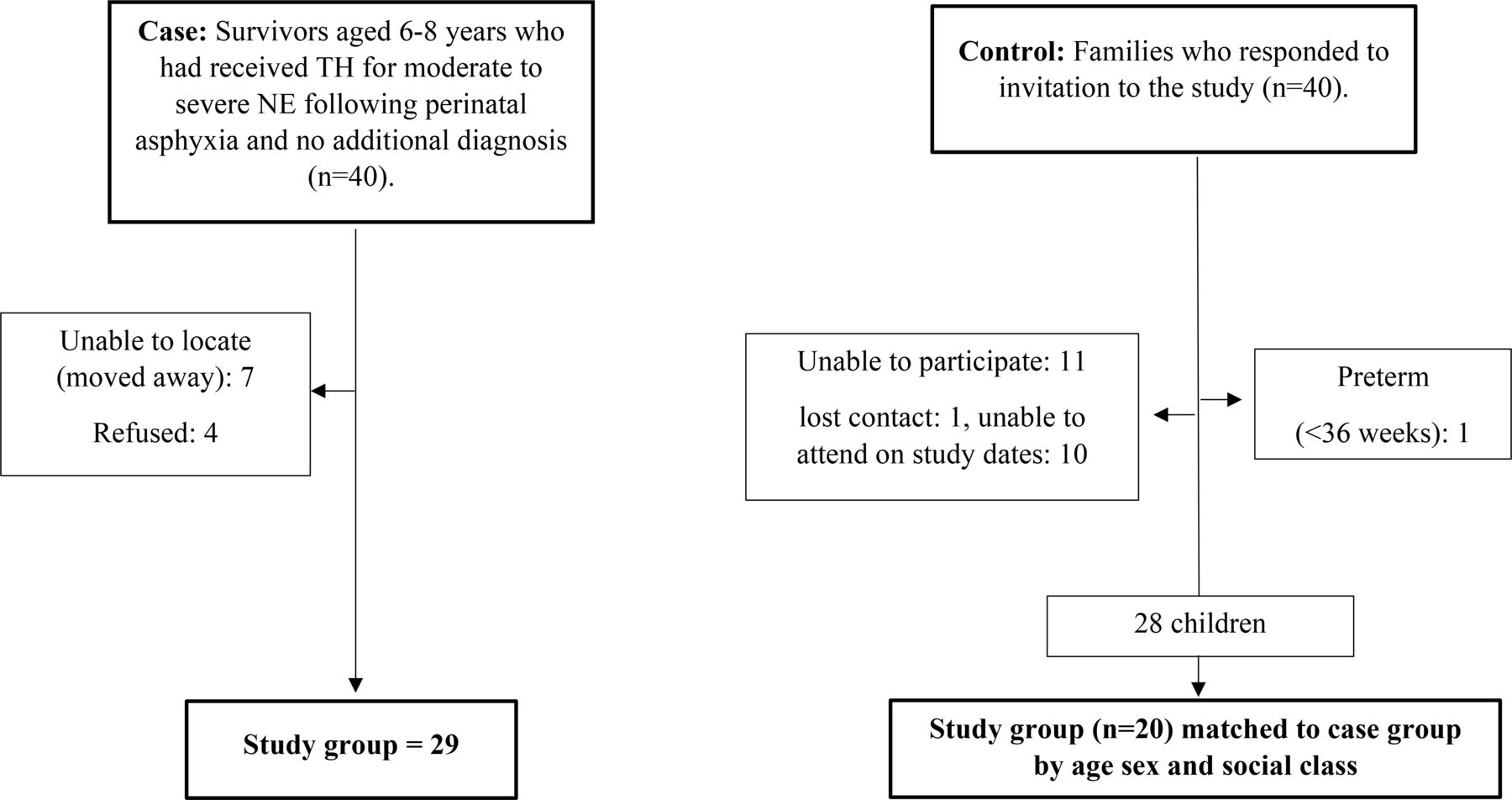
Flow chart showing recruitment of cases and control children. TH, therapeutic hypothermia.
We contacted 133 schools to recruit the controls. Among the 40 families that responded, 20 children who were best comparable with the cases in terms of age, sex and social class comprised the control group (figure 1, table 1).
Case–control comparison of demographics, early development and educational needs
Case–control comparison
A higher proportion of case children were receiving additional support in the classroom than control children (10/29 [34%] vs 1/20 [5%], p=0.02); ORs: 10.0, 95% CI 1.16 to 86.0, and one case child had a statement of special educational needs (none in the control group) (table 1).
