Article Text

Abstract
Objective To assess benefits of recording and reviewing neonatal resuscitation as experienced by neonatal care providers.
Design A qualitative study using semistructured interviews questioning neonatal care providers about their experiences with recording and reviewing neonatal resuscitation. Data were analysed using the qualitative data analysis software Atlas.ti V.7.0.
Setting Neonatal care providers working at neonatal intensive care units (NICUs) of the Leiden University Medical Center, the Netherlands, and the University of Pennsylvania School of Medicine, USA, participated in this study.
Results In total, 48 NICU staff members were interviewed. Reported experiences and attitudes are broadly similar for both NICUs. All interviewed providers reported positive experiences and benefits, with special emphasis on educational benefits. Recording and reviewing neonatal resuscitation is used for various learning activities, such as plenary review meetings and as tool for objective feedback. Providers reported to learn from reviewing their own performance during resuscitation, as well as from reviewing performances of others. Improved time perception, reflection on guideline compliance and acting less invasively during resuscitations were often mentioned as learning outcomes. All providers would recommend other NICUs to implement recording and reviewing neonatal resuscitation, as it is a powerful tool for learning and improving. However, they emphasised preconditions for successful implementation, such as providing information, not being punitive and focusing on the benefits for learning and improving.
Conclusion Recording and reviewing neonatal resuscitation is considered highly beneficial for learning and improving resuscitation skills and is recommended by providers participating in it.
- neonatology
- medical education
- qualitative research
- resuscitation
Statistics from Altmetric.com
What is already known on this topic?
Knowledge and skills often diminish shortly after neonatal resuscitation training, and activities that boost knowledge and skills are therefore recommended.
Several neonatal intensive care units (NICUs) implemented recording and reviewing neonatal resuscitation in order to improve the quality of provided support during transition at birth.
Many studies highlight the clear educational benefits of recording and reviewing actual care.
What this study adds?
Recording and reviewing neonatal resuscitation is considered highly beneficial for maintaining and improving resuscitation skills and is therefore recommended by providers participating in it.
Recording and reviewing neonatal resuscitation is considered to be a valuable tool for asking and providing objective feedback.
Insight in educational benefits of recording and reviewing neonatal resuscitation contributes to successful implementation, fitting to educational needs of a NICU.
Introduction
Neonatal resuscitation is the most provided form of acute resuscitation performed in hospitals, with 10% of all neonates needing support in stabilisation and 3% needing resuscitation.1 2 Effective neonatal resuscitation has the potential to save lives and reduce disabilities.3 However, resuscitation is complex and may not always be maximally effective. Further improvement of the quality of neonatal resuscitation is therefore pursued.
Various neonatal intensive care units (NICUs) around the world implemented the technique of recording and reviewing neonatal resuscitation in order to improve the quality of provided support during transition at birth. Although NICU staff members agree that recording and reviewing neonatal resuscitation can improve the quality of the procedure, concerns about implementation of the technique and the impact of the technique on providers are raised as well.4 These concerns create a barrier to further implementation of the technique at other NICUs.
For a wider study, we interviewed neonatal staff members who participate in recording and reviewing neonatal resuscitation in order to gain an understanding of factors that could impede or assist implementation of the technique. In this paper, we report the experienced benefits for learning and improving neonatal resuscitation and the necessity of preconditions for a safe learning environment.
Methods
For this study, which is a substudy of a project where we review factors that impede or assist wider implementation of recording and reviewing neonatal resuscitation, we conducted semistructured interviews with NICU staff members working at the NICU of the Leiden University Medical Center (LUMC), the Netherlands, and the Hospital of the University of Pennsylvania (HUP), USA. To produce maximum variation in the study sample, participants were selected through purposive sampling. Using an interview guide, participants were questioned about their experiences with recording and reviewing neonatal resuscitation.
Leiden University Medical Center
The LUMC is a tertiary-level perinatal centre with an average of 850 admissions a year. In 2009, recording and reviewing video and vital parameters of neonatal resuscitation was implemented. Since 2013, audits are conducted, discussing, among others, the technical performance and the documentation of the resuscitation. All NICU staff members are invited to participate in the meetings. Audits are prepared and chaired by the coordinator of the audit. As recording and reviewing neonatal resuscitation is considered standard care since 2016, recordings are stored as part of the medical record and parents are invited to watch the recording of their child accompanied by a provider.
