Article Text

Abstract
Objectives Identify determinants of neurodevelopmental outcome in preterm children.
Methods Prospective national cohort study of children born between 2009 and 2011 at <29 weeks gestational age, admitted to one of 28 Canadian neonatal intensive care units and assessed at a Canadian Neonatal Follow-up Network site at 21 months corrected age for cerebral palsy (CP), visual, hearing and developmental status using the Bayley Scales of Infant and Toddler Development-Third Edition (Bayley-III). Stepwise regression analyses evaluated the effect of (1) prenatal and neonatal characteristics, (2) admission severity of illness, (3) major neonatal morbidities, (4) neonatal neuroimaging abnormalities, and (5) site on neurodevelopmental impairment (NDI) (Bayley-III score < 85, any CP, visual or hearing impairment), significant neurodevelopmental impairment (sNDI) (Bayley-III < 70, severe CP, blind or hearing aided and sNDI or death.
Results Of the 3700 admissions without severe congenital anomalies, 84% survived to discharge and of the 2340 admissions, 46% (IQR site variation 38%–51%) had a NDI, 17% (11%–23%) had a sNDI, 6.4% (3.1%–8.6%) had CP, 2.6% (2.5%–13.3%) had hearing aids or cochlear implants and 1.6% (0%–3.1%) had a bilateral visual impairment. Bayley-III composite scores of <70 for cognitive, language and motor domains were 3.3%, 10.9% and 6.7%, respectively. Gestational age, sex, outborn, illness severity, bronchopulmonary dysplasia, necrotising enterocolitis, late-onset sepsis, retinopathy of prematurity, abnormal neuroimaging and site were significantly associated with NDI or sNDI. Site variation ORs for NDI, sNDI and sNDI/death ranged from 0.3–4.3, 0.04–3.5 and 0.12–1.96, respectively.
Conclusion Most preterm survivors are free of sNDI. The risk factors, including site, associated with neurodevelopmental status suggest opportunities for improving outcomes.
- prematurity
- impairments
- Outcomes research
Statistics from Altmetric.com
What is already known on this topic?
Despite improving survival rates, cognitive, motor and sensory impairments are common in the preterm population.
There are significant site variations in neurodevelopmental impairment rates.
What this study adds?
In Canada, 83.5% of survivors born at <29 weeks gestation have no significant neurodevelopmental impairments (non-ambulatory cerebral palsy, Bayley Scales of Infant and Toddler Development-Third Edition (Bayley-III) cognitive, language or motor score <70, bilateral visual impairment, hearing aids) though less severe impairments are common (46%) at 21 months corrected age.
Site variations and modifiable characteristics identified provide opportunities for improvement.
Introduction
The goal of neonatal intensive care for the baby born preterm is long-term survival with optimal health, development and well-being. Whereas survival has improved dramatically with advances in neonatal care, most studies show little improvement in longer term neurodevelopmental outcomes including cognitive, motor, visual or hearing impairments.1 ,2 Demonstrating evidence of between-site variations3 ,4 is important because comparative effectiveness studies have used site variation and modifiable risk factors to target improvement.5–7 Identifying determinants of long-term neurodevelopmental outcomes and site variation in the preterm population is therefore important.
The objective of this study was to investigate determinants of neurodevelopmental impairment (NDI), significant NDI (sNDI) and ‘sNDI or death’ rates among very preterm infants born at <29 weeks gestational age (GA) in Canada and assessed at 18–21 months corrected age (CA). Instead of the more negative term ‘severe’ to describe degree of NDI, the expression ‘significant’ NDI is used. We hypothesised that there would be significant variations in neurodevelopmental outcome rates between Canadian neonatal intensive care units (NICUs), even after adjustment for confounding variables.
Patients and methods
Study population
Eligible preterm infants were born between 1 April 2009 and 30 September 2011 at <29 weeks GA and were admitted to one or more of the 28 NICUs contributing data to the Canadian Neonatal Network (CNN) and the Canadian Institutes of Health Research (CIHR) Team in the Maternal-Infant Care (MiCare) study.8 This population represented approximately 95% of Canadian NICU admissions during this time period. As part of the MiCare study, the Canadian Neonatal Follow-Up Network (CNFUN)9 developed a national standardised assessment and data collection database for infants at 18–21 months CA, with the ability to link data to the CNN database. Infants were excluded if they were moribund on admission or had life-threatening congenital anomalies. Site research ethics boards approved the MiCare study at all participating sites.
Data collection
Patient data were collected by the CNN, as previously described,10 and a unique identifier, shared between CNN and CNFUN data abstractors, was used to link CNN and CNFUN data. The NICU to which a newborn was first admitted was defined as the CNN site. Eligible patients were recruited and scheduled for an assessment at one of the 26 CNFUN follow-up programmes (including all follow-up programmes in Canada) at a target age of 18–21 months CA, with subsequent tracking of recruits by the CNFUN coordinating site, as outlined in the CNFUN manual.9 Children who were difficult to schedule or lost to follow-up and assessed later were also included.
