Article Text

Abstract
Background Antibiotic resistance is a worldwide problem. We describe 25 years of responsible antibiotic use in a tertiary neonatal unit.
Methods Data on neonatal infections and antibiotic use were collected prospectively from 1990 to 2014 at a single tertiary Sydney neonatal intensive care unit attached to a maternity unit. There are approximately 5500 deliveries and 900 nursery admissions per year.
Results The mean annual rate of late-onset sepsis was 1.64 episodes per 100 admissions. The mean number of late-onset sepsis episodes per admission to the neonatal unit decreased by 4.0% per year (95% CI 2.6% to 5.4%; p<0.0001) and occurred particularly in infants born weighing <1500 g. No infants with negative cultures relapsed with sepsis when antibiotics were stopped after 48–72 hours. Antibiotic use decreased with time. The proportion of colonising methicillin-resistant Staphylococcus aureus isolates decreased by 7.4% per year (95% CI 0.2% to 14.1%; p=0.043). The proportion of colonising Gram-negative bacilli isolates resistant to either third-generation cephalosporins or gentamicin increased by 2.9% per year (95% CI 1.0% to 4.9%; p=0.0035). Most were cephalosporin-resistant; gentamicin resistance was rare. An average of one baby per year died from late-onset sepsis, the rate not varying significantly over time. The mortality from episodes of late-onset sepsis was 25 of 332 (7.5%).
Conclusion Stopping antibiotics after 2–3 days if neonatal systemic cultures are negative is safe. However, it does not prevent the emergence of cephalosporin-resistant Gram-negative organisms.
- Antibiotic stewardship
- Nosocomial infection
- MRSA
- Antibiotic resistance
Statistics from Altmetric.com
What is already known on this topic?
Prolonged use of broad-spectrum antibiotics in an intensive care setting is one known factor in selection of antibiotic resistance.
There is limited evidence that antibiotics can be stopped after 2–3 days if neonatal systemic cultures are negative.
What this study adds?
Antibiotics were stopped safely after 2–3 days for 90% of neonates in a tertiary neonatal unit.
The incidence of late-onset sepsis fell over time, particularly in infants born weighing <1500 g.
Responsible antibiotic use did not prevent the emergence of resistant Gram-negative bacilli.
Introduction
The incidence of infection is higher in the neonatal period than at any other age.1 Early onset neonatal infection is thought to be primarily due to heavy exposure to micro-organisms in the maternal genital tract, usually acquired by ascending amniotic infection or haematogenous spread, while late-onset neonatal infection is primarily due to exposure to micro-organisms through invasive procedures. In both instances the susceptibility to infection is compounded by relative immunological immaturity and the incidence of infection is inversely related to gestational age and birth weight.1
Antibiotic resistance is a growing problem worldwide, particularly in low/middle-income countries.1–5 This is especially true for late-onset neonatal sepsis in neonatal units,2–5 but there is growing evidence of the occurrence in low/middle-income countries of early onset neonatal infections due to multi-resistant organisms, presumably acquired from the maternal genital tract.6 ,7
Antibiotic resistance is an example of natural selection.8 Micro-organisms have evolved antibiotic resistance genes over millions of years, but do not usually express these genes, presumably because to do so carries too great a metabolic cost. Prolonged exposure to broad-spectrum antibiotics, however, may select for host microflora with resistance genes they are able to express. The corollary is that reduced use of broad-spectrum antibiotics may reduce the antibiotic pressure selecting for resistance and, therefore, the incidence of antimicrobial resistance.8
There is moderate evidence from longitudinal studies that it is safe to stop empiric antibiotics after 2–3 days if a neonate has negative blood cultures and is improving clinically.9–11 In this paper we analyse the pattern of antibiotic use and infections over 25 years in a tertiary neonatal unit attached to a maternity unit.
Methods
One of the authors (DI) has collected data prospectively on neonatal infections, colonisation and antibiotic use over 25 years from 1990 to 2014 at the neonatal unit at Royal Prince Alfred (RPA) Hospital, Sydney (formerly King George V Hospital). RPA covers an inner city, multicultural population. It accepts in utero and ex utero transfers from around the state and overseas. The neonatal unit is attached to a tertiary maternity hospital with approximately 5500 deliveries per year. It provides a level 5 neonatal intensive care unit (NICU) service with an average of approximately 900 admissions to the nursery each year. The unit consists of 34 beds, comprising 10 level-3 beds (ventilation or ‘NICU’) and 24 level-2 beds (divided into two sections, the high-dependency unit and the special care nursery). Data were only able to be collected for 5 months in 2006 and for 6 months in 2012.
