Article Text

Abstract
Background Infant enterostomies are used to manage various neonatal surgical conditions where it is not suitable or safe to form a primary anastomosis. Complications are common and there is no consensus regarding optimal timing of enterostomy reversal. Stoma reversal is thought to allow patients to thrive; however, this has not been demonstrated robustly.
Aim The study aimed to identify risk factors for enterostomy-related complications and to determine the relationship between enterostomy complications, enterostomy reversal and weight gain in infants with enterostomies.
Methods A retrospective case note review of 58 infants who underwent enterostomy formation and reversal during a 6-year period was undertaken; demographic data, diagnosis, enterostomy complications and serial weights were noted. Standardised growth charts were used to calculate z scores.
Results Enterostomy complications were documented in 24 infants (41%). Infants of low birth weight and low gestational birth age were significantly more likely to have an enterostomy-related complication (1110 vs 2125 g, 28.5 vs 35 weeks, respectively); they were more likely to have longer inpatient stays and remain dependent on parenteral nutrition prior to closure (median 92.5 vs 52 days, 40% vs 16%, respectively). Irrespective of diagnosis, gestation and presence of an enterostomy complication, the mean z score prior to enterostomy closure was −0.747 vs +0.892 following closure.
Conclusions Around 40% of infants with an enterostomy will have an enterostomy-related complication. Whatever their weight, gestation or underlying pathology, most infants thrive after enterostomy closure and this should be considered when planning the optimal timing for this procedure.
- Neonatology
- Paediatric Surgery
- Growth
Statistics from Altmetric.com
What is already known on this topic?
Temporary enterostomy formation is used to manage a variety of neonatal surgical conditions, including necrotising enterocolitis and intestinal atresia.
Enterostomy management in small babies can be challenging; complications are well described and establishing weight gain may be difficult.
There is no consensus regarding the best timing of enterostomy reversal, and this is usually a multifactorial decision.
What this study adds?
We found a significant improvement in z score following enterostomy reversal regardless of gestational age at birth, underlying diagnosis or presence of enterostomy-related complications.
The data supports consideration of early restoration of intestinal continuity in neonates with growth failure; however, further work is needed to assess the risk of early enterostomy reversal.
Introduction
Temporary enterostomy (stoma) formation is used to manage a variety of neonatal surgical conditions, including necrotising enterocolitis (NEC) and intestinal atresia. While bowel resection and primary anastomosis with avoidance of an enterostomy is preferable when clinically appropriate, there are many situations where it is considered safer to create an enterostomy.1 ,2 Enterostomy management in small babies can be challenging; complications are well described and establishing weight gain may be difficult.3 ,4 Although the evidence is limited, lower weight and younger age at time of enterostomy reversal have been associated with complications, such as stoma prolapse and wound dehiscence, yet high-output enterostomies are associated with poor weight gain and early closure may be preferable.4–6
Depending on the primary pathology, postsurgical recovery often involves administration of parenteral nutrition (PN) followed by graded introduction of enteral feeds with the aim of weaning from PN. Recycling of enterostomy output down the distal bowel enterostomy (mucous fistula) is commonly employed to stimulate mucosal growth and prevent distal bowel atrophy prior to enterostomy reversal.7 There is no consensus regarding the best timing of enterostomy reversal: this is usually a multifactorial decision, taking into account factors such as patient age, diagnosis, comorbidities, duration with enterostomy, ability to establish enteral feeding and weight gain. Poor growth is associated with paediatric enterostomies and it is accepted that in the majority of patients, enterostomy reversal allows weight gain and growth.8 However, to the best of our knowledge, no studies show this growth in terms of weight gain on standardised growth charts.
Aim
The aim of this study was to identify risk factors for development of enterostomy-related complications and to determine the relationship between enterostomy complications, enterostomy reversal and weight gain in infants with enterostomies.
Methods
Study design
This was a retrospective case note review with audit department approval at both the paediatric surgery centre (audit number 3642) and the nearby tertiary neonatal unit (audit number 2014/031). Infants with a code for ileostomy or jejunostomy reversal at the paediatric surgical centre during a 6-year period from January 2008 to December 2013 were included in the study. Children over 20 weeks of age at the time of first enterostomy formation were excluded. Data were analysed according to two main criteria: first according to the presence or absence of enterostomy-related complications, and second, according to gestational age at birth, with a cut-off of 36 weeks to try and separate the two main pathologies (NEC and intestinal atresia). Data were collated from operation notes, inpatient medical and nursing notes, weight charts and histopathology reports.
Patient weight analysis
Where the birth weight and more than two weight recordings both pre-enterostomy and post-enterostomy reversal were available (33 of 58 patients), LMSgrowth software (Royal College of Paediatrics and Child Health, UK) was used to calculate weight-for-age z scores using British 1990 (UK 90) growth reference charts. The weight-for-age z score (or SD score) is a measure of the SD of weight from the median value of a reference population matched for age and sex. Z scores, therefore, can be used to discriminate between a child who is gaining weight at a slower rate than the reference population (therefore faltering on a standardised growth chart) and a child who is gaining weight faster than a reference population and hence thriving in terms of weight.9 The difference between pre-enterostomy and post-enterostomy reversal scores was calculated to determine weight loss (a negative z score) or gain (a positive z score).
Statistical analysis
GraphPad Prism 4.03 was used for the statistical analysis. Data are presented as median (range) unless otherwise stated. The Mann-Whitney U test was performed on continuous data and Fisher's exact test for categorical data. Outliers were identified and removed using Rosner's outlier test. A p value of <0.05 was considered statistically significant.
Results
Seventy children were eligible for the study; 58 of these had comprehensive case notes and formed the study population. In the 12 patients not included, eight were male, nine had a diagnosis of NEC (one meconium ileus, one milk curd obstruction and one ileal stricture), 11 had ileostomies, the median birth weight was 1265 g (range 830–1300 g) and the median gestation age at birth was 30 weeks (range 26–36 weeks). There was no significant difference between the demographics of the included and excluded groups. Demographics and diagnosis for the patients are shown in table 1.
Table showing associations with developing enterostomy-related complications
Comparison of patients with and without enterostomy-related complications
The overall