Neonatal data definitions
Variables abstracted from the CNN database were categorised as follows: (1) infant and pregnancy characteristics, (2) illness severity, (3) major neonatal morbidities, (4) brain injury and (5) NICU site. Subject characteristics included the best estimate of GA10; multiple birth; small for GA (SGA), defined as birth weight (BW) below the 10th percentile11; and Apgar score at 5 min of age. Pregnancy characteristics assessed were chorioamnionitis, defined as maternal fever ≥38.4°C within 24 hours of birth, uterine tenderness, maternal leucocytosis >15 000/mm3 or inflammation on placental pathology; obstetrical report of pre-existing or gestational and pregnancy-induced hypertension; obstetrical report of gestational diabetes mellitus; receipt of one or more doses of antenatal steroids; prolonged rupture of membranes (≥24 hours) and mode of delivery (vaginal or caesarean section). Score for Neonatal Acute Physiology (SNAP-II), a validated measure of severity of illness, was collected during the first 12 hours of admission; higher scores predict mortality in extremely preterm infants.12 Major neonatal morbidities evaluated were bronchopulmonary dysplasia (BPD), defined as any supplemental oxygen and/or respiratory support at 36 weeks corrected GA or at the time of transfer to a lower level of care; sepsis, defined as a positive bacterial, viral or fungal culture in blood or cerebrospinal fluid with early onset occurring in the first 2 days after birth and late-onset sepsis thereafter; stage 2 or 3 necrotising enterocolitis (NEC), defined according to Bell's criteria13; severe retinopathy of prematurity (ROP), defined as stage 3 or greater14 in either eye or treatment with laser or injections of anti-vascular endothelial growth factor and severe brain injury, defined as any grade 3 or 4 intraventricular haemorrhage,15 ventricular dilatation ≥10 mm, intraparenchymal haemorrhage or periventricular leukomalacia.16
Study participant assessments
The assessment at 18–21 months CA included a standardised history, physical exam, neurological exam and the Bayley Scales of Infant and Toddler Development-Third Edition (Bayley-III).17 Children were usually seen in a CNFUN site by experienced clinicians; however, if travel to a CNFUN site was not possible (<6% of cases), community healthcare professional assessments were used. A standardised history included sociodemographic information about the child's family and primary caregivers, medical history and current health status, including medications and health resource utilisation. To encompass non-traditional family composition, parents were described as caregivers and their characteristics (ie, sex, biological or other relationship to the child, education, employment status) were recorded. As hearing assessment is a standard of care for the study population, hearing testing results and the need for hearing aids or cochlear implants was obtained from patient history. Vision history including ophthalmology follow-up for ROP and current visual status was documented. If vision history was unknown, a screening visual assessment was performed. A small, scarred eye, sustained sensory nystagmus or lack of response to a 1 cm object on a white background from a distance of 30 cm was deemed as a visual impairment. A diagnosis of cerebral palsy (CP) was assigned as definitive when all criteria were met18 and assigned as suspect when only partially met.9 The Gross Motor Function Classification System (GMFCS) was used to classify the degree of functional impairment in children with CP.19 The presence or absence of other clinically significant neurological abnormalities affecting a child's development was determined. Trained examiners, certified using an online training course specific to this study population (Bayley-III, NCS Pearson), assessed cognitive, language and motor development using the Bayley-III.17 Using CA, raw, scaled and composite scores for cognitive, language and motor domains were calculated. In cases where the child could not be tested, the reason, including severe developmental delay, was recorded and the Bayley-III Adaptive Behavior questionnaires were administered. NDI and sNDI definitions (table 1) were adapted from the literature.20 Since Bayley-III composite scores tend to underestimate developmental delay,21 scores <70 were classified as a sNDI and Bayley-III composite scores <85 were classified as a NDI.
Definitions of NDI
Data analyses
Population characteristics and adverse outcomes were descriptively analysed. Results are not displayed for outcomes with less than five subjects. χ2 and non-parametric tests were used to compare study participants with those lost to follow-up. Outcome rates were calculated for each week of GA and for all CNN sites. Cochran-Armitage test was used for trend analyses. Forward stepwise logistic regression analyses were performed for NDI, sNDI and ‘sNDI or death’ with inclusion of variables with a p value <0.1 for steps 1–4 and p value <0.05 for step 5. In step 1, patient and pregnancy characteristics were included. Subsequently, severity of illness (step 2), major neonatal morbidity (step 3), brain injury (step 4) and CNN sites with at least 10 cases of NDI, sNDI or ‘sNDI or death’ (step 5) were added to the model. A p value of <0.05 was deemed significant.
Results
Population characteristics
During the study period, 3993 infants were admitted to a participating NICU (see online supplementary figure 1) and 293 were excluded because they were moribund (n=65) or had life-threatening congenital anomalies (n=228). The neonatal survival rate was 84% (3108/3700). Among 3700 eligible infants, outcome data were available for 2954 (80%), including 2340 assessed, 592 NICU deaths and 22 post-NICU deaths. Reasons for children (n=470) not seen at 18–21 months were as follows: (1) parents did not consent (26.2%), (2) study participants could not be contacted (24.5%), (3) subjects were scheduled but did not attend (17.0%) and (4) unknown reason for non-participation (32.3%). This very preterm cohort had a median GA of 27 weeks and BW of 920 g. Compared with children lost to follow-up, the participant cohort was of lower GA, lower BW, more likely to have received antenatal steroids, had higher early severity of illness and suffered from more complications of prematurity (see online supplementary table 1). In the Canadian multicultural context, approximately two-thirds of caregivers were born in Canada, 54% described themselves as Caucasian, 76% had English or French as the primary language and most caregivers had some education beyond high school (see online supplementary table 2).