The criterion for starting antibiotics was clinically suspected sepsis and all babies routinely have blood cultures sent prior to commencing antibiotics. Throughout the 25 years, systemic neonatal infection was defined as a positive culture of a likely pathogen from blood or cerebrospinal fluid (CSF).12 ,13 If the organism isolated was a potential pathogen, the episode was only considered to be true sepsis if there was supportive evidence of a significant change in one or more haematological parameters (total peripheral white blood cell count, immature-to-total white blood cell count or platelet count) or an elevated serum C reactive protein (CRP) or the organism was isolated from more than one systemic culture.12 ,13 Infections were defined as early onset if occurring within 48 hours of birth and as late-onset if the first positive culture was more than 48 hours after birth.12 ,13 Deaths were attributed to sepsis if systemic cultures grew a significant pathogen and the baby died acutely or the infection was thought to have contributed significantly to the baby's demise.
The same empiric antibiotic regimen was used throughout the 25 years: penicillin and gentamicin for suspected early onset sepsis and vancomycin and gentamicin for suspected late-onset sepsis (LOS). The serum CRP was frequently measured at the start and end of treatment but was not used as a basis for starting or stopping antibiotics, which was primarily a clinical decision. In general, antibiotics were stopped after 2–3 days of treatment if systemic cultures were negative and the baby is well, regardless of the CRP results. We would stop antibiotics on an individual child whose systemic cultures were negative and who was improving or clinically stable. Broad-spectrum antibiotics, such as ticarcillin-clavulanate or meropenem were reserved for infants with positive cultures with resistant organisms and were rarely used.
Surveillance swabs from the endotracheal tube or nasopharynx of infants requiring respiratory support were cultured once a week using standard microbiologic techniques. In 1998, during an outbreak of an extended-spectrum β-lactamase-producing Klebsiella oxytoca, weekly rectal swabs or faecal specimens were sent of all infants in the unit, not just those on artificial ventilation, for some weeks until the outbreak ceased. Colonising Staphylococcus aureus was reported as sensitive to methicillin or as resistant (MRSA). Colonising Gram-negative organisms were reported as sensitive or resistant (including inducible resistance) to third-generation cephalosporins (usually cefotaxime/ceftriaxone but ceftazidime for Pseudomonas species which are inherently resistant to cefotaxime/ceftriaxone) and as sensitive or resistant to gentamicin.
Antibiotic use was recorded prospectively. A ‘course’ of antibiotics was defined as having been completed when antibiotics had been stopped for at least 48 hours. If antibiotics were resumed within 48 hours of stopping, they were considered to have been given continuously, for example, if given for 2 days, stopped for 1 day, then continued for 3 more days, we would record this as a 5-day course.
Data were tabulated. Statistical analyses were conducted in SAS (V.9.3). Regression models were used to test for trends over time, with year as a continuous predictor. Sepsis episodes in each year were analysed using Poisson regression with the number of admissions as exposure variable. Mean duration of antibiotic use, percentage of babies on antibiotics and proportion of time on antibiotics in each year were analysed using linear regression. Drug resistance was analysed using logistic regression. There was no adjustment made for multiple statistical comparisons.
Changes in the distribution of birth weight over time were tested using logistic regression models for weight categories <1000 g, 1000–1499 g, 1500–2499 g and ≥2500 g. To explore the impact of birth weight on LOS, we performed logistic regression with year as a continuous predictor, weight category and their interaction, then separate models in each weight category with year as a continuous predictor.
De-identified clinical data were collected as part of a larger study on neonatal infections conducted by the Australasian Study Group for Neonatal Infections, which is approved by the Royal Alexandra Hospital for Children ethics committee (approval number 93060).
Results
Over the 25-year study period, there were 20,962 total admissions to the neonatal unit. There were 8133 episodes of suspected early or late sepsis treated with antibiotics. There were 332 episodes of proven LOS (positive blood and/or CSF culture after 48 hours of age). The annual rate of LOS was between 0.33 and 3.80 episodes per 100 admissions, with an overall mean of 1.64 episodes per 100 admissions. The mean number of LOS episodes per admission to the neonatal unit decreased by 4.0% per year (95% CI 2.6% to 5.4%; p<0.0001) (figure 1). The decreased incidence occurred for both Gram-positive and Gram-negative infections. There were no episodes where infants whose antibiotics were stopped after 48–72 hours because blood cultures were negative relapsed within 48 hours with culture-proven sepsis.
