Article Text

Abstract
Clinical assessment of an infant’s heart rate (HR) in the delivery room (DR) has been reported to be inaccurate. We compared auscultation of the HR using a stethoscope with electrocardiography (ECG) and pulse oximetry (PO) for determining the HR in 92 low-risk newborn infants in the DR. Caregivers auscultated the HR while masked to the HR on the monitor. Auscultation underestimated ECG HR (mean difference (95% CI) by −9 (−15 to –2) beats per minute (bpm)) and PO HR (mean difference (95% CI) by −5 (−12 to 2) bpm). The median (IQR) time to HR by auscultation was 14 (10–18) s. As HR was determined quickly and with reasonable accuracy by auscultation in low-risk newborns, study in high-risk infants is warranted.
- infant
- newborn
- electrocardiogram
- clinical assessment of heart rate
- pulse oximetry
Statistics from Altmetric.com
Background
Heart rate (HR) is used to assess newborn infants’ condition at birth, their need for intervention and response to resuscitation in the delivery room (DR). Clinical assessment of HR was demonstrated to be unreliable in manikin studies,1 2 and to underestimate HR measured with ECG in 26 newborns in the DR.3 While continuous and accurate HR measurement in the DR is desirable, using technology to determine HR incurs delays and cost. Auscultation of HR may be quicker than technology, and it is cheap and easy to perform. We wished to compare the accuracy and speed of assessment of HR by auscultation with that measured using ECG and pulse oximetry (PO) in newborns in the DR.
Methods
We performed this study at The National Maternity Hospital, Dublin, a university maternity hospital with a tertiary neonatal unit. While conducting a randomised study of HR estimation comparing two monitors in newborns (the SHEEP (Study of Heart rate Evaluation using Electrocardiogram) study, ISRCTN11028739), we performed a parallel study of clinical assessment of HR using auscultation on low-risk infants with the approval of our research ethics committee and parental consent. These infants were predominantly born at term by elective caesarean section. Video recordings, reviewed by one investigator, were used to record data.
For the SHEEP study, infants were randomly assigned to monitoring with the Philips IntelliVue X2 (Philips, Eindhoven, The Netherlands), which incorporates ECG and Masimo pulse oximeter, or the Nellcor Portable SpO2 Patient Monitoring System PM10N (Covidien, Boulder, Colorado, USA), in a 1:1 ratio. For each infant, one of two investigators was randomly chosen to apply the monitors. When using the IntelliVue, the investigators applied the ECG before PO4 and connected the ECG leads to the monitor before applying them to the infant.5 When applying PO for both the IntelliVue and Nellcor, investigators applied the PO sensor to the infant before connecting it to the monitor.6 In all cases, leads and sensors were applied and connected as quickly as possible immediately after one another.
As soon as an HR appeared on the monitor, a clinician was asked to auscultate the HR. Clinicians were masked to the monitor on all occasions. Clinicians were instructed to determine the HR by listening to the praecordium with a stethoscope, counting the beats over 6 s and multiplying by 10, as this is the method recommended by the Neonatal Resuscitation Program, the newborn life support course taught at our hospital.7 We defined the duration of time for clinical assessment of HR as being from when the stethoscope touched the chest until an HR value was verbalised. The time for either monitor to display HR was calculated from the start of applying the monitor to when an HR value was displayed. The HR given using clinical assessment was compared with that on the monitor at the time the stethoscope was taken off the chest. Data were analysed with SPSS (version 22, IBM, Armonk, New York). Continuous variables were expressed as mean (SD) and compared with a parametric test (eg, paired t-test) when normally distributed, and as median (IQR) and compared with a non-parametric test (eg, Wilcoxon signed-rank test) when the distribution was not normal.