Supplementary table
Comparison of neonates assessed and those lost to follow-up.
Supplementary table
Characteristics of neonates and caregivers who had neurodevelopmental assessment (n=2340).
Neurodevelopmental outcomes
Of the 2340 survivors assessed at a median age of 21.7 months, 16.5% met the criteria for sNDI and 46.0% met the criteria for NDI (table 2), respectively. Definitive CP was present in 6.4% of the population. The severity of CP as assessed by GMFCS was less than level 2 (walking independently) in 35.6%, was level 2 in 15.7%, was level 3 in 14.4%, was level 4 in 9.6% and was level 5 (no head control) in 10.3%. Significant sensory impairment was infrequent (2.6% of children had a hearing aid or cochlear implant and 1.6% had bilateral visual impairment), as were Bayley-III composite scores <70. However, Bayley-III scores <85 were common: language 35%, motor 22% and cognitive 15%. Outcomes were inversely correlated with GA (p<0.01) (figure 1).
Outcomes at 21 months corrected age by GA
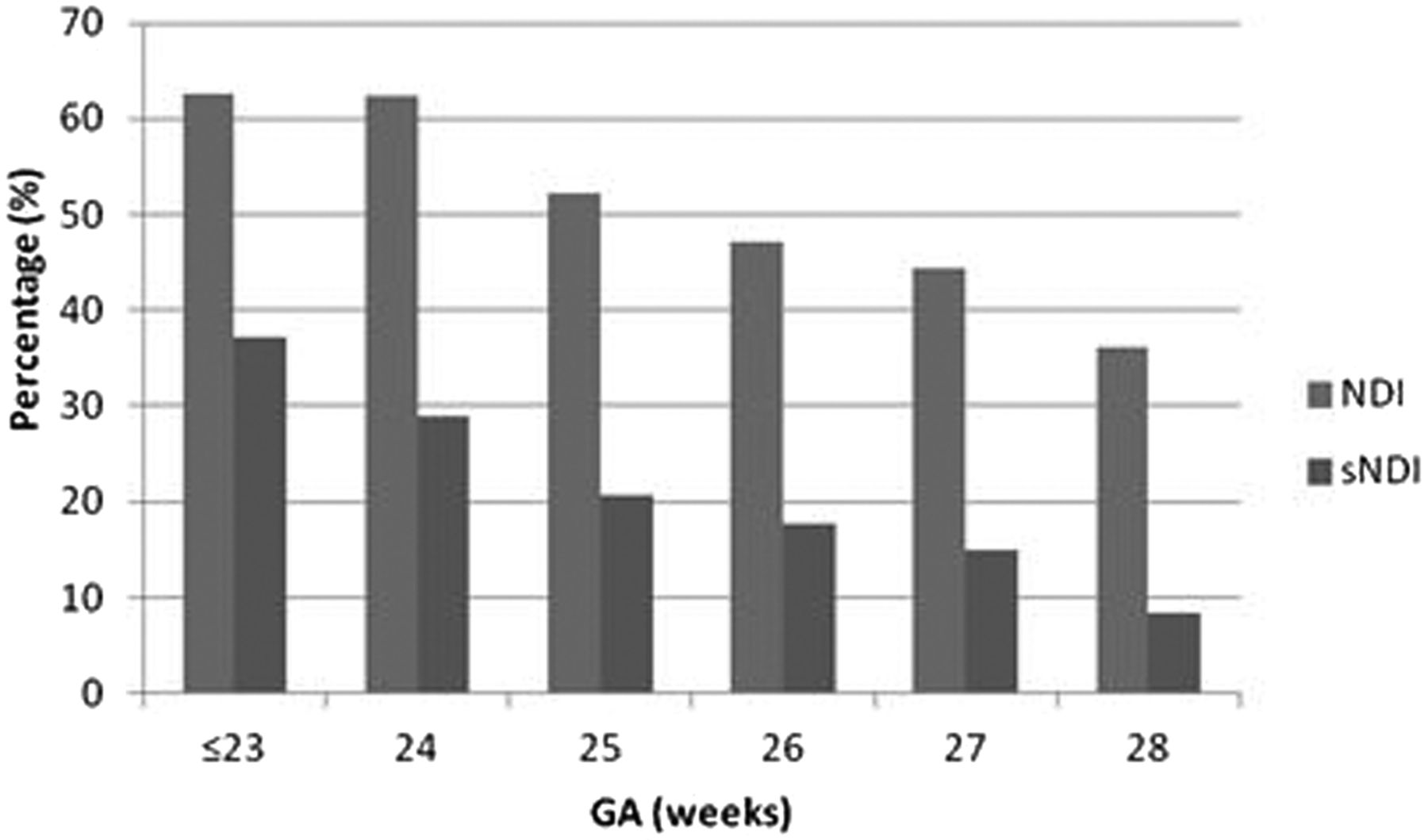
Bar graph showing the incidence of neurodevelopmental impairment (NDI) and significant NDI (sNDI) by gestational age (GA). The percentage of children with NDI and sNDI for each completed week GA is shown.