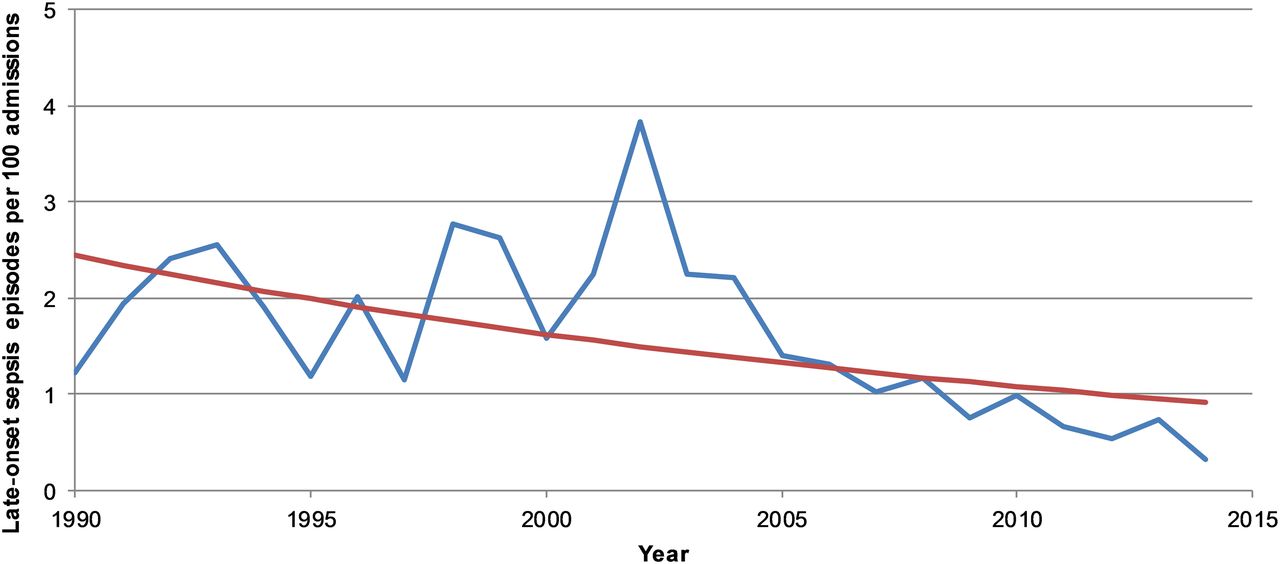
Graph showing the annual rate of episodes of late-onset sepsis per 100 admissions to the neonatal unit at Royal Prince Alfred Hospital, Sydney, 1990–2014.
The mean duration of all antibiotic courses, for both early and late suspected sepsis, decreased by 0.061 days/year (95% CI 0.045 to 0.077; p<0.0001) (figure 2). In 2013, 84% of infants received antibiotics for ≤48 hours and 90.1% for ≤72 hours; in 2014, the figures were 85.8% for ≤48 hours and 90.9% for ≤72 hours. The babies with negative cultures for whom antibiotics were continued were considered clinically unstable and most were infants receiving ventilator support and <1500 g birth weight.

Graph showing the mean duration of antibiotic use, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014.
The mean percentage of all babies admitted to the neonatal unit who ever received antibiotics for either suspected early onset sepsis or LOS increased by 0.27% per year (95% CI 0.095 to 0.44%; p=0.004) (figure 3).