Results
We studied 100 infants at a mean (SD) gestational age and birth weight of 39 (1) weeks and 3402 (561) g, respectively. Infants were monitored with the IntelliVue and Nellcor monitors on 47 and 53 occasions, respectively. HR determination by auscultation was recorded on 92 occasions (IntelliVue 45, Nellcor 47). It was performed once by a registrar (>2 years’ experience in paediatrics) and by 17 senior house officers (<2 years’ experience) for the remaining 91 infants. The time taken to determine HR by auscultation was recorded on 90 occasions (IntelliVue 45, Nellcor 45).
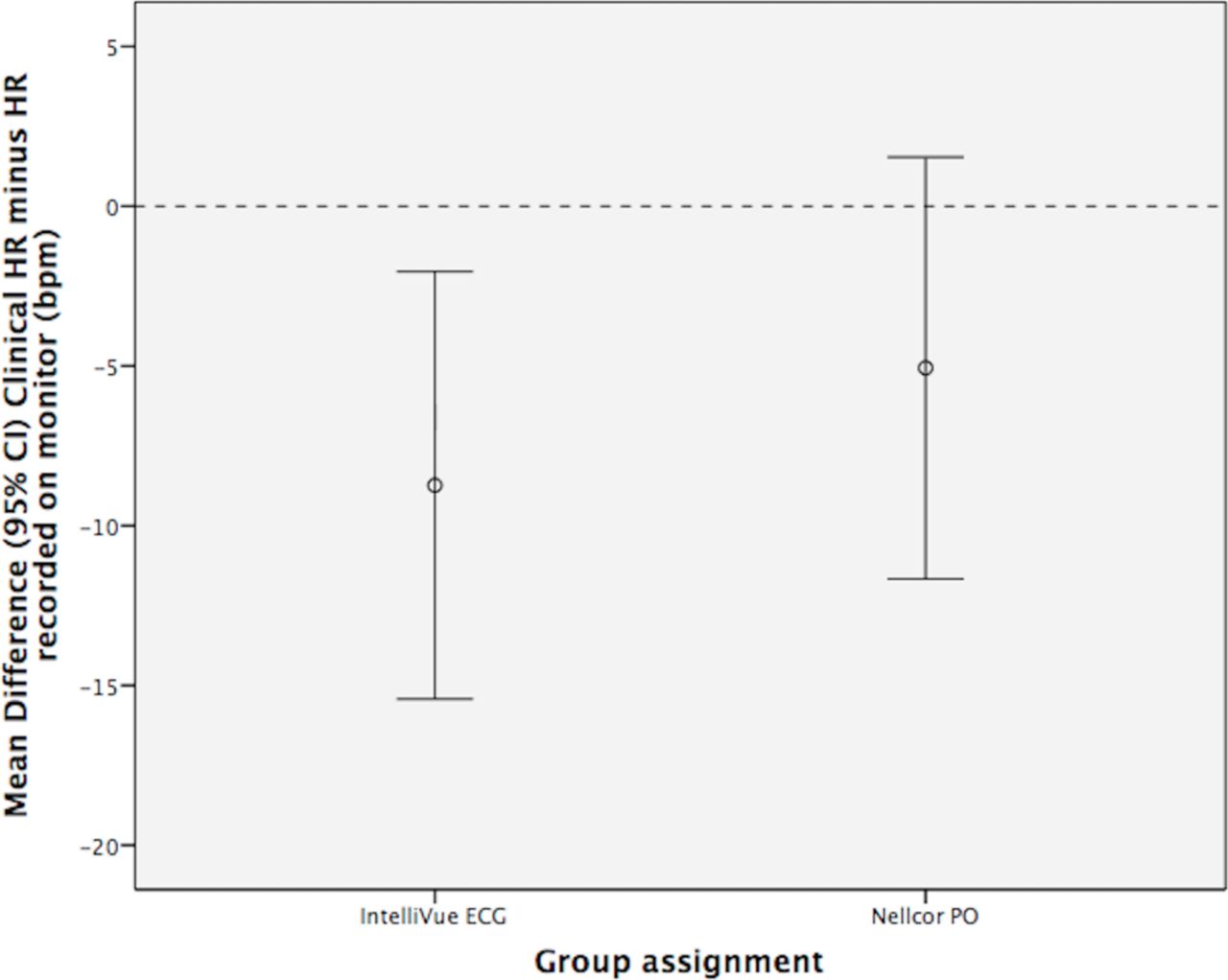
The HR was determined by the monitors at a mean (SD) of 104 (32) s of life. Caregivers started to determine the infants’ HR by auscultation at a mean (SD) of 112 (36) s of life and took a median (IQR) of 14 (10–18) s to do so. HR determined by auscultation underestimated both the IntelliVue ECG HR (mean difference (95% CI) by −9 (−15 to –2) beats per minute (bpm)) and the Nellcor PO HR (mean difference (95% CI) by −5 (−12 to 2) bpm) (figure 1).