Risk factors for adverse outcome
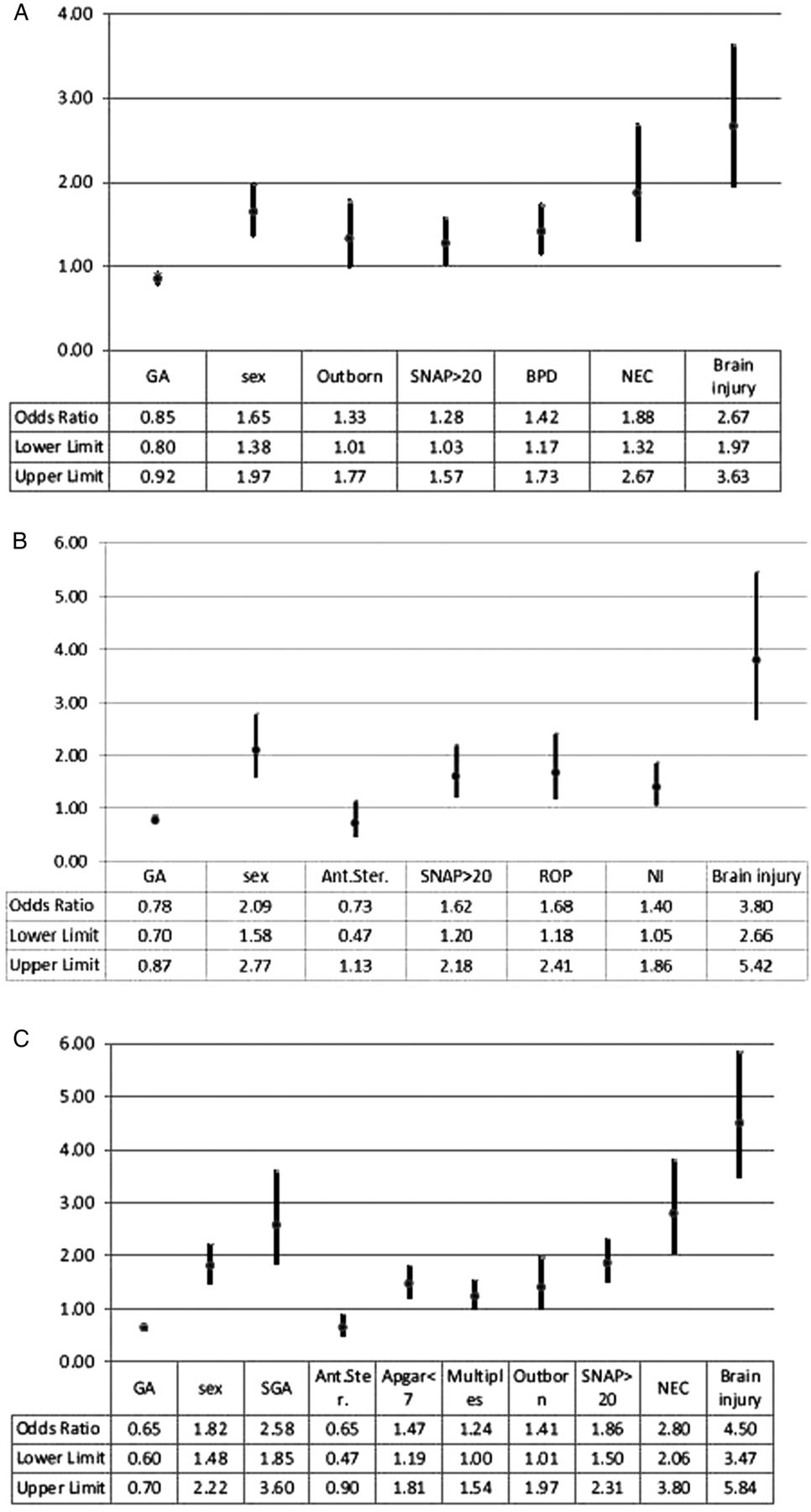
Results of the final stepwise regression analyses for NDI, sNDI and ‘sNDI or death’ are shown graphically in figures 2 and 3 (see online supplementary tables 3–5). In step 1, GA and sex were strongly associated with all three outcomes as was a high SNAP-II score >20 in step 2 and severe brain injury in step 4. The major neonatal morbidities (step 3), which were statistically significant, varied: BPD and NEC were associated with NDI, ROP and late-onset sepsis with sNDI and NEC with ‘sNDI or death’. Outborn delivery was weakly associated with NDI and ‘sNDI or death’. Non-receipt of antenatal steroids, 5 min Apgar score <7, being a multiple, and SGA were statistically associated with the composite outcome ‘sNDI or death’. The predictive ability improved with each additional step. The area under the curve for the final models was 0.683, 0.769 and 0.815 for NDI, sNDI and ‘sNDI or death’, respectively.