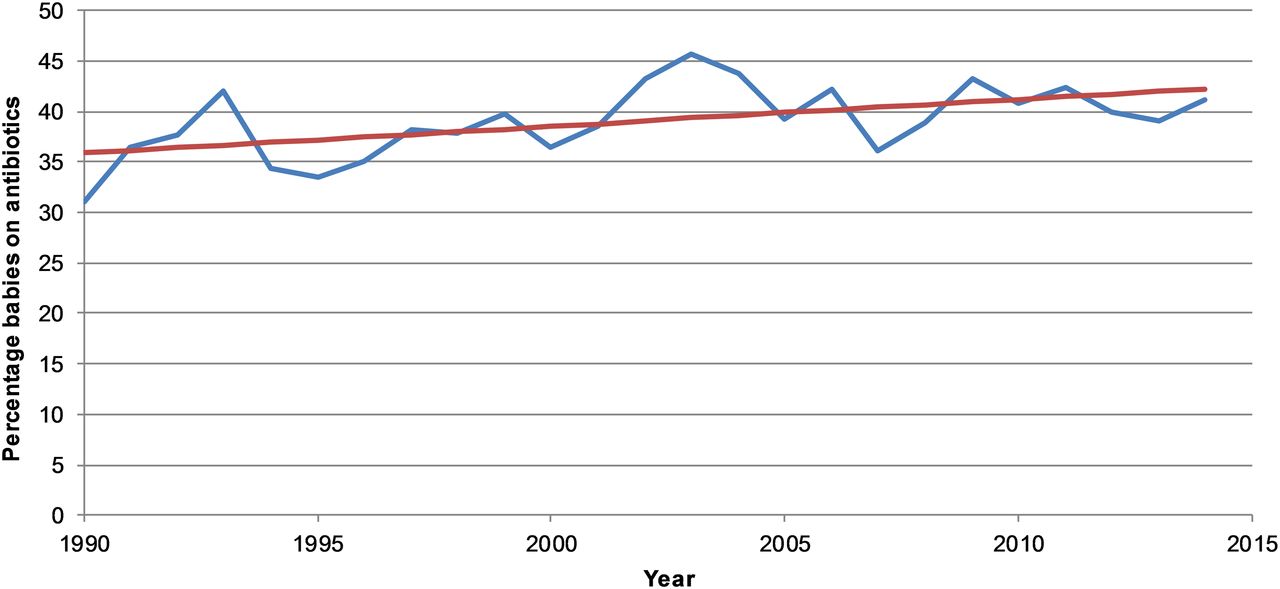
Graph showing the percentage of babies receiving antibiotics, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014.
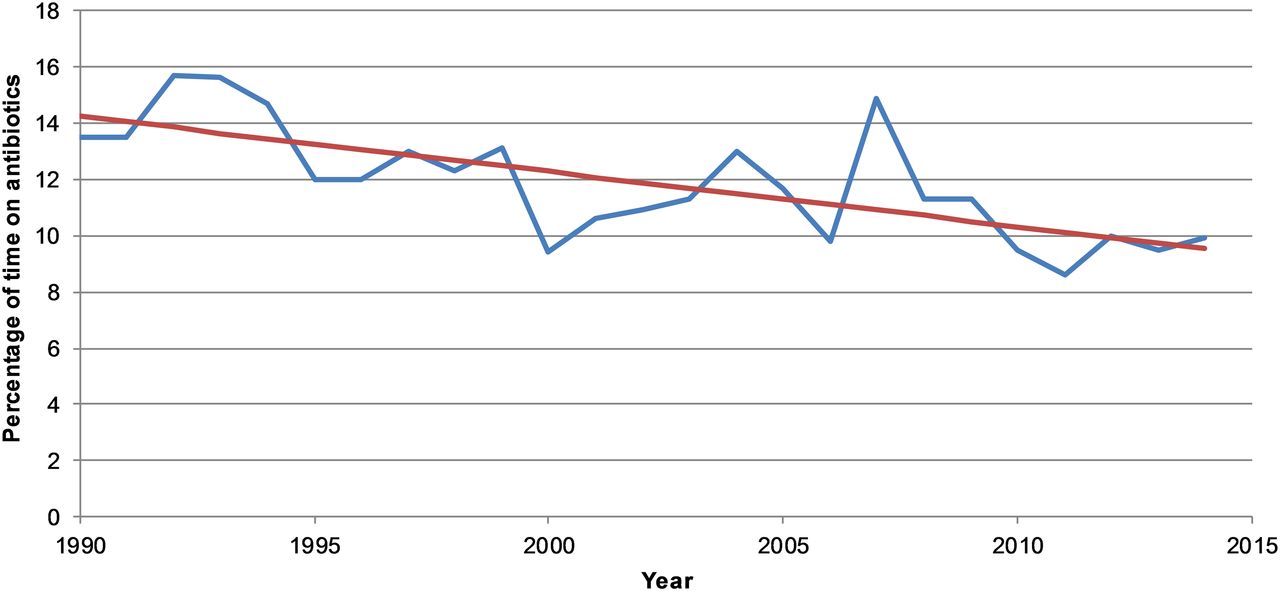
Time spent on antibiotics as a percentage of the time they spent on the unit (expressed as the sum of baby-days on antibiotics/total baby-days in the neonatal unit) decreased by 0.20% per year (95% CI 0.11 to 0.28; p<0.0001) (figure 4).