Hospital of the University of Pennsylvania
The HUP is a tertiary-level perinatal centre with an average of 800 admissions a year. Since 2015, video, audio and vital parameters of neonatal resuscitation are recorded and reviewed. Providers meet for review conferences, discussing recordings of neonatal resuscitation and relevant literature. All NICU staff members are invited to participate in these meetings. Review conferences are prepared by the coordinator of the programme, together with a fellow. The video recordings are part of the hospital’s quality improvement and peer review programme and are therefore protected under the Pennsylvania Peer Review Protection Act.
The LUMC and the HUP differ both in their method of recording (figure 1) and their process of reviewing: the LUMC conducts weekly audits of 15 min, whereas the HUP conducts an hour-lasting review conferences six times a year; the HUP records audio, whereas the LUMC is still considering to record audio; the position of the camera and the amount of cameras differs between NICUs; providers of the LUMC use a respiratory functioning monitor, both during resuscitation and audits; and the HUP has a live stream that allows providers to watch resuscitations at the ward.
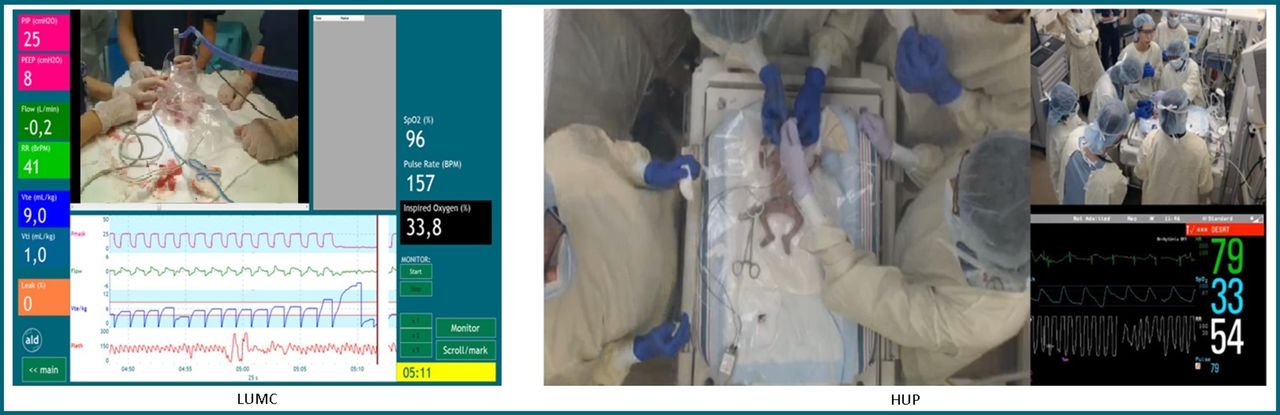
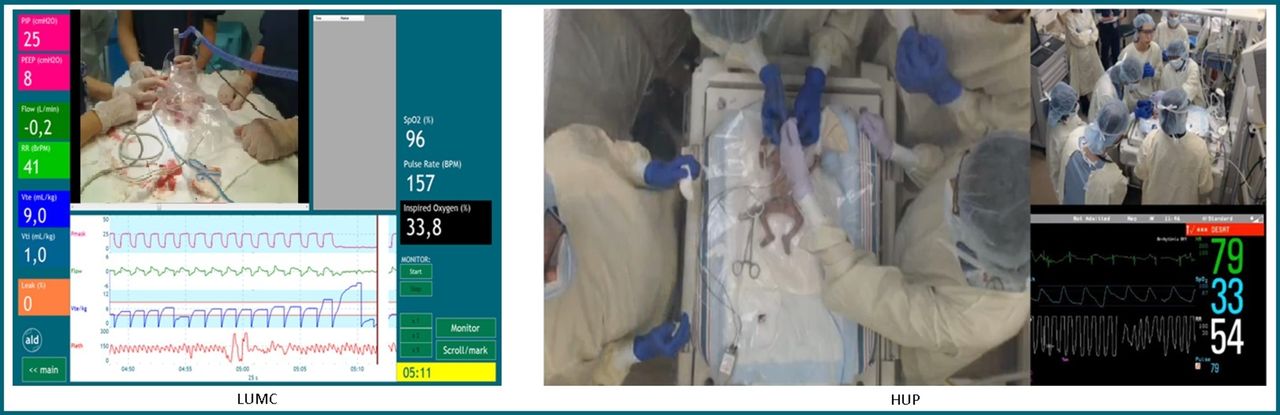{kind=link}
Recording at the Leiden University Medical Center and the Hospital of the University of Pennsylvania.