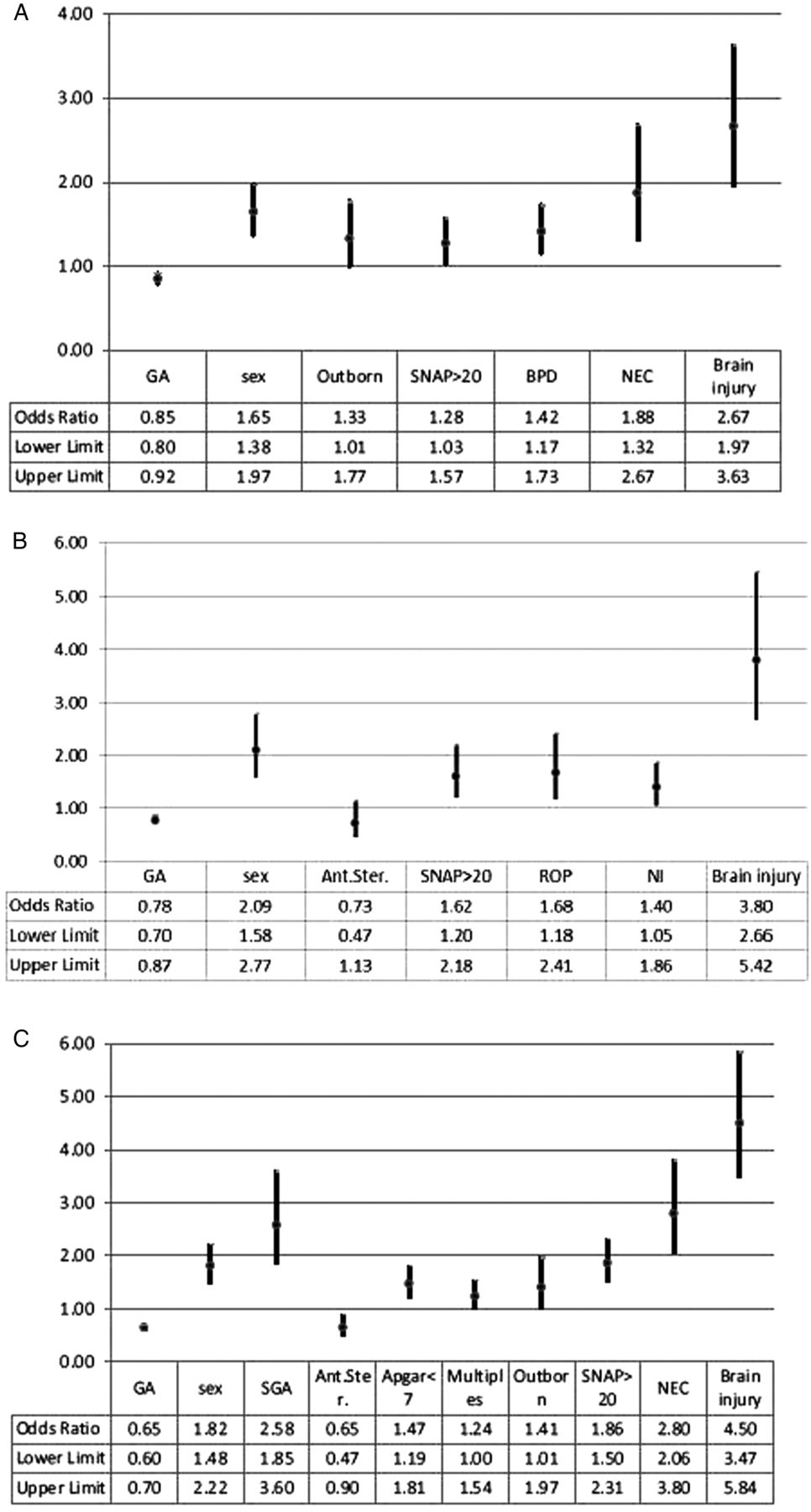
Results of stepwise regression analyses are shown. Analyses were conducted to examine the association between (A) neurodevelopmental impairment (NDI), (B) significant NDI (sNDI) and (C) ‘sNDI or death’ and infant and pregnancy characteristics, illness severity (SNAP >20), major neonatal morbidities and brain injury. Ant. Ster., antenatal steroids; BPD, bronchopulmonary dysplasia; GA, gestational age; NEC, necrotising enterocolitis; NI, nosocomial infection; ROP, severe retinopathy of prematurity; SGA, small for gestational age; SNAP, Score for Neonatal Acute Physiology.