Graph showing the percentage of time on antibiotics, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014.
The organisms responsible for LOS will be analysed and reported separately, but the distribution of organisms was similar over time.
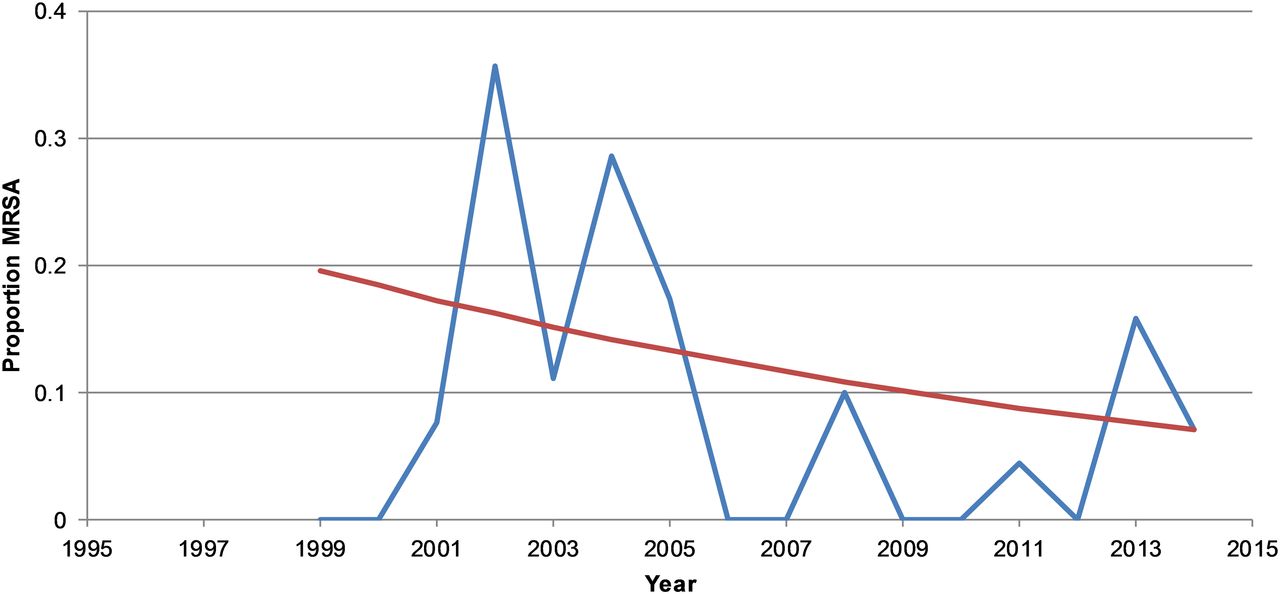
The proportion of isolates of MRSA decreased over time. The odds of resistance decreased by 7.4% per year (95% CI 0.2% to 14.1%; p=0.043) (figure 5).

Graph showing the proportion of Staphylococcus aureus isolates resistant to methicillin, Royal Prince Alfred Hospital neonatal unit, Sydney, 1999–2014. MRSA, methicillin-resistant Staphylococcus aureus.