Analysis
Data collection and analysis occurred simultaneously. Interviews were audio recorded and transcribed. Transcripts were analysed in two stages. Data were manually reviewed in a process of open coding. Subsequently, data were reviewed using the qualitative data analysis software program Atlas.ti (V.7.0). Themes emerged after initial review of data, which resulted in adaption of the interview guide. In later interviews, participants were therefore directly questioned about their educational experiences.
Ethics
In concordance with laws and guidelines, a statement of no objection against execution of the study at the LUMC and the HUP was issued by the Ethics Review Committee.
Results
Interviews were conducted from 17 February to 27 December 2017. A total of 49 interviews were conducted with 48 NICU staff members, of various ages and levels of experience at the NICU. Table 1 shows participant characteristics. One participant was interviewed twice, as initial analysis of the interview showed that more information on specific themes was required. Interviews lasted between 24:19 and 93:05 (mean 45:43) min. Duration of interviews varied widely, as providers differed in their exposure to being recorded and reviewed.
Participant characteristics
Although both NICUs differ in the design of their review process, reported experiences and attitudes are broadly similar. Interviewed providers highly value recording and reviewing neonatal resuscitation, and benefits were reported by all providers, with special emphasis on educational benefits. Negative feelings and experiences were reported by many providers, but these were mostly overcome by being exposed to the procedure in a safe learning environment that allowed learning and improving. Three overarching themes were identified: recording and reviewing neonatal resuscitation as a learning activity; reported learning outcomes; and preconditions for successful implementation. These themes and illustrative quotes are presented in tables 2–4.
Recording and reviewing neonatal resuscitation as a tool for various learning activities
Educational benefits
Preconditions for successful implementation
Recording and reviewing neonatal resuscitation as a learning activity
Both NICUs implemented recording table 2 neonatal resuscitation as a research tool. Over time, the technique developed into a tool for various learning activities. To date, the technique is mostly used for the review conference (HUP) and the audit (LUMC). Recording and reviewing neonatal resuscitation is furthermore valued as a feedback tool, both for asking feedback on performance and for providing feedback on the performance of others. This was reported by junior providers and by senior providers who emphasised how reviewing resuscitations with their peers allows them to keep on learning and improving.
Providers reported to appreciate reviewing recordings of neonatal resuscitation as it allows objective feedback. Recordings are used for feedback in various settings. Feedback can be provided during plenary review meetings or on an individual base: trainees sit down with their trainers to review their resuscitations. Moreover, recordings are discussed by the team performing a resuscitation. As such, reviewing recordings also functions as a debrief tool. Recordings are furthermore used for teaching and orientation.
Reported learning outcomes of recording and reviewing neonatal resuscitation
Interviewed providers regarded recording and reviewing table 3 neonatal resuscitation as a unique way to learn and improve. It allows a different perspective than when actually being in a resuscitation, resulting in, for instance, a better perception of time. Furthermore, appropriateness of interventions and guideline adherence can be evaluated. This offers opportunities for fully assimilating guidelines of neonatal resuscitation. Providers reported that they regard recording and reviewing neonatal resuscitation as actually improving patient safety and the quality of provided care, although they realise this may be difficult to prove.
Providers reported learning from reviewing their own performance during resuscitation, as well as from reviewing performances of others. Reviewing one’s own performance is considered valuable for reassurance and self-improvement. Providers often compared reviewing actual resuscitations with debrief after simulations but considered the first more valuable, as this includes actual emotions and interventions.
