Article Text

Abstract
Aim To determine whether IntelliVue (ECG plus Masimo pulse oximeter (PO)) measures heart rate (HR) in low-risk newborns more quickly than Nellcor PO (PO alone).
Methods Unmasked parallel group randomised (1:1) study.
Results We studied 100 infants, 47 randomised to IntelliVue, 53 to Nellcor. Time to first HR was shorter with IntelliVue ECG than Nellcor (median (IQR) 24 (19, 39) vs 48 (36, 69) s, p<0.001). There was no difference in time to display both HR and SpO2 (52 (47, 76) vs 48 (36, 69) s, p=0.507). IntelliVue PO displayed initial bradycardia more often than the Nellcor (55% vs 6%). Infants monitored with IntelliVue were handled more frequently and for longer.
Conclusions IntelliVue ECG displayed HR more quickly than Nellcor PO. IntelliVue PO often displayed initial bradycardia. Infants monitored with IntelliVue were handled more often. Study of ECG in high-risk infants is warranted.
- infant
- newborn
- heart rate
- electrocardiogram
- pulse oximeter
Statistics from Altmetric.com
What is already known on this topic?
Observational studies report that ECG measures newborn’s heart rate (HR) faster than pulse oximetry (PO) in the delivery room (DR), and the International Liaison Committee on Resuscitation states its use should be considered.
Using ECG in the DR requires resources and may result in more handling of infants.
Measuring newborn’s HR with ECG does not obviate the need for PO to measure oxygenation.
What this study adds?
Although the IntelliVue (combined ECG and PO) measured HR more quickly than Nellcor PO, there was no difference in the total time for either monitor to display HR and SpO2 readings.
The IntelliVue PO displayed more episodes of initial bradycardia (HR<100 bpm) than the Nellcor.
Infants monitored with IntelliVue were handled more frequently and for longer than those monitored with the Nellcor PO.
Background
Heart rate (HR) is used to determine newly born infants’ condition, need for and response to resuscitation in the delivery room (DR). Pulse oximetry (PO) accurately and continuously displays HR1; and in 2010 the International Liaison Committee on Resuscitation (ILCOR) recommended its use during neonatal resuscitation.2 The 2015 recommendations3 stated that using ECG to measure HR may be reasonable, citing studies that reported ECG provides HR more quickly than PO.4–7 While ECG may provide HR more quickly, it does not measure oxygenation and so PO is still needed.
Introducing ECG monitoring to the DR is likely to come at a cost (in terms of monitors, consumables and staff to apply them) and may increase handling of infants.
We monitor infants in our neonatal unit with the IntelliVue X2 (Philips, Eindhoven, The Netherlands) which combines ECG and Masimo PO. We monitor infants in our DR with the Nellcor Portable SpO2 PM10N (Covidien, Boulder, Colorado, USA). We wished to determine whether IntelliVue measures HR in low-risk newborns more quickly than Nellcor in the DR.
Methods
Study design
The Speed of Heart rate Estimation using ECG and PO study was approved by our Research Ethics Committee and registered before the first patient was enrolled (ISRCTN11028739). Term infants were eligible if antenatal consent had been obtained. We enrolled infants born via elective caesarean section. Infants with congenital anomalies were excluded.
Randomisation and masking
Infants were randomly assigned (1:1) to monitoring with IntelliVue or Nellcor. The group assignment schedule was generated in blocks of four using a random number table, written on cards and placed in numbered, sealed, opaque envelopes. Envelopes were selected in order and opened by the research team prior to delivery. Neither caregivers nor outcome assessors were masked to group assignment.
Procedures
Infants were transferred to a resuscitation cot after the umbilical cord was divided. One of two investigators was randomly chosen to apply the assigned monitor.
Intervention
For infants monitored with IntelliVue, three ECG electrodes (Ambu WhiteSensor, Ambu A/S Ballerup, Denmark) were connected to the monitor before delivery, the chest was dried with a towel, and the electrodes applied before the PO sensor.8 9 When applying PO, the sensor (Masimo Neo LNOP) was applied to the infant’s right wrist before it was connected to the monitor.10 11 The monitor calculated the ECG HR by averaging the 12 most recent RR intervals; and acquired PO data with maximal sensitivity and averaged it over 10 s.
Control
For infants monitored with the Nellcor, the sensor (OxiMax neonatal SpO2, Covidien) was applied to the infant’s right wrist before connection to the monitor, which incorporates Nellcor digital signal processing technology.
