Article Text

Abstract
Objective To compare the resistance of interfaces used for the delivery of nasal continuous positive airway pressure (CPAP) in neonates, as measured by the generated system pressure at fixed gas flows, in an in vitro setting.
Design Gas flows of 6, 8 and 10 L/min were passed through three sizes of each of a selection of available neonatal nasal CPAP interfaces (Hudson prong, RAM Cannula, Fisher & Paykel prong, Infant Flow prong, Fisher & Paykel mask, Infant Flow mask). The expiratory limb was occluded and pressure differential measured using a calibrated pressure transducer.
Results Variation in resistance, assessed by mean pressure differential, was seen between CPAP interfaces. Binasal prong interfaces typically had greater resistance at the smallest assessed sizes, and with higher gas flows. However, Infant Flow prongs produced low pressures (<1.5 cmH2O) at all sizes and gas flows. RAM Cannula had a high resistance, producing a pressure >4.5 cmH2O at all sizes and gas flows. Both nasal mask interfaces had low resistance at all assessed sizes and gas flows, with recorded pressure <1 cmH2O in all cases.
Conclusions There is considerable variation in measured resistance of available CPAP interfaces at gas flows commonly applied in clinical neonatal care. Use of interfaces with high resistance may result in a greater drop in delivered airway pressure in comparison to set circuit pressure, which may have implications for clinical efficacy. Device manufacturers and clinicians should consider CPAP interface resistance prior to introduction into routine clinical care.
- neonatology
- respiratory
- intensive care
Statistics from Altmetric.com
What is already known on this topic?
Short binasal prongs are more effective than single/long nasopharyngeal prongs for delivery of nasal continuous positive airway pressure (CPAP) in neonates and preventing reintubation.
Short binasal prongs have a lower intrinsic resistance than single or double nasopharyngeal prongs.
Nasal CPAP masks are a commonly used alternative to short binasal prongs.
What this study adds?
Nasal CPAP mask interfaces have a lower intrinsic resistance than short binasal prongs, which may improve clinical effectiveness.
Resistance varies considerably between currently available short binasal prong devices, and is higher with smaller prong sizes and higher gas flows.
The RAM Cannula has a high resistance at all assessed sizes, and requires further evaluation before it can be recommended for CPAP use.
Introduction
Nasal continuous positive airway pressure (CPAP) has become standard practice for the management of breathing difficulties in the newborn, including transient tachypnoea of the newborn and respiratory distress syndrome.1 2 The dangers of long-term endotracheal ventilation are well described and alternatives including nasal CPAP and nasal high flow have increased in popularity.2 Provision of nasal CPAP involves the delivery of a continuous distending pressure, with the aim of supporting respiratory function by several physiological mechanisms. These include increasing functional residual capacity, maintenance of upper airway patency and reduction in work of breathing. Several nasal CPAP interfaces are described in the literature, including single and binasal prongs, nasopharyngeal prongs and nasal masks.3
The use of CPAP is now common in neonatal practice around the world, particularly in the care of preterm infants. In Australia and New Zealand in 2015, 88% of infants born very preterm (<32 weeks’ gestational age) received CPAP support during their hospital admission.4 The 2016 European Consensus Guidelines recognise non-invasive support as the optimal method of respiratory assistance for preterm infants.5 These guidelines specifically highlight the importance of CPAP, recommending ‘CPAP should be started from birth in all infants at risk of RDS, such as those <30 weeks gestation who do not need intubation for stabilisation.’ They do not make specific recommendations on choice of CPAP delivery system, but do recommend that the interface should be short binasal prongs or a nasal mask.5 The position statement of the American Academy of Pediatrics also recommends CPAP use immediately after birth as an alternative to routine intubation, but makes no specific recommendation on device or interface.6 The Cochrane Review of this subject, most recently updated in 2008 (at which time there were minimal published data assessing the use of nasal masks), recommends the use of short binasal prongs.3 There are multiple CPAP delivery systems and interfaces available, and each neonatal unit must decide which to use. Many factors come into play in making this decision, among which are included the comfort of the device, risk of nasal trauma, effectiveness of the seal created, positioning and the potential for head moulding, and cost.1 7