{kind=link}
{kind=link}
{kind=link}
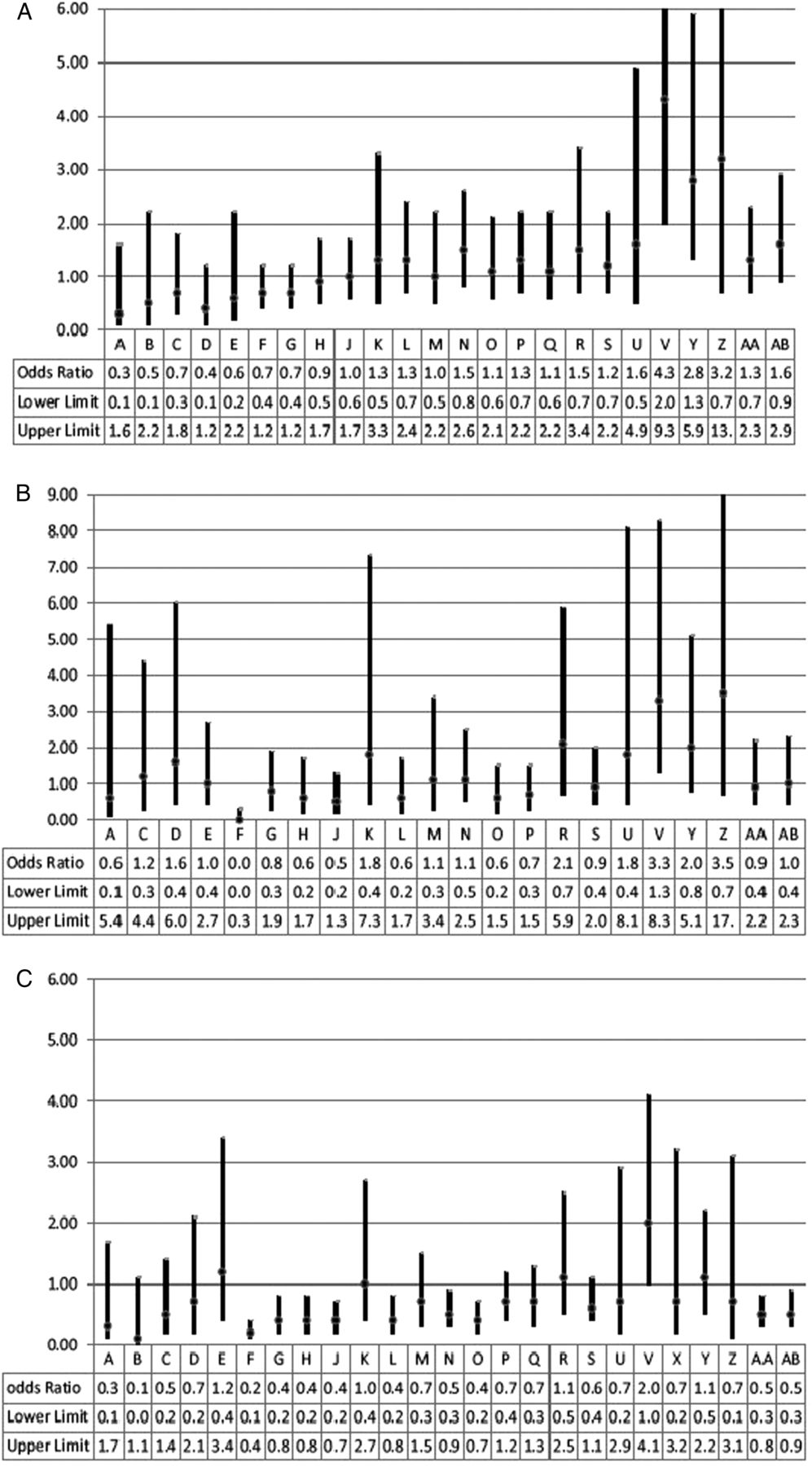
Results of the regression analyses—site variation—are shown. Analyses examined the association between (A) neurodevelopmental impairment (NDI), (B) significant NDI (sNDI) and (C) ‘sNDI or death’ and neonatal intensive care unit.
Supplementary table
Site variation
The variations in unadjusted NICU incidence rates for all outcomes are shown in table 3. After adjustment for known risk factors, some sites showed statistically significant variations in NDI, sNDI or ‘sNDI or death’ (figure 3) with adjusted ORs ranging from 0.04 (95% CI 0.01 to 0.32) to 3.51 (0.69 to 17.83) for sNDI and from 0.32 (0.06 to 1.63) to 4.27 (1.96 to 9.33) for NDI.
Proportion of children with adverse developmental outcomes by centre
Discussion
In Canada, most surviving preterm infants (83.5%) born at <29 weeks GA are free of sNDI at 21 months CA. Though 46% of patients met our definition for NDI, the long-term clinical significance is less certain.22 Our sNDI and NDI rates of 16.5% and 46%, respectively, are consistent with most other networks and national studies. In the Swedish EXPRESS cohort23 born at <27 weeks GA, the severe or moderate impairment rate was 20% and the mild, moderate or severe impairment rate was 44.5%. The French EPIPAGE group reported that children aged 5 years who were born at 24–28 weeks gestation had a moderate or severe disability rate of 22% and any disability rate of 48%.24 The Victorian Infant Collaborative Study Group25 reported quality-adjusted outcomes relative to term-born controls, rather than test norms, for children born in 2005 at <28 weeks gestation: 80% had either a mild or no disability and 17% and 4% had a moderate or severe disability (<−2 SD), respectively. In the National Institute of Child Health and Human Development Research Network, NDI or death decreased with increasing GA up to 27 weeks GA.26 Unfortunately, although the above findings are relevant to our study, differences in cohort and impairment definitions make it challenging to compare outcomes between countries.