Extra exposure was the most frequent reported benefit of reviewing others performing resuscitation. Being exposed to more resuscitations, especially more difficult ones or those including intubation, is considered very instructive. Furthermore, providers considered that plenary review of resuscitations allows them to keep their knowledge up to date and also provides a forum to discuss approaches. This results in more uniformity in procedures.
Providers reported various benefits of adding extra features to the review process, such as the possibility to train communication skills or crew resource management when recording audio. Although these additional features are considered valuable, implementing them should be considered carefully, as they may affect providers negatively as well.
Providers reported that recording and reviewing also affected their professional standard. Recording and reviewing taught providers to act less invasively during neonatal resuscitation. At the HUP, this led to fewer hands on the baby, while at the LUMC, this led to providers spending more time evaluating the baby’s condition before being interventional. Reviewing neonatal resuscitation furthermore contributes to a culture of openness, allowing providers to openly discuss procedures of any kind. Finally, providers stated that recording and reviewing neonatal resuscitation benefits the relationship with parents, as it instils trust and shows that the NICU is striving for quality improvement.
All interviewed providers reported at least one learning outcome. The educational value, however, differed between disciplines. Various providers emphasised the importance of a more interdisciplinary approach during review meetings, although they realise interdisciplinary reviews are challenging to implement in the daily routine at a NICU.
Preconditions for successful implementation
Providers reported negative feelings table 4 and experiences with recording and reviewing neonatal resuscitation and therefore emphasised preconditions for using the technique. Providing information, such as information about data storage and the legal status of recordings, is considered very important for providers in order to feel safe when using the technique.
Many providers reported feeling nervous when their performance was reviewed by colleagues. These feelings were reported more frequent by junior providers and providers who stated that they felt less confident about their clinical performance. Feelings of anxiety normally reduced after exposure. Providers tended to give little weight to negative feelings, as they experienced the benefits of recording and reviewing neonatal resuscitation for learning and improving the quality of the procedure. All providers stated that the benefits of the technique outweigh the concerns.
In order to prevent or reduce negative feelings and enable learning and improving, providers highlighted preconditions for a safe learning environment. Providers considered involvement, a shared group culture or mind set, focus on the educational benefits and a blame-free, shame-free environment as essential conditions for an effective review process. Creating a safe learning environment is considered an ongoing process and a shared responsibility for all providers who benefit from the technique.
When preconditions are met, recording and reviewing neonatal resuscitation is acceptable for providers and definitely recommended to implement at other NICUs. Furthermore, providers assume that recording and reviewing actual care could be valuable for other procedures, such as laryngoscopy, or at other wards, such as the emergency room or other operating rooms. Moreover, providers proposed recording consultation with patients in order to improve communication between providers and patients.
Discussion
Our study explored benefits of recording and reviewing neonatal resuscitation as experienced by neonatal care providers. Recording and reviewing neonatal resuscitation is considered highly beneficial for learning and improving resuscitation skills. All interviewed providers would definitely recommend other NICUs to implement recording and reviewing neonatal resuscitation but stated that preconditions should be met for successful implementation.
Knowledge and skills often diminish shortly after Neonatal Resuscitation Program and equivalent trainings.5 6 Matterson et al showed that resuscitation skills diminish between 2 months and 4 months after completion of neonatal resuscitation training.5 Therefore, activities that boost knowledge and skills are recommended.7 Sawyer et al and Cordero et al furthermore showed that multiple sessions are needed in order to actually improve resuscitation skills.8 9 Many NICUs therefore conduct regular simulation training of neonatal resuscitation. Various studies reported improvement of neonatal resuscitation skills after simulation trainings.5 10 11 In our study, providers considered reviewing actual neonatal resuscitation even more valuable for learning and improving clinical performance than reviewing performances after simulations.
