Article Text

Abstract
Background NeoTapAdvancedSupport (NeoTapAS) is a mobile application, based on a screen tapping method that calculates the heart rate (HR). We aimed to evaluate the accuracy of NeoTapAS in reliably determining HR from auscultation in a high-fidelity simulated newborn resuscitation scenario.
Methods Paediatric residents assessed HR by auscultation plus NeoTapAS in an asphyxiated term infant scenario and orally communicated the estimated HR. An external observer simultaneously documented the actual HR set in the manikin and the communicated HR.
Results One hundred and sixty HR measurements were recorded. The agreement between communicated and set HR was good (Cohen’s kappa 0.80, 95% CI 0.72 to 0.87; Bangdiwala’s weighted agreement strength statistic 0.93). Bland-Altman plot showed a mean difference between communicated and set HR values of 1 beats per minute (bpm) (95% agreement limits −9 to 11 bpm).
Conclusion NeoTapAS showed a good accuracy in estimating HR and it could be an important resource in settings with limited availability of ECG monitor.
- neonatology
- resuscitation
- mobile health
- heart rate
- accuracy
Statistics from Altmetric.com
What is already known on this topic?
Heart rate is the most important clinical indicator to evaluate the status of a newborn and to drive neonatal resuscitation.
Previous studies have shown that HR determination by auscultation can be inaccurate leading to inappropriate or delayed treatment.
What this study adds?
NeoTapAdvancedSupport is a mobile application that provides an accurate estimation of HR in a simulated scenario of neonatal resuscitation.
NeoTapAdvancedSupport could be a useful tool in resource-constrained settings and where an ECG monitor is not promptly available.
Introduction
Heart rate (HR) is the most important clinical parameter to evaluate newborn status. HR is also an indicator of the adequacy of resuscitative efforts and drives medical decisions.1
Guidelines on neonatal resuscitation recommend assessing the HR by auscultation along the left side of the chest and by counting the number of beats in 6 s and multiplying by 10.
Previous studies have shown that clinical HR determination can be inaccurate due to imprecise auscultation and/or errors in mental computation.2 3 HR can also be provided by pulse oximetry and ECG monitor.1 However, pulse oximetry is affected by motion artefacts and delay in HR display and availability of ECG is limited in delivery rooms, especially in low-resource settings.
Incorrect HR determination may lead to inappropriate or delayed treatment and to fail resuscitation.1 Using a calculator may reduce mental computation errors and increase the accuracy of HR determination. NeoTapAdvancedSupport (NeoTapAS) is a mobile application based on a screen tapping method and calculates the HR after a minimum of three taps, allowing a fast recording of HR (www.tap4life.org).
The aim of this study was to evaluate the accuracy of NeoTapAS in reliably determining HR from auscultation in a high-fidelity simulated newborn resuscitation scenario.
Methods
This is a simulation study performed at the SIMNOVA Center of the University of Piemonte Orientale in Novara, Italy. The Ethics Committee of ‘Maggiore della Carità’ Hospital (Novara, Italy) deemed that a formal ethical approval was not required since the study used manikin data. Participants gave their consent to record the scenario and to use the data.
The primary outcome was the agreement between set HR and communicated HR. The secondary outcome was participants’ satisfaction on the simulation and the app. Satisfaction was assessed using a five-item questionnaire. Each item was a Likert scale ranging from 1 (strong disagree) to 5 (strong agree).
The scenario consisted of an asphyxiated term infant needing a complex resuscitation including positive pressure ventilation, endotracheal intubation, chest compressions and emergency medications (neonatal simulator manikin: Newborn HAL S3010; Gaumard Scientific, Miami, Florida, USA). HR, respiratory rate and breath sounds were controlled remotely and could be assessed by auscultation of the thorax and observation of chest movements. Oxygen saturation via pulse oximetry (SpO2) was displayed on the bedside monitor about 40 s after the positioning of the oximeter probe whereas HR was not available. The SpO2 was not shown on the monitor when HR <60 beats per minute (bpm). The external observer provided verbal feedbacks during the scenario only if specifically required by the team and not provided by the manikin (ie, the presence of secretions). A bedside Apgar timer was available for the team.