The case and control groups were of comparable gestational age, birth weight, weight and head circumference at 6–8 years (table 1). While median (IQR) height centile22 at 6–8 years was significantly lower in the case group than the control group 43.8 (17.5–75) versus 71.1 (50.5–87.2), p=0.02, weight centile and body mass index (BMI) were comparable. There was a weak positive correlation between birth weight and height at 6–8 years (r=0.28) in case children but not in control children (r=0.03).
Median age at commencement of playgroup was similar between cases and control but the median (IQR) age of independent walking was 1 month later in the cases compared with controls (13 months [12–15] vs 12 months [11–14], p=0.02).
Primary outcomes
All 20 control children completed the motor and cognitive assessments. One case child refused to complete the WISC-IV processing speed subscale, preventing the calculation of processing speed and therefore FSIQ score. Case children compared with controls had a significantly lower mean (SD) FSIQ (91 [10.37] vs 105 [13.41]; mean difference (MD) −13.62, 95% CI −20.5 to −6.71) and total MABC-2 score (8 [3.26] vs 10 [2.86], MD −2.12, 95% CI −3.93 to −0.30) (table 2). The test scores of children with severely abnormal aEEG before cooling (n=3) were within the distribution of scores of children with moderately abnormal aEEG although in the lower half of the distribution (see online supplementary figure 1).
Supplemental material
Primary and secondary outcomes at 6–8 years of age
Secondary outcomes
The case group had significantly lower mean standardised scores in all four subscales of the WISC-IV and the manual dexterity and the aiming and catching subscales but not the balance subscale of the MABC-2 than controls (table 2, figure 2). A significantly higher proportion of case children had FSIQ <1 SD below the control mean (<92) than controls and MABC-2 total score ≤15th centile but not at ≤5th (table 2).

{kind=link}
![[fetalneonatal-2018-316509supp002.jpg]](https://fn.bmj.com/content/fetalneonatal/105/1/8/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
Comparison of WISC-IV standardised scores and MABC-2 total and subscale standard scores between case and control children. For full-scale IQ and the different WISC domains (cases n=28 [processing speed, full scale IQ] and n=29 [verbal comprehension, perceptual reasoning and working memory], controls n=20). Data represents the mean scores with 95% CIs. The triangles denote the case children scores, and the circles denote the control children scores. MABC-2, Movement Assessment Battery for Children – Second Edition; WISC-IV, Wechsler Intelligence Scale for Children – Fourth UK Edition.
Children who received additional help at school had significantly lower mean (SD) FSIQ (87.5 [13.8]) than those who did not (99.6 [12.31], MD: −12.1, 95% CI −21.15 to −3.11). Case children who did not receive extra help at school still had statistically lower mean (SD) scores than controls in verbal comprehension (96.2 [7.54] vs 102.8 [10.36], MD:−6.7, 95% CI −12.65 to −0.72), perceptual reasoning (90.7 [10.77] vs 103.6 [12.55], MD:−12.9, 95% CI −20.59 to −5.20) and FSIQ (94.1 [7.56] vs 105.2 [13.78], MD: −11.1, 95% CI −18.44 to –3.67). The case group scored significantly higher in the total difficulties and emotional behavioural difficulties scales of the SDQ compared with control children. Scores for hyperactivity and conduct problems were also higher for cases than controls, the difference approaching statistical significance (table 2).
Discussion
Our study found that school-age children cooled for HIE even in the absence of CP have significantly lower cognitive and motor scores with an IQ, on average, 14 points lower than their peers. Consistent with these findings, a third of the case children were receiving additional classroom support and parents of case children reported significantly higher total and especially emotional difficulties than parents of control children.
Cognitive abilities were particularly affected in the perceptual reasoning and processing speed domain with scores on average 14 points and 12 points lower than their peers. However, in National Institute of Child Health and Human development Neonatal Research Network (NICHD NRN) trial of TH, verbal IQ was more affected than performance IQ and processing speed in cooled children with and without CP.6 In our cohort, a higher proportion of case children had subnormal IQ scores (<1 SD below the mean) when compared with the control mean rather than the test mean. This highlights the importance of comparing cognitive abilities to a contemporary matched control group rather than test standardisation norms. Comparing our case children with cooled children without CP from the NICHD NRN trial,6 we observed a lower proportion with FSIQ <1 SD (21% vs 32%) and <2 SD (3.5% vs 11%) below the test mean indicating that the outcomes in the posthypothermia trial era might be better than that reported in this clinical trial. The mean IQ of our case children was 91; unfortunately, the corresponding data from the clinical trials is unavailable. The lower cognitive abilities reported in this study are in line with prior studies reporting lower cognitive abilities in non-cooled children with HIE without severe disability2 4 23 24 indicating that this effect is still present, despite the use of TH.