During CPAP delivery, the pressure is set (and sometimes measured) within the system, but the delivered airway pressure is not commonly measured during routine clinical care. Studies assessing this have shown that delivered pressure, measured in the pharynx, is lower than set pressure, typically by approximately 2–3 cm of water (cmH2O). Modern CPAP circuits are designed to have no contribution to resistance, and many include a distal pressure monitoring port to ensure target circuit pressure is maintained. However, factors beyond the circuit may contribute to pressure loss, including leak at the nose or mouth, or resistance of the interface.8 9 Given there is a direct relationship between pressure, resistance and flow, the pressure produced by the system can therefore be used as an indication of the system’s intrinsic resistance, or more specifically, that of the nasal interface.10 11 Clinical efficacy of CPAP may be dependent on effective pressure delivery. In 2002, De Paoli et al tested the resistance of CPAP devices available at that time, by measuring the pressure differential across each interface, which increases proportionately with resistance.12 In their study multiple devices were tested. They found that short binasal prongs have much lower resistance than longer nasopharyngeal prongs. Since the original study by De Paoli, more devices have become available including nasal masks and RAM Cannula.
We used the same benchtop method to assess currently available devices. We hypothesised that currently available interfaces would display similar variability in pressure differential and resistance, and that smaller devices would have higher resistance, which may have implications for clinical efficacy of CPAP.
Methods
The study was carried out in the Newborn Research Centre at The Royal Women’s Hospital, Melbourne, Australia. We tested nasal CPAP interfaces commonly used in neonatal units, including four short binasal prong devices, and two nasal mask devices currently in use, and assessed three sizes of each interface:
Hudson prongs (Hudson-RCI, Temecula, California, USA) sizes 0, 3, 5.
RAM Cannula (Neotech, Valencia, California, USA) sizes Preemie, Newborn, Infant.
Fisher & Paykel (F&P) prongs (Fisher & Paykel Healthcare, Auckland, NZ) sizes small (3040), medium (4030), large (5040).
F&P masks (Fisher & Paykel Healthcare) sizes small, medium, large.
Infant Flow prongs (Vyaire Medical, Mettawa, Illinois, USA) sizes XS, M, XL.
Infant Flow masks (Vyaire Medical) sizes XS, M, XL.
Prong dimensions were measured using digital callipers (Duratool ISO 9001:2000). Mask dimensions were measured at the narrowest internal point of airflow, where the mask attaches to the tubing. In each type of mask there were two channels for airflow—dimensions given were those measured for a single channel.
A schematic of the experimental set-up is shown in figure 1. Each interface was tested at commonly used flows of 6, 8 and 10 L/min. A flow probe was inserted in the inspiratory limb of the circuit to verify delivery of the desired gas flow. A pressure probe was inserted into the expiratory limb of the circuit to measure the generated circuit pressure. The expiratory limb was occluded so that all applied gas flow passed through the CPAP interface, which was open to atmosphere. Therefore, the generated pressure equates to the pressure differential across the interface, and is proportional to interface resistance. The exception to this set-up was the RAM Cannula, which has only a single limb, into which a single flow and pressure probe was inserted. Measured values were recorded using the NewLifeBox Neo-RSD monitor (Advanced Life Diagnostics UG, Weener, Germany), which incorporates an Avea VarFlex Flow Transducer (CareFusion, Yorba Linda, USA). The transducers were calibrated according to manufacturer’s instructions immediately prior to each study. The expiratory limb pressure was measured for 15 s at each set flow, for each size of each interface, and each measurement was repeated three times. The mean pressure for each interface and size was calculated using the three 15 s recordings.

Schematic of experimental set-up.