All paediatric residents from third to fifth year of residency of the University of Piemonte Orientale who were trained on neonatal resuscitation participated in the study. They were divided into teams including three residents (one from each year of residency, in order to balance team experience) and were asked to assume the roles of team leader and assistants. After a short training on NeoTapAS and familiarisation with the manikin, participants were involved in the scenario. During each simulation, the participant responsible for HR assessment estimated the HR by listening to the praecordium with a stethoscope and simultaneously tapping the same pace on the screen of an iPad with the NeoTapAS app installed. As soon as he/she was sure of the HR displayed on the screen, he/she verbally communicated it to the team. An external observer simultaneously documented the actual HR set in the manikin and the communicated HR. All scenarios were videorecorded, stored and reviewed by the same observer to confirm the data collected during the simulation.
NeoTapAS is a free-of-charge mobile application based on a screen tapping method (www.tap4life.org) and calculates the HR after a minimum of three taps (online Supplementary video).
Supplementary file 1
Statistical analysis was performed using R V.3.3 (R Foundation for Statistical Computing, Vienna, Austria). Assuming an expected Cohen’s kappa of 0.80, at least 145 measurements were required to provide a two-sided 95% CI with width of 0.20. We finally performed 160 measurements to ensure the same number of role as HR assessor among the 40 participants. Agreement between set HR and communicated HR was evaluated using weighted Cohen’s kappa, Bangdiwala’s agreement chart and Bland-Altman plot. All tests were two-sided and a p value of less than 0.05 was considered statistically significant.
Results
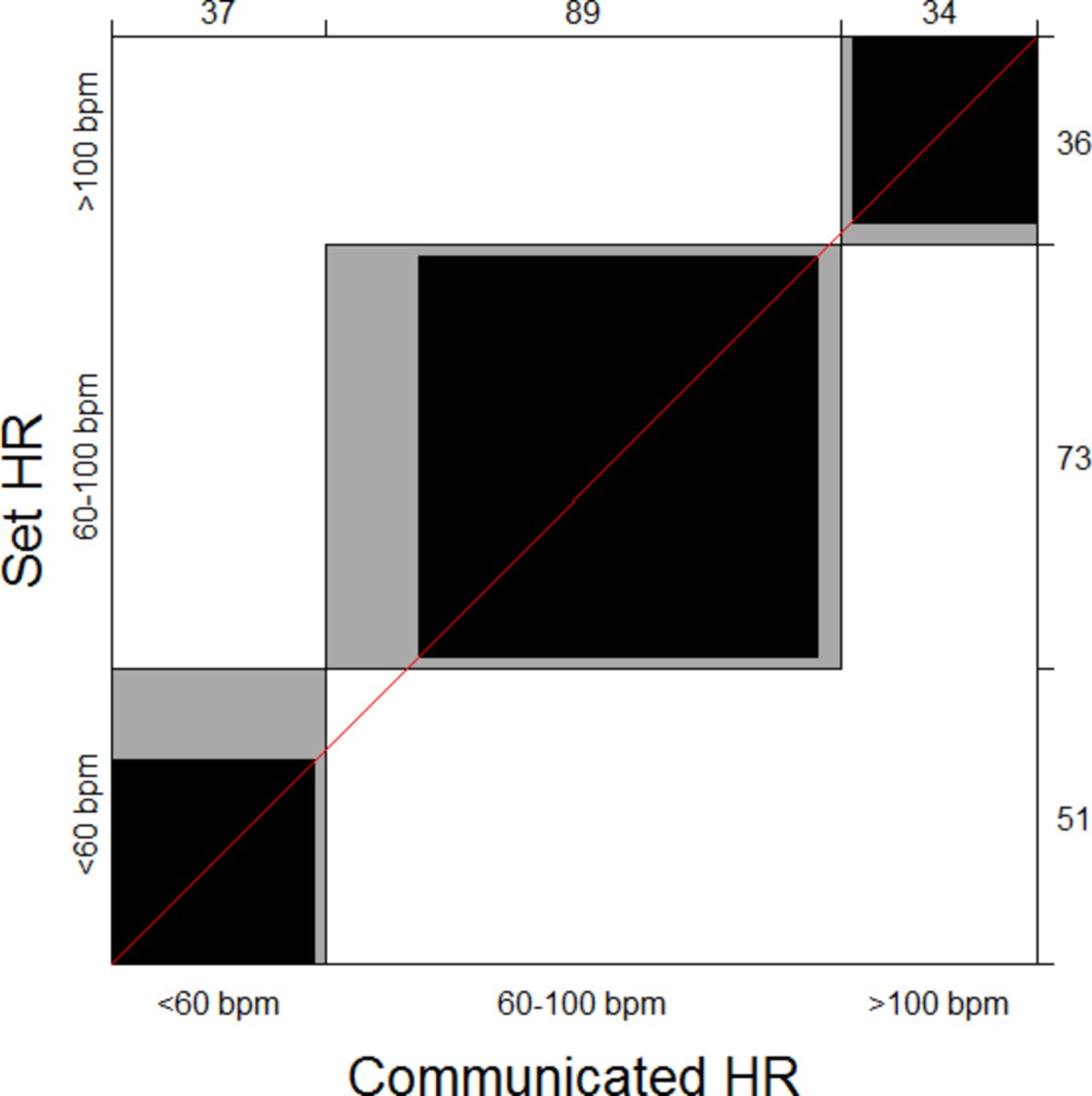
Forty residents participated in the study and 160 HR measurements were recorded. Data on HR categories as set in the manikin and as communicated by participants are shown in table 1. The agreement between communicated HR and set HR categories was good (Cohen’s kappa 0.80, 95% CI 0.72 to 0.87). Bangdiwala’s weighted agreement strength statistic was 0.93 (figure 1). Bland-Altman plot (online Supplementary figure 1) indicated a mean difference between communicated HR and set HR values of 1 bpm (95% agreement limits −9 to 11 bpm). All participants answered the questionnaire on satisfaction and agreed that NeoTapAS improved HR evaluation, while its effects on promptness of resuscitation and on decision-making were less strong (online Supplementary figure 2).
Supplementary file 2
Supplementary file 3
Distribution of HR as set in the manikin and as communicated by participants

![[fetalneonatal-2018-315408supp002.jpg]](https://fn.bmj.com/content/fetalneonatal/104/4/F440/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
![[fetalneonatal-2018-315408supp003.jpg]](https://fn.bmj.com/content/fetalneonatal/104/4/F440/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