Motor assessment in the clinical trials has been limited to functional ability within CP, that is, Gross Motor Function Classification System5 or a general neurological examination,6 and lacked an assessment of coordination difficulties using a validated scale. With such a scale, the MABC-2, we observed that 38% of case children were at a higher risk of motor impairment and had lower total scores and lower scores in two of the subscales than controls. In addition, we also found that parents reported case children to walk independently 1 month later than parents of the peer group. In non-cooled children aged 5–6 years who had grade 2 NE and did not develop CP, 12% had MABC-1 scores ≤15th centile.3 We included infants with grade 3 NE and used the MABC-2 rather than MABC-1,3 which makes a direct comparison with the above study difficult.
Higher rates of hyperactivity,2 4 anxiety and depression25 have been reported in non-cooled children with moderate HIE based on parent and/or teacher questionnaires. Vision, hearing, speech, emotion and pain at 6–7 years measured using parental questionnaire was comparable between the cooled and the non-cooled groups in the (TOtal Body hYpothermia) TOBY trial.26 However, when compared with peers, we found that cooled children without CP have increased difficulties with emotional problems and overall difficulties with behaviour.
A third of the case children were already receiving additional educational support in school, indicating that their reduced performances in the psychometric and motor assessments are related to real-world educational difficulties. However, this group did not explain the overall lower scores in case children, as those not receiving extra help at school still had lower cognitive scores than the control children.
Case children were significantly shorter than their peers, with no difference in weight or BMI. This new observation requires further research to ascertain the effect of HIE on growth.
Limitations include a small sample size that come from a higher socioeconomic group than the rest of the country, and a higher proportion (70%) of males with a follow-up rate of 73%. Our study limitations are similar to that of TOBY trial childhood follow-up undertaken in the UK (males in cooled group: 70% vs 63%; study follow-up rate: 73% vs 79%)5 and these may influence generalisability. However, our study excluded non-hypoxic–ischaemic neonatal encephalopathy and represents a well-defined cohort of children who underwent TH for neonatal HIE since TH became standard practice.
In conclusion, this study shows that despite the protective effect of TH, cooled children who do not develop CP have reduced behavioural, cognitive and motor performance at 6–8 years compared with peers, with a third of the case children already receiving additional support in the classroom. These concerning findings adds weight to the argument that follow-up for children who had HIE without major problems in infancy should extend beyond 18–24 months.
References
Footnotes
Contributors RL-K: contributed to the study design, recruited participants, conducted the study, collected and analysed the data, wrote the first draft of the manuscript and approved the final version as submitted. SJ: contributed to the study design, assisted with data collection, contributed to the revisions of the paper and approved the final manuscript as submitted. JT: contributed to the study design, performed psychometric assessments, collected data, contributed to revisions of the paper and approved the final manuscript as submitted. FMC: contributed to the study design, revised the paper and approved the final manuscript as submitted. MT: formed the newborn cohort, headed the steering group, obtained funding for part of the staff salaries, contributed to study design, revised the paper and approved the final manuscript as submitted. EC: conceptualised and designed the study, obtained funding for the study and part of the staff salaries, supervised analysis, drafted the second and further versions of the manuscript, completed revisions of the paper and approved the final manuscript as submitted.
Funding We are grateful to the following for support: research project support: The Baily Thomas Charitable Fund, Luton, UK, and The David Telling Charitable Trust, University Hospitals Bristol NHS Trust, Bristol, UK. Staff salary support: The Moulton Foundation, London, UK; The Baily Thomas Charitable Fund, Luton, UK; and a Charitable donation through SPARKS, London, UK.
Competing interests None declared.
Ethics approval The study has favourable ethical opinion from the NRES Committee South West-Frenchay and the Health Research Authority (15/SW/0148).
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at The work has been presented in the Pediatric Academic Societies conference in San Francisco (2017) and the Neonatal Society Spring Meeting in London (2017).
Patient consent for publication Not required.
Linked Articles
- Fantoms