Results
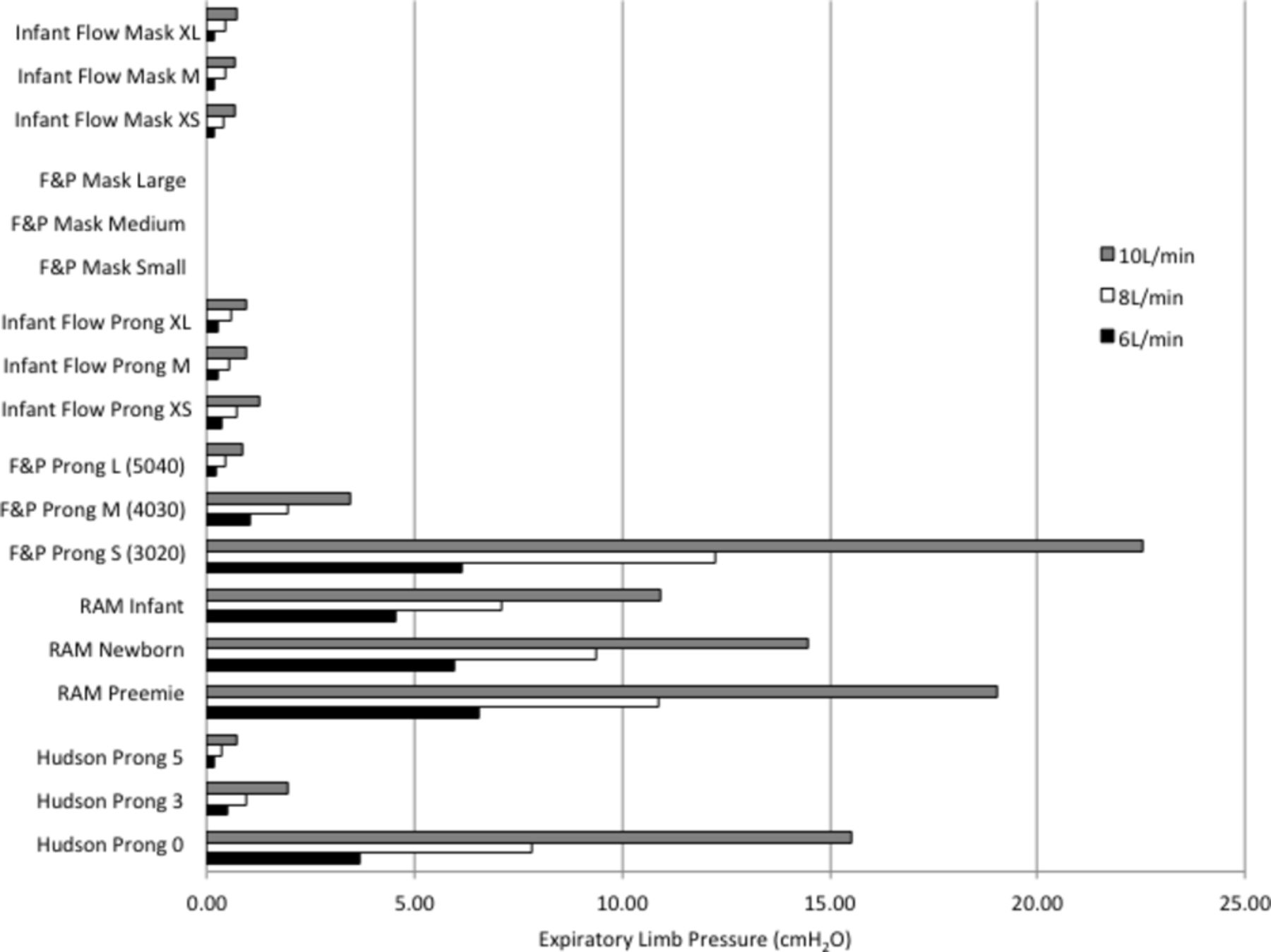
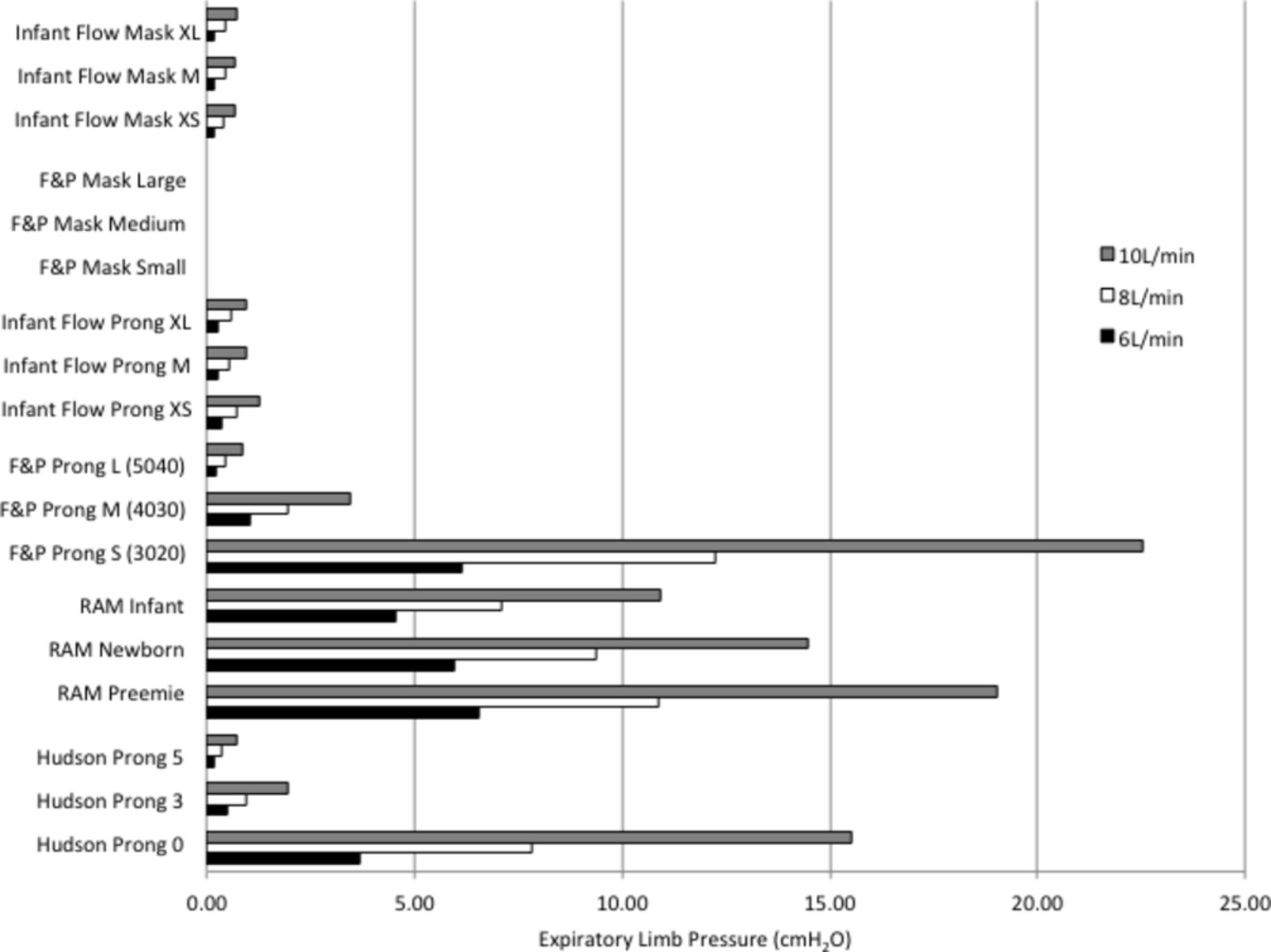
Table 1 shows the interface dimensions, and the pressure measured in the expiratory limb at three different set flows through the nasal CPAP devices. Figure 2 shows a graphical representation of these results.