Since our results will be of interest for counselling families, it is important to understand the limitations of the terms ‘sNDI’ and ‘NDI’. Families' perceptions of ‘severe’ and ‘clinically significant’ disabilities will vary. There is no valid measure of quality of life at 18 months CA27 and the predictive ability of the Bayley-III is limited.22 ,28 Though based on the American norms, 15% of children would be expected to score <85 on the Bayley-III composite scores,17 but this may not apply to the Canadian population. In Australia, the mean (SD) of healthy controls was 108.9 (14.3), 108.2 (14.8) and 118.4 (16.7) for the Bayley-III Cognitive, Language and Motor composite scores, respectively, and only approximately 5% of controls scored <85.21 We used composite scores and definitions similar to those in the literature but did not evaluate whether these are meaningful definitions for parents and healthcare providers. The use of composite scores is very helpful in the statistical analyses of neurodevelopmental outcomes but composite scores hide the variance within domains.1 Further studies are therefore needed to identify the most meaningful outcome definitions.
Systematic audit, benchmarking and analysis of risk factors are promising strategies to reduce adverse outcome rates. Our results highlight the importance of severe brain injury, as well as BPD, NEC and sepsis as risk factors for adverse outcomes. A reduction in the latter three was associated with a recently reported fall in extremely preterm NDI rates.29 The CNN ‘Evidence Based Practice to Improve Quality’ intervention significantly improved short-term morbidities such as BPD,5 ,6 sepsis,5–7 severe ROP7 and NEC.7 Site variation is essential for this intervention where sites with better outcomes facilitate improvement in those doing less well.
We acknowledge several limitations. First, we were unable to link 9% of subjects in the CNN (276/3108) with the CNFUN database and had an attrition rate of 16.7% (470/2810) among survivors. Children included in our analyses were of lower GA and had higher severity of illness than those lost to follow-up; therefore, sNDI and NDI rates may have been overestimated. Second, although we report on outcomes at 18–21 months CA, which aligns with CNFUN clinical practices, the lower predictive ability of the Bayley-III at 18 months CA compared with older ages should be taken into account.22 Also, even though most children with CP can be diagnosed at 18–24 months,30 CP registries consider 5 years to be more reliable.31 Third, CNN data were abstracted from medical records and definitions such as intracranial ventricular dilatation were not independently verified. In CNFUN, hearing and vision status were determined by history and clinically available information rather than direct assessment. Finally, as the focus of our study included comparisons between sites, our study did not include a healthy term-born comparison group. These compromises were necessary to achieve the benefits of our large, current ongoing national database.
Unlike survival and many short-term outcomes, the evaluation of long-term outcomes is challenging due to referral biases, variations in outcome definitions and how they are evaluated, attrition bias and small sample size.2 The CNFUN has successfully addressed many of these challenges despite having the second-largest landmass in the world and demonstrated the feasibility of a national neonatal follow-up data for children born very preterm.
In conclusion, the linked CNN and CNFUN databases demonstrated that 83.5% of survivors born at <29 weeks GA are free of sNDI, though a less severe impairment or developmental delay that may require intervention affects almost 50% of children. An improved understanding of the outcome variability between units is urgently required to target interventions with better efficiency and to improve long-term outcomes for future very preterm births.
Acknowledgments
The authors would also like to acknowledge Natasha Musrap, PhD, from the Maternal-Infant Care Research Centre for editorial assistance in the preparation of this manuscript.
References
Footnotes
Collaborators Canadian Neonatal Network Investigators: Prakesh S Shah, MD, MSc (director, Canadian Neonatal Network and site investigator), Mount Sinai Hospital, Toronto, Ontario; Adele Harrison, MD, MBChB, Victoria General Hospital, Victoria, British Columbia; Anne Synnes, MDCM, MHSC, and Joseph Ting, MD, British Columbia Women's Hospital, Vancouver, British Columbia; Wendy Yee, MD, Foothills Medical Centre, Calgary, Alberta; Khalid Aziz, MBBS, MA, MEd, and Jennifer Toye, MD, Royal Alexandra Hospital and University of Alberta Hospital, Edmonton, Alberta; Zarin Kalapesi, MD, Regina General Hospital, Regina, Saskatchewan; Koravangattu Sankaran, MD, MBBS, and Sibasis Daspal, MD, Royal University Hospital, Saskatoon, Saskatchewan; Mary Seshia, MBChB, Winnipeg Health Sciences Centre, Winnipeg, Manitoba; Ruben Alvaro, MD, St Boniface General Hospital, Winnipeg, Manitoba; Sandesh Shivananda, MBBS, MD, DM, Hamilton Health Sciences Centre, Hamilton, Ontario; Orlando Da Silva, MD, MSc, London Health Sciences Centre, London, Ontario; Chukwuma Nwaesei, MD, Windsor Regional Hospital, Windsor, Ontario; Kyong-Soon Lee, MD, MSc, Hospital for Sick Children, Toronto, Ontario; Michael Dunn, MD, Sunnybrook Health Sciences Centre, Toronto, Ontario; Nicole Rouvinez-Bouali, MD, Children's