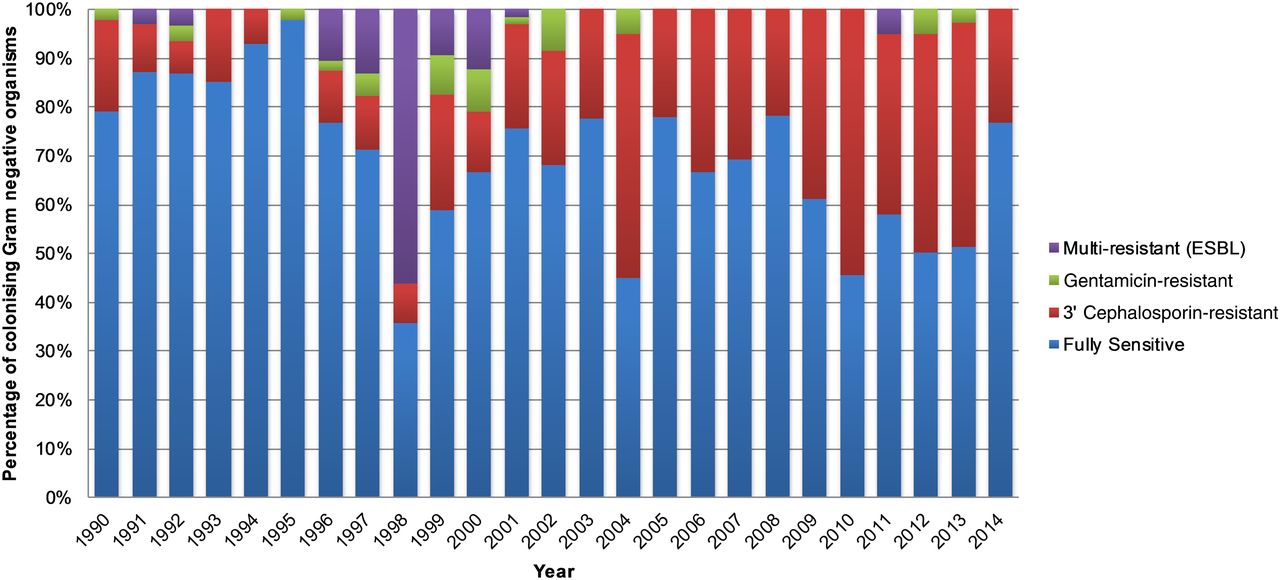
The proportion of colonising Gram-negative bacilli isolates resistant to either third-generation cephalosporins or gentamicin increased over time (figure 6). The odds of a Gram-negative isolate being resistant increased by 2.9% per year (95% CI 1.0% to 4.9%; p=0.0035). This was mostly driven by cephalosporin resistance (figure 7); gentamicin resistance was rare.

Graph showing the proportion of colonising Gram-negative (GN) bacilli with gentamicin or third-generation cephalosporin resistance, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014.
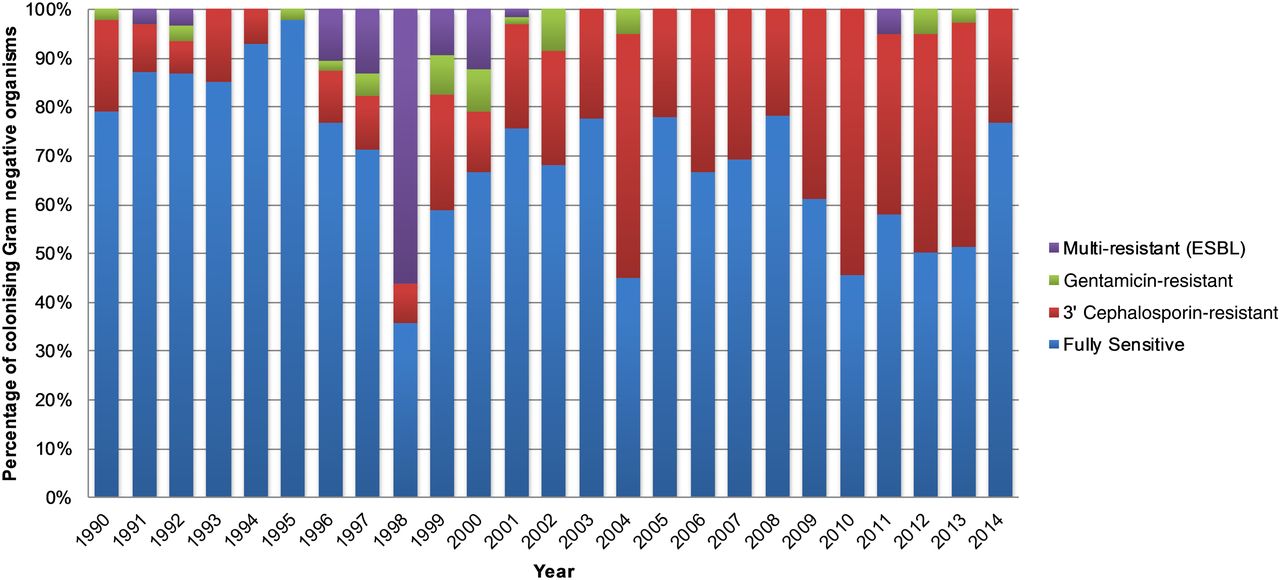
Graph showing the resistance patterns of colonising Gram-negative organisms, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014. ESBL, extended-spectrum β-lactamase.