Dimensions of nasal CPAP interfaces and mean expiratory limb pressure at flows of 6, 8 and 10 L/min
{kind=link}
{kind=link}
Expiratory limb pressure in nasal CPAP interfaces at flows of 6, 8 and 10 L/min. CPAP, continuous positive airway pressure.
Of all assessed prong interfaces, the Infant Flow system generated the lowest expiratory limb pressure, particularly at the smallest assessed size, indicating a lower resistance in the circuit. The Infant Flow system consistently produced low pressures across all assessed sizes and gas flows. Conversely the smaller F&P prongs and Hudson prongs produced a higher pressure than their larger counterparts, particularly at higher set gas flows.
The RAM Cannula was found to have a high resistance, with the generated pressure exceeding 4.5 cmH2O for all assessed interfaces; pressure was higher with smaller interface sizes and greater set flows.
Among the mask systems, the F&P masks had the least intrinsic resistance overall, with a pressure low enough to be unmeasurable at the expiratory limb across all sizes and all set flows. The Infant Flow masks produced very low pressures, at all assessed sizes and set flows. These were similar to the pressures noted with the Infant Flow prongs.
Discussion
There are many factors that affect the mean airway pressure delivered to an infant on nasal CPAP. These include the seal of the nasal interface, loss of pressure through the mouth, the resistance of the airways, as well as the resistance of the device.1 13 14 This study assessed the pressure differential created by the intrinsic resistance of commonly used nasal CPAP interfaces; this is of potential clinical importance as lower resistance interfaces will result in less pressure loss during delivery of gas to the infant’s upper airway.
In 2002, De Paoli et al assessed a variety of nasal CPAP interfaces used in neonatal units at the time, including a single prong, long binasal prong and short binasal prong interfaces. They found that short binasal prong interfaces had lower resistance than the longer nasopharyngeal prongs studied.12 Early studies comparing neonatal nasal CPAP delivery interfaces, in vivo as well as in vitro, showed that short binasal prongs were more effective than single nasal prong or longer nasopharyngeal prongs, and the most recent Cochrane Review on this topic concluded that short binasal prongs were more effective in preventing reintubation, and in improving short-term respiratory parameters such as oxygen requirement and respiratory rate. The authors acknowledged that there were insufficient data to draw any conclusions for longer term outcomes.3 12
In this study, we compared four types of short binasal prongs currently used in clinical practice. Our results were similar to the original measurements obtained with the Hudson prongs and Infant Flow prongs. While most binasal prongs had a higher resistance at the smallest assessed size, this was not seen with the Infant Flow prongs. This may reflect that, while the external diameter of these prongs was similar to the other small prongs, they have a greater internal diameter (2.5 mm). We also tested the more recently available F&P prongs and RAM Cannula. The generated pressure differential values with the F&P prongs were similar to those seen with Hudson prongs, with higher resistance in the smaller sizes particularly at higher flows. The RAM Cannula consistently produced pressures >4.5 cmH2O higher across all sizes and flows, higher than all other devices with the exception of the smallest Hudson and F&P binasal prongs. Although the RAM Cannula had the shortest binasal prongs of all devices assessed, the device includes a much longer section of tubing between the nasal prongs and the point of connection to the CPAP circuit, which is likely to explain the high resistance. A previous study using an artificial airway model found that delivered mean airway pressure with the RAM Cannula was 60% lower than the set nasal CPAP level, which may in part be explained by the high resistance of this device.15 This is concerning, because RAM Cannula has been adopted into routine clinical practice in many centres for the delivery of CPAP, nasal intermittent positive pressure ventilation and even nasal high-frequency ventilation,16–18 despite a lack of published data to support their clinical efficacy. The manufacturer’s recommendations state that the RAM Cannula is a device for the delivery of low or high-flow oxygen.19 However, the device is designed to interface easily with all commonly available dual-limb CPAP circuits, and several studies have described its use in this fashion.16–18 Clinicians using the RAM Cannula in this manner should be aware that its higher intrinsic resistance is likely to compromise pressure delivery to the airway in comparison with other devices that we have assessed, which has the potential to reduce the effectiveness of CPAP treatment.