Hospital of Eastern Ontario and Ottawa General Hospital, Ottawa, Ontario; Kimberly Dow, MD, Kingston General Hospital, Kingston, Ontario; Ermelinda Pelausa, MD and Lajos Kovacs MD, Jewish General Hospital, Montréal, Québec; Keith Barrington, MBChB, Hôpital Sainte-Justine, Montréal, Québec; Christine Drolet, MD, and Bruno Piedboeuf, MD, Centre Hospitalier Universitaire de Québec, Sainte Foy Québec; S Patricia Riley MD and Martine Claveau, RN, Montreal Children's Hospital and Daniel Faucher MD, Royal Victoria Hospital (latter two now merged as McGill University Health Centre), Montréal, Québec; Valerie Bertelle, MD, and Edith Masse, MD, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Québec; Roderick Canning, MD, Moncton Hospital, Moncton, New Brunswick; Hala Makary, MD, Dr Everett Chalmers Hospital, Fredericton, New Brunswick; Cecil Ojah, MBBS, and Luis Monterrosa, MD, Saint John Regional Hospital, Saint John, New Brunswick; Wayne Andrews MD and Akhil Deshpandey, MD, MBBS, Janeway Children's Health and Rehabilitation Centre, St John's, Newfoundland; Doug McMillan MD and Jehier Afifi, MB BCh, MSc, IWK Health Centre, Halifax, Nova Scotia; Shoo K Lee, MBBS, PhD (chairman, Canadian Neonatal Network), Mount Sinai Hospital, Toronto, Ontario. Canadian Neonatal Follow-Up Network Investigators: Thevanisha Pillay, MD, Victoria General Hospital, Victoria, British Columbia; Anne Synnes, MDCM, MHSC, British Columbia Women's Hospital, Vancouver, British Columbia; Reg Sauvé, MD, MPh, Alberta's Children's Hospital, Foothills Medical Centre, Calgary, Alberta; Amber Reichert, MD, Glenrose Rehabilitation Hospital, Edmonton, Alberta; Jaya Bodani, MD, Regina General Hospital, Regina, Saskatchewan; Koravangattu Sankaran, MD, Royal University Hospital, Saskatoon, Saskatchewan; Diane Moddemann, MD, Winnipeg Health Sciences Centre, St Boniface General Hospital, Winnipeg, Manitoba; Chukwuma Nwaesei, MD, Windsor Regional Hospital, Windsor, Ontario; Thierry Daboval, MD, Children's Hospital of Eastern Ontario, Ottawa, Ontario; Kimberly Dow, Kingston General Hospital, Kingston, Ontario; David Lee, MD, Children's Hospital London Health Sciences Centre, London, Ontario; Linh Ly, MD, Hospital for Sick Children, Toronto, Ontario; Edmond Kelly, MD, Mount Sinai Hospital, Toronto, Ontario; Salhab el Helou, MD, Hamilton Health Sciences Centre, Hamilton, Ontario; Paige Church, MD, Sunnybrook Health Sciences Centre, Toronto, Ontario; Ermelinda Pelausa, MD, Jewish General Hospital, Montréal, Québec; S Patricia Riley, MD, Montréal Children's Hospital, Royal Victoria Hospital, Montréal, Québec; Francine Levebvre, Centre Hospitalier Universitaire Sainte-Justine, Montréal, Québec; Charlotte Demers, Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke, Québec; Sylvie Bélanger, MD, Centre Hospitalier Universitaire de Québec, Québec City, Québec; Roderick Canning, MD, Moncton Hospital, Moncton, New Brunswick; Luis Monterrosa, MD, Saint John Regional Hospital, Saint John, New Brunswick; Hala Makary, MD, Dr Everett Chalmers Hospital, Fredericton, New Brunswick; Michael Vincer, MD, IWK Health Centre, Halifax, Nova Scotia; Phil Murphy, Charles Janeway Children's Health and Rehabilitation Centre, St John's, Newfoundland.
Contributors AS, the founding director of the Canadian Neonatal Follow-Up Network, conceptualised and implemented the study, wrote the initial manuscript and approved the final manuscript as submitted. JY performed the statistical analyses, reviewed and approved the final manuscript as submitted. TML, DM, PC, DL, MV, MB, AM and DC are Canadian Neonatal Follow-up Network steering committee members who contributed to the implementation of this study, reviewed and revised the study protocol and the final manuscript and approved the final manuscript as submitted. RS and SS are Canadian Neonatal Follow-up Network founding steering committee members who obtained funding, contributed to the implementation of this study, reviewed and revised the final manuscript and approved the final manuscript as submitted. PS, the director of the Canadian Neonatal Network, reviewed and revised the study protocol and the final manuscript, supervised the data analyses and approved the final manuscript as submitted. SKL, the founding director of the Canadian Neonatal Network and the Maternal-Infant Care Network, is the principal investigator on the Canadian Institutes of Health Research (CIHR) Team in Maternal-Infant Care which funded the Canadian Neonatal Follow-Up Network and reviewed and revised the final manuscript and approved the final manuscript as submitted. All authors take responsibility for all aspects of the work presented in this paper, including the accuracy and integrity of the data analyses.
Funding This work was supported by the CIHR through a grant to the CIHR Team in Maternal-Infant Care (CTP 87518). The study coordinating centre, the Maternal-Infant Care Research Centre, is supported by a programme funding from the Ontario Ministry of Health and Long-Term Care. In addition, participating sites contributed additional funding for patient outcome assessments.
Competing interests None declared.
Ethics approval University of British Columbia Children's and Women's Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The privacy impact assessment for the Maternal-Infant Care Research Centre, Mount Sinai Hospital, Toronto, Ontario, Canada, has not approved any data to leave the coordinating site.