Video recording
A video camera, Canon HD Legria HR200 (Canon, Tokyo, Japan), was placed above the resuscitation cot to give a field of view that included the infant, monitor and hands of the team. Outcomes were determined from video recordings and timings were obtained in second intervals.
We recorded the times taken to: (1) apply ECG; (2) display ECG HR for the IntelliVue; (3) apply and connect PO and (4) display PO HR for the IntelliVue and the Nellcor. We defined the time to apply ECG electrodes and PO sensor as the time taken from starting to apply the electrodes/sensor to the time when the circuit was complete. We defined time to display HR for each monitor as the time from the start of applying the monitor to display a HR number, not merely the ECG or plethysmograph.
Handling events, including warming, monitor application and tactile stimulation, were recorded.
Outcomes
The primary outcome was the time to first HR display. Prespecified secondary outcomes included (1) failure of monitoring (HR not displayed within 5 min), (2) time taken to apply monitor and (3) skin damage with electrodes/sensors measured visually.
Statistical analysis
Continuous variables were expressed as mean (SD) and compared with a parametric test when normally distributed; and expressed as median (IQR) and compared with a non-parametric test when the distribution was not normal. No adjustments were made for potential confounders; all were term infants delivered via elective caesarean section. Data were analysed using SPSS v24 (IBM, Armonk, New York, USA). We chose a convenience sample of 100 infants.
Results
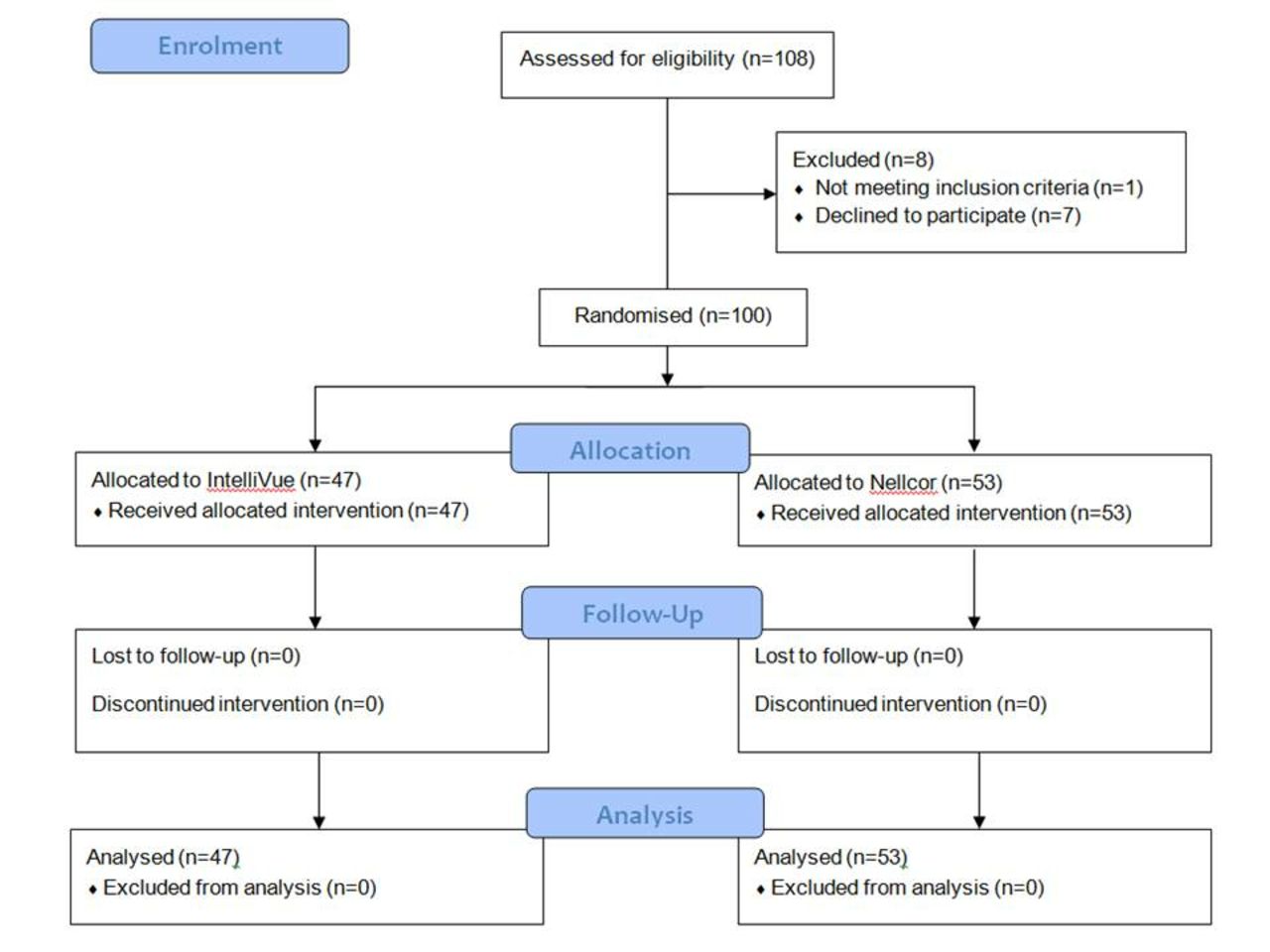
We enrolled 100 infants (figure 1); 47 were randomised to IntelliVue and 53 to Nellcor (table 1). Time to first HR was shorter with the IntelliVue ECG than the Nellcor PO (median (IQR) 24 (19, 39) vs 48 (36, 69) s, p<0.001) (table 2). There was no difference in the time for either monitor to display both HR and SpO2 data (median (IQR) 52 (47, 76) vs 48 (36, 69) s, p=0.507).