As well as short binasal prongs, we assessed two types of mask interface, which are now commonly used in clinical practice. At all assessed sizes and flows, the mask interfaces were of lower resistance than the short binasal prong interfaces, with minimal pressure differential. For each brand of mask interface, F&P and Infant Flow, the pressure produced was almost identical across all sizes, suggesting the resistance is produced by the airflow channel where the interface is connected to the tubing (which is uniform in all sizes) rather than the dimensions of the masks themselves, which in all cases are too wide to make any contribution to resistance.
Recent in vivo studies comparing mask and short binasal prong interfaces have suggested that masks are similarly effective to prongs, and in some respects they may present an advantage.20–25 There are now five published randomised controlled trials comparing nasal masks and binasal prongs for CPAP administration in preterm infants. Individually, these studies have reported that the use of nasal masks is associated with a significant reduction in intubation,21 a reduction in nasal trauma,20 a reduced incidence of pulmonary interstitial emphysema20 and lower rates of moderate-severe bronchopulmonary dysplasia (BPD).23
A recently published meta-analysis including the 459 infants from these five trials reported that the risk of CPAP failure was significantly reduced with the use of nasal masks compared with binasal prongs, with a risk ratio of 0.63 (95% CI 0.45 to 0.88).26 Two pooled analyses have reported a reduction in nasal trauma with nasal masks compared with binasal prongs, either moderate-severe26 or of any grade.7 Short binasal prongs are known to cause septal trauma, which was reduced with the use of nasal masks. However, masks have been associated with nasal bridge trauma.7 20 21 24 25 This has led to the current practice in many units of cycling between masks and prongs.7 The meta-analysis conducted by Jasani et al reported no benefit with nasal mask use on other important outcomes such as BPD, death, pneumothorax or severe intraventricular haemorrhage.26
There are limitations in how these findings can be interpreted. The set-up used in this lab study was designed with the principal aim of assessing pressure differential as an indication of resistance, so it does not accurately reflect the set-up used in clinical practice, nor are the demonstrated circuit pressures an accurate reflection of those seen during standard use in the neonatal unit. We chose commonly set gas flows, but in clinical practice some gas flow passes out the expiratory limb of the circuit. Therefore, the inspiratory flow of the infant across the interface may be much lower, and result in less pressure loss, than was shown in this study. However, a study measuring respiratory function soon after birth found mean (SD) high-peak inspiratory flows of 5.7 (3.8) L/min in preterm infants, and 8.0 (5.0) L/min in term infants, so many infants can achieve the flows we tested.27
Loss of delivered pressure is potentially of clinical importance to infants treated with CPAP. Further studies in newborn infants assessing the degree of pressure loss with specific CPAP devices, at different set CPAP pressures and gas flows, might allow for the identification of a ‘correction factor’ necessary to deliver a target airway pressure in clinical practice.
Our study has shown that among commonly available nasal CPAP interfaces, there is considerable variation in resistance to gas flow, indicated by pressure differential across the interface. Nasal masks were found to have low resistance, which may optimise transmission of the set nasal CPAP pressure to the infant. In contrast, some binasal prongs had higher resistance, in particular at the smallest sizes. Device manufacturers should consider reducing the resistance of nasal CPAP interfaces as an important priority in product design.
References
Footnotes
Contributors EAG performed the data collection and analysis, and was involved in the conception and design of the study and in interpretation of the findings. She also wrote the first draft of the manuscript. JAD, PGD, AGDP and CTR were involved in the conception and design of the study, interpretation of the findings and revision of the manuscript. All authors approved the final version of the manuscript for submission.
Funding CTR is supported by the Monash University Kathleen Tinsley Research Fellowship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.
Linked Articles
- Fantoms