The mortality from episodes of LOS was 25 of 332 (7.5%) or one per year on average (see table 1). The odds of LOS deaths per LOS episode increased by 0.7% per year over the period of the study but there was no statistical evidence that the observed change was greater than expected by chance (OR for fatal LOS 1.007 per year, 95% CI 0.944 to 1.074, p=0.8).
Outcome of episodes of late-onset sepsis (LOS)
The overall proportions of admissions by birth weight were as follows: <1000 g: 5.2% of 20 792 total admissions; 1000–1499 g: 8.3%; 1500–2499 g: 33.1% and >2499 g: 53.3%. There was strong evidence of changes in the birthweight distribution of admitted babies over the period of the study, with the odds of babies being in the heaviest weight category decreasing by 1.6% per year (OR=0.984 per year, 95% CI 0.980 to 0.988, p<0.0001).
There was strong evidence of an interaction between birthweight category and calendar time on the odds of LOS (interaction p value=0.0006), meaning that the changes in LOS over time differed between the birthweight categories. Separate models in each weight category showed evidence of decreases in LOS over time in all weight categories except the heaviest (figure 8). For babies <1000 g, OR was 0.89 (95% CI 0.87 to 0.92) per year (p<0.0001). For babies 1000–1499 g, OR was 0.93 (95% CI 0.90 to 0.97; p=0.0004). For babies 1500–2499 g, OR was 0.93 (95% CI 0.88 to 0.98; p=0.012). For babies ≥2500 g, OR was 1.05 (95% CI 0.97 to 1.03; p=0.19).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Graph showing the annual rate of late-onset sepsis episodes by birth weight, Royal Prince Alfred Hospital neonatal unit, Sydney, 1990–2014.
From 1992 to 2003 inclusive, the proportion of infants in each weight bracket who developed LOS at RPA Hospital was as follows: <1000 g: 138 of 496 infants (27.8%); 1000–1499 g: 47 of 915 (5.1%); 1500–2499 g: 19 of 3141 (0.6%) and ≥2500 g: 7 of 5741 (0.1%). From 2004 to 2014 inclusive, the proportions were as follows: <1000 g: 48 of 539 infants (7.4%); 1000–1499 g: 21 of 810 (2.6%); 1500–2499 g: 9 of 3744 (0.2%) and ≥2500 g: 10 of 5350 infants (0.2%).
Discussion
Antimicrobial resistance is a major problem worldwide, but particularly in low/middle-income countries. It is estimated that in 2012, of the deaths due to neonatal sepsis, 214 500 (95% CI 139 100 to 318 400) were attributable to resistant pathogens.14 Most neonatal deaths occur in low/middle-income countries where the problem of antimicrobial resistance is greatest. There are many reasons for this, including lack of access to diagnostics, because of which infections are often treated empirically on clinical grounds.15 ,16
We present 25 years of data from a single tertiary centre in Australia with good access to diagnostics to support previous studies suggesting that a policy of routinely stopping antibiotics after 2–3 days if systemic cultures are negative is safe.9–11 We do not use acute phase reactant measurements such as serum CRP as a routine basis for deciding whether or not to stop antibiotics. Antibiotics are ceased in over 90% of babies within 3 days if cultures are negative. We actually used fewer antibiotics over time overall, because although a greater proportion of babies were started on antibiotics, antibiotics were stopped earlier and the mean duration of antibiotic courses as well as proportion of time babies spent on antibiotics decreased. The mean annual rate of LOS of 1.64 episodes per 100 admissions compares favourably with the usual reported rate from Western tertiary neonatal units of 2%–5% of admissions.13 ,17–23 The reduction in the rate of LOS was mostly marked in the smallest babies and occurred although the proportion of admitted babies who were low birth weight increased significantly over time. Multiple factors are likely to have contributed to the observed decrease in LOS. Infection with coagulase-negative staphylococci, the predominant cause of LOS, is associated with poor infection control, prolonged central venous catheterisation and artificial ventilation. Over the 25 years, there has been a growing focus on infection control policies, with an emphasis on improved hand hygiene and improved care of central lines. Surfactant use has been refined, permitting earlier extubation, and enteral feeds have been introduced sooner allowing earlier cessation of parenteral nutrition. Our rate of LOS is low compared with most other countries.24 This could be due to case-mix, but one likely explanation is our restrictive definition of LOS which rigorously excludes contaminants.