Patient recruitment.
Patient characteristics at study entry
Time (s) to apply monitors for IntelliVue and Nellcor monitors
We did not observe failure of monitoring or skin damage from electrodes/sensor placement in any participant.
Post hoc analysis
The ECG electrodes were reapplied in 21/47 (45%) infants (once in 14, twice in 6 and three times in 1 infant, respectively). This was most often due to the electrodes not sticking on the skin; but vigorous infants removed the electrodes on occasion.
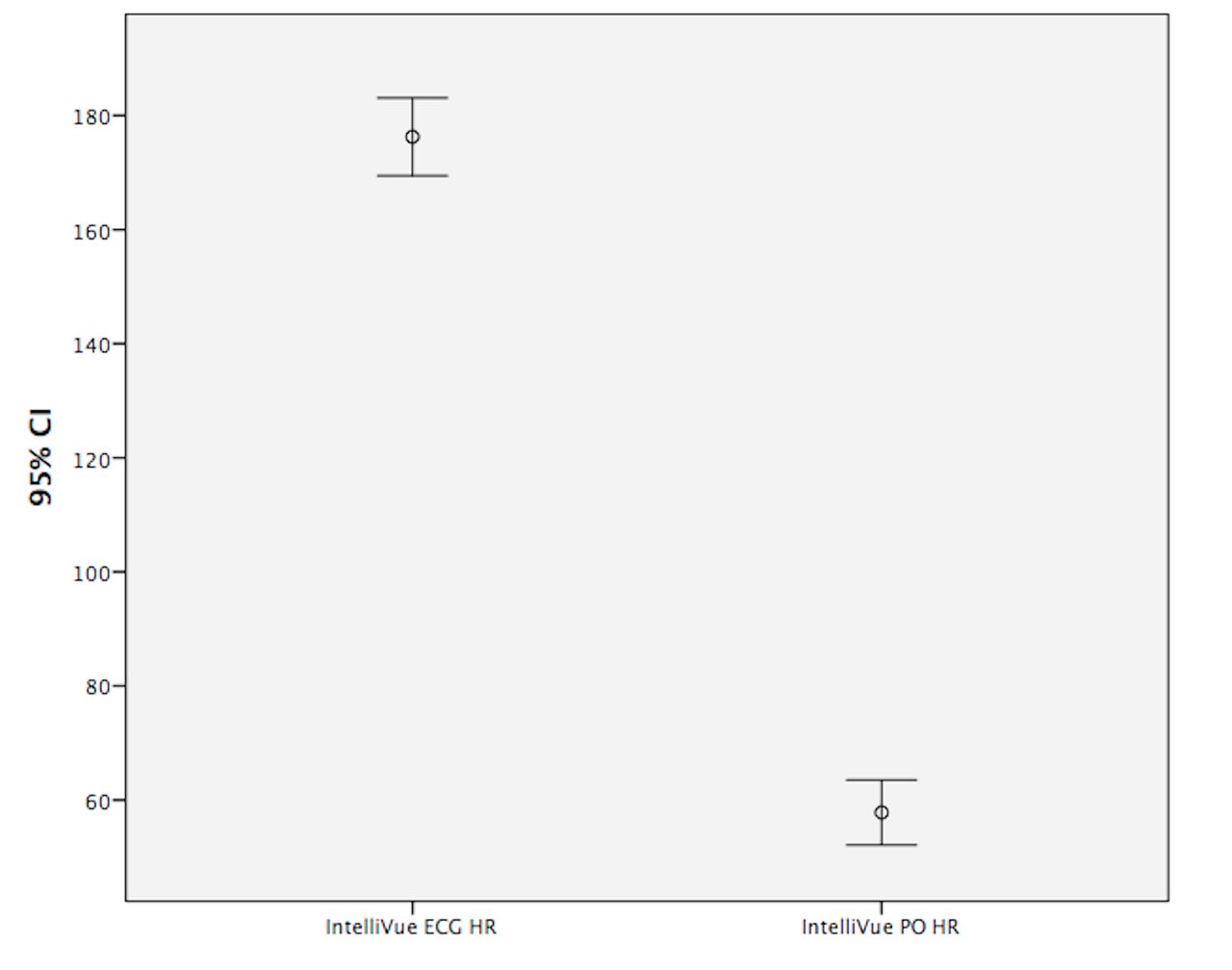
The initial PO HR displayed by IntelliVue was <100 bpm in 26/47 (55%) infants. All 26 infants had an ECG HR displayed simultaneously and none was <100 bpm. The mean (95% CI) difference between the initial ECG HR and PO HR for these infants was −118 (−126, –110) bpm (figure 2); median (IQR) time for IntelliVue PO HR to match ECG HR was 16 (2, 31) s. An initial HR<100 bpm was seen on 3/53 (6%) occasions with Nellcor; there was no ECG HR for comparison.
{kind=link}
{kind=link}
Error bars showing mean value and its 95% CI for IntelliVue ECG HR and corresponding IntelliVue PO HR for the 26 infants with initial PO HR<100 bpm. HR, heart rate; PO, pulse oximeter.
IntelliVue (Masimo PO) gave intermittent readings on 15/47 (32%) infants. For the Nellcor, data were displayed continuously after the first reading appeared in all infants.
Infants monitored with IntelliVue were handled more frequently (mean (SD) 9 (4) vs 7 (3) events, p<0.001) and for longer (104 (49) vs 85 (28) s, p<0.019; table 3) than those monitored with Nellcor.
Number and duration of handling events for infants randomly assigned to monitoring with the IntelliVue and Nellcor devices, respectively, n=98
Discussion
While technology may serve as an adjunct to help with resuscitation, good resuscitation skills are more important than any equipment. The recommendation for ECG in the DR is based on weak evidence, and has not been shown to improve outcomes. Most studies performed to date have been in low-risk infants.4–7 Katheria et al did not report any statistical or clinically important differences in vitals or time to intervention in 40 preterm infants, whether ECG data