Enhanced learning after reviewing actual resuscitation was reported by Shivananda et al and Skåre et al.12 13 Many studies highlight the clear educational benefits of recording and reviewing actual care.14 Yet, an improvement in clinical performance after reviewing recordings of actual resuscitation could not be proved.2 15–17 In these studies, clinical performance was mostly scored as correct performance of hands-on technical skills. Successful delivery room management, however, demands a combination of technical, cognitive and behavioural skills.18 Interviewed providers in our study reported learning outcomes in all these domains. For instance, when reviewing recordings, providers are trained on physiology and clinical indications (cognitive skills), and they receive objective feedback on mask technique (technical skills) and communication (behavioural skills). The improved clinical performance that interviewed providers reported experiencing may be due to the learning effect on this combination of skills. Increased self-assurance about clinical skills, which has been reported to improve resuscitation skills,10 may also contribute to the learning effect.
Based on the reported learning outcomes of recording and reviewing actual neonatal resuscitation, we propose that the technique supports maintaining resuscitation skills. Moreover, we suggest that review processes as performed by the LUMC and the HUP can be even more successful than debrief after simulation trainings, as these review processes are more concise and more frequent than most simulation training programmes. Frequently recurring short-lasting booster sessions may allow better integration in the daily routine of NICUs and extra exposure for providers. This extra exposure will especially benefit residents: in the short time of rotating at a NICU, residents will be exposed to various booster sessions. Furthermore, they are more likely to be exposed to a booster session before being hands-on again after a period of rotations at other wards. This will improve patient safety.
Although recording and reviewing neonatal resuscitation is considered valuable for improving resuscitation skills, providers of both NICUs reported that the educational value of recording and reviewing neonatal resuscitation differs strongly between NICU staff members, as it is often logistically impossible for all neonatal disciplines to join review meetings. More research is needed in order to develop a format for review meetings, fitting to the daily routine of a NICU, in which all NICUS staff members can participate, allowing all providers to improve resuscitation skills.
In our study, providers reported that recording and reviewing neonatal resuscitation is acceptable for providers. This is in accordance with previous reported experiences. For example, in 2008, O’Donnell et al reported that providers accepted recording and reviewing neonatal resuscitation as little different from being observed and instructed by senior colleagues.19 Gelbart et al reported that most staff members were willing to participate.20 Shivananda et al recently reported that 90% of questioned providers considered recording and reviewing acceptable.12 This suggests a growing base of evidence that recording and reviewing neonatal resuscitation is acceptable for neonatal care providers, supporting the recommendation for implementation made by the providers participating in our study. However, although participant selection was conducted carefully and anonymously, researcher bias may have occurred. Furthermore, providers may have been biased by positive experiences or providers may have felt constrained to report negative experiences, as the general consensus at both NICUs is very positive. Based on reported concerns about recording and reviewing neonatal resuscitation, both by providers in our study and providers in other studies, we therefore recommend cautiousness on implementation. As providers who experienced the educational benefits of recording and reviewing neonatal resuscitation generally highly appreciate the technique, we advise NICUs that plan to implement recording and reviewing neonatal resuscitation, to expose providers to the educational benefits as early as possible and to involve them in designing a review process fitting to their educational needs.
To the best of our knowledge, this is the first study to report learning outcomes of recording and reviewing neonatal resuscitation in depth. In order to provide guidance to other NICUs that are planning to implement this technique, we provide an overview of learning outcomes of various forms of review meetings for providers (table 5). This overview may be used to provide neonatal care providers insight in educational benefits and to create involvement in designing a review process fitting to educational needs of providers.
Educational benefits of various review processes
Conclusion
Recording and reviewing neonatal resuscitation is considered highly beneficial for maintaining and improving resuscitation skills. Providers using the technique would recommend other NICUs to implement it, assuming that preconditions for a safe learning environment are met. Insight in educational benefits may be used for successful implementation of a review process, fitting to educational needs of those participating in it.
Acknowledgments
We would like to thank all providers who participated in this study.
References
Footnotes
Contributors MCdB and MH drafted the initial version of the manuscript, and all authors participated in critical revision of the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding ABteP is recipient of a NWO innovational research incentives scheme (VIDI 91716428).
Competing interests None declared.
Patient consent Not required.
Ethics approval This study was reviewed by the Ethics Review Committee of the Leiden University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.