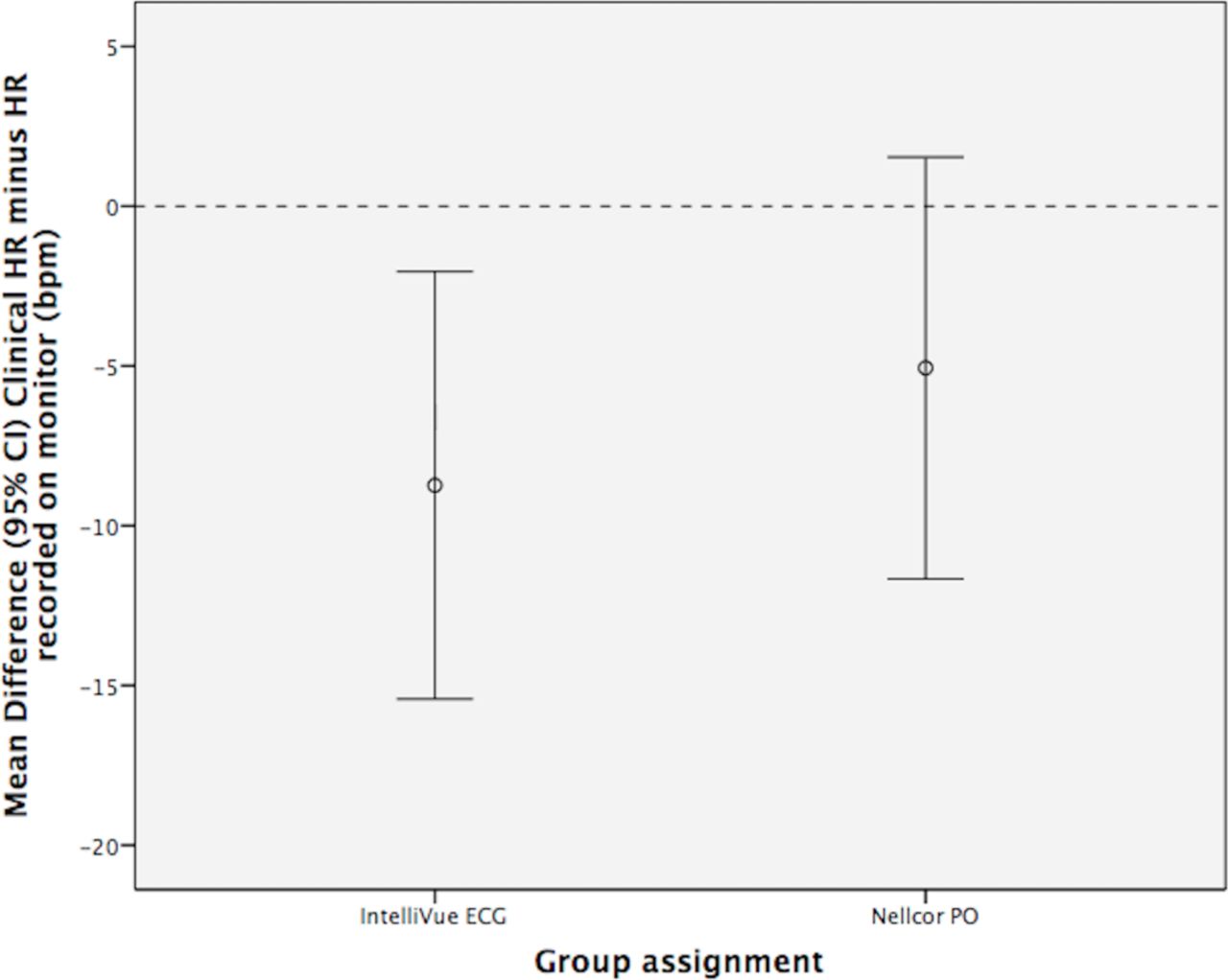
Error bars showing the mean differences (95% CIs) between heart rate (HR) determined by auscultation and by IntelliVue and Nellcor monitors. bpm, beats per minute; PO, pulse oximetry.