were displayed or not.12 A concern with ECG in the DR is its utility in the setting of pulseless electrical activity. In a study of asphyxiated piglets, ECG accurately identified asystole in 56% of cases while auscultation did so in 100%.13 Visual attention is often directed away from infants towards monitors during neonatal resuscitation.14 If another monitor is added into an already busy environment, it may adversely affect human performance.
More episodes of initial bradycardia were recorded with Masimo PO (IntelliVue) than Nellcor PO. Our findings are similar to those of van Vonderen et al,7 where Masimo PO HR was lower than ECG HR in the first 2 min after birth. Infants monitored with Nellcor in our study did not have ECG electrodes placed for comparison. However, there were fewer episodes of initial bradycardia with Nellcor than IntelliVue (Masimo PO). More frequent bradycardia with IntelliVue may be a problem, as discrepancies in HR between ECG and PO may be distracting.
It is unclear whether handling impacts infants positively or negatively in the DR. The term infants we studied are less likely to be negatively affected by handling than preterm infants, for whom ‘minimal handling’ is generally advised. Monitoring preterm infants with both ECG and PO might lead to increased handling and have potential adverse effects.
Conclusion
IntelliVue ECG displayed HR more quickly than Nellcor PO. IntelliVue PO often displayed initial bradycardia. Infants monitored with ECG were handled more. Study of ECG in high-risk infants in the DR is warranted.
References
Footnotes
Contributors MCM participated in study concept, study design, data collection, data analysis and writing of the first draft of the manuscript. LDeA participated in data collection. LKMcC participated in data analysis and review of the manuscript prior to submission. CPFO’D participated in study concept, study design, data analysis and writing of the manuscript.
Funding This study was supported by National Children’s Research Centre, OLCHC, Dublin (grant number: R17637).
Competing interests None declared.
Ethics approval National Maternity Hospital Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.