Bangdiwala’s agreement chart between set heart rate (HR) and communicated HR categories (Bangdiwala’s weighted agreement strength statistic: 0.93). Observed and expected diagonal elements of the confusion matrix are represented by superposed black and white rectangles. Partial agreement is represented by grey rectangles.
Discussion
NeoTapAS showed good accuracy in estimating HR, although it led to partial overestimation when HR was below 60 bpm.
International guidelines on neonatal resuscitation recommend HR determination by physical examination, but this approach may lead to inaccurate HR estimation in 33%–75% of cases,2 3 potentially compromising resuscitation interventions. It is unknown whether inaccuracy is due to imprecise auscultation, wrong mental computation or combination of both. Hawkes et al reported low accuracy of tapping HR on the resuscitation table during HR auscultation.4
NeoTapAS avoids mental computation, thus potentially increasing accuracy in HR assessment. Our results indicated good accuracy of NeoTapAS, in agreement with a previous study.5 NeoTapAS limited the overestimation to 31% of cases with HR <60 bpm, while a recent simulation study reported an overestimation of 69%–83%.4 In addition, NeoTapAS was inaccurate in 6% of cases with HR between 60 and 100 bpm, and 11% of cases with HR over 100 bpm.
ECG monitor during neonatal resuscitation would provide fast and accurate HR assessment,1 but its availability is limited, especially in low-resource settings. Moreover, the use of ECG at birth may delay signal acquisition due to skin cleaning, leads placement, potential skin damage in extremely low birth weight infants and incorrect interpretation of a pulseless electric activity. Despite these limitations, ECG remains the gold standard and NeoTapAS will need to be compared with ECG in real-life scenarios.
Participants believed that NeoTapAS was useful in improving HR evaluation, while its effects on promptness of resuscitation and on decision-making were less strong. We observed no problems with the participants tapping on the screen and HR communication was very fast (median 6 s). With respect to mental calculation, NeoTapAS avoids mental computation and directly provides HR calculation, thus it can become a useful tool for healthcare staff in such stressful situation. It should be noted that our findings may be different in real-life situation. Moreover, participants were paediatric residents with limited experience in neonatal resuscitation.
In conclusion, NeoTapAS showed good accuracy in estimating HR, despite partial overestimation when HR <60 bpm. This free-of-charge mobile application could be an important resource in settings with limited availability of ECG.
Acknowledgments
We would like to thank all paediatric residents who were involved in this study.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All the data of the current study are published in the manuscript. Raw data will be made available on request.