For the 45 infants monitored with IntelliVue, the IntelliVue took longer to determine an HR compared with clinical assessment (median (IQR) 24 (19–39) vs 14 (9–18) s, p<0.001). For the 45 infants monitored with the Nellcor for whom the time was recorded, the Nellcor took longer to determine an HR compared with clinical assessment (median (IQR) 48 (36–69) vs 14 (10–19) s, p<0.001) (figure 2).

{kind=link}
{kind=link}
A box plot showing medians, IQRs, outliers and extreme values of time (s) to determine heart rate (HR) using auscultation or the IntelliVue or Nellcor monitor, respectively. *extreme values.
Discussion
While clinical assessment underestimated the HR measured by the IntelliVue and Nellcor monitors, the mean differences were small (−9 and −5 bpm, respectively). The mean difference between the HR determined by auscultation and ECG that we found in 45 infants was less than that reported in Kamlin et al’s3 study of 26 infants (−14 bpm). We believe that the larger number of infants in our study should make our estimate more precise. Caregivers were instructed to count the HR over 6 s, multiply by 10 and verbalise the result. Given that the method we used to determine HR by auscultation might easily generate ‘ten-fold errors’, we were pleased to find that the mean difference between the HR measured clinically and by both monitors was this small. We were not surprised that caregivers took longer than 6 s to determine the HR clinically as we expected them to take a few seconds to do the arithmetic. We found that clinical assessment of HR gave an estimation of an infant’s HR more quickly than either monitor. The clinicians and the monitors did not measure the HR at precisely the same time in a ‘head-to-head’ fashion. As we wished to assess the accuracy of HR determined clinically, we needed a value to compare it with. The HR was therefore clinically assessed after the HR had been determined by the monitor. As HR may be more difficult to determine the sooner after birth it is done, it is possible that the monitors might have been disadvantaged somewhat. However, as the HR was determined by the monitors shortly after birth and determined clinically very shortly afterwards, we believe that this comparison is largely valid. Infants in our study were born at term, were not anticipated to need resuscitation and none had an HR <100 bpm; we cannot therefore comment on the performance of auscultation in preterm infants, in those anticipated to need resuscitation or in the setting of bradycardia.
The 2015 International Liaison Committee on Resuscitation stated that during neonatal resuscitation, the use of ECG for assessment of HR might be reasonable on the basis that it displays the HR more quickly than PO.8 The use of ECG in the DR has associated costs, in terms of resources and handling of the infant. If clinical assessment of HR can provide a reasonably accurate HR more quickly than ECG, ECG monitoring may become less attractive. While auscultation of the HR is usually intermittent, it is cheap, easy to perform and not dependent on technology or a power source. Further study of clinical assessment of HR in high-risk infants and during episodes of bradycardia is warranted.
Footnotes
Contributors MCM participated in study concept, study design, data collection, data analysis and writing of the first draft of the manuscript. LDA participated in data collection. LKM participated in study design, data analysis and revision of the manuscript. CPFO participated in study concept, study design, data analysis and revision of the manuscript.
Funding MCM is supported by a Clinical Research Fellowship from the National Children’s Research Centre (R17637).
Competing interests None declared.
Patient consent Not required.
Ethics approval National Maternity Hospital Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.