Mortality due to LOS did not change significantly over the 25 years, although there were just two deaths in the past 9 years. We conclude that it is usually safe to stop empiric antibiotics after 2–3 days if systemic cultures are negative and the baby is clinically stable. This, however, is not necessarily practised in other neonatal units, where clinicians often continue antibiotic therapy despite negative cultures for ‘presumed late onset sepsis’, sometimes basing this on CRP results. For example, in a multicentre retrospective US study of 4039 infants <1000 g birth weight with negative systemic cultures, the median duration of antibiotics was 5 days.25 Furthermore, after attempting to adjust for confounding variables including severity of illness, infants who received 5 or more days of antibiotics despite negative cultures had a 50% increase in mortality compared with infants who received <5 days (p<0.001) and a 42% increased risk of necrotising enterocolitis (p<0.001).25 These data could suggest that prolonged antibiotic use actually harms extremely low birthweight infants, presumably by altering their intestinal microflora.
The proportion of a neonate's admission spent receiving antibiotics reduced significantly over the study period. This is a unique measure that has not been used in other studies. It is an important data point as it demonstrates the average degree of exposure to antibiotics for each neonate while in the unit. Even though a greater proportion of neonates received antibiotics over time, their overall exposure is minimised as they are not on antibiotic therapy for the bulk of their admission and as such are less susceptible to the harmful effects of antibiotics and contribute less to developing antimicrobial resistance. This measure is also a useful marker of a unit's approach to antibiotic use and represents a useful benchmark for comparing different units.
We observed a gradual increase in the proportion of all colonising Gram-negative bacillary isolates resistant to either a third-generation cephalosporin or gentamicin, largely driven by intrinsically cephalosporin-resistant organisms. We did not observe any increase in MRSA colonisation over time, suggesting the absence of a major problem with infection control. However, we observed a gradual rise in colonising cephalosporin-resistant Gram-negative organisms despite apparently responsible use of antibiotics, with virtually no use of broad-spectrum antibiotics such as meropenem and third-generation cephalosporins. The relationship between antimicrobial use and drug resistance is complex. Possible factors involved in the observed pattern of antibiotic resistance include pathogen-drug interactions, pathogen-host interactions, pathogen mutation rates and transmission rate of pathogens to babies from mother, other babies or the environment.15 The increase may in part, for example, be due to increasing travel by families with overseas acquisition of resistant organisms.26
A key strength of this study is the long duration of prospective data collection using a consistent definition of sepsis, coding by one researcher and clearly defined indications for continuing or ceasing antibiotic therapy. Furthermore, the antibiotics used for empiric treatment of suspected LOS (vancomycin and gentamicin) remained the same for the 25-year duration. There are, however, some notable limitations to the study. First, the data were collected from a single centre and it is not certain whether the findings would apply generally. Second, the current study is based on observational data only and a limited number of predictors were collected. Nevertheless, it provides evidence to support a policy of stopping antibiotics after 2–3 days under specified criteria. Such a policy could be investigated in a randomised study in which infants with negative cultures would have their serum CRP measured and antibiotics would be stopped if the CRP was normal. If raised, the infants would be randomised to stop antibiotics immediately or to continue antibiotics until CRP normalised, as is common practice in some neonatal units. The numbers required for this study are likely to be large but may be achieved with a multicentre study.
Finally, it is not known if our data would be applicable in a low/middle-income country setting, where it is frequently argued that the population may be sicker and it is not safe to stop antibiotics despite negative cultures because the culture results may be unreliable.
Our study demonstrates that stopping antibiotics after 2–3 days was safe for babies who are clinically well or stable with negative systemic cultures over a prolonged period. Despite responsible antibiotic use, however, and decreased rates of late-onset infection, we witnessed a steady increase in colonisation with antibiotic-resistant Gram-negative bacilli. This is an issue of public health concern.
Acknowledgments
The authors thank Dr Tarun Singh and Dr Bradley de Vries for assistance in providing data by birth weight.
References
Footnotes
Contributors DCcollected, collated and analysed the data, performed the initial analyses and drafted the initial manuscript. EHBperformed all the statistical analyses. AGconceived the study with DI. DIconceived the study and collected the data over 25 years. All authors contributed to and approved the final manuscript as submitted.
Competing interests None declared.
Ethics approval Royal Alexandra Hospital for Children ethics committee (approval number 93060).
Provenance and peer review Not commissioned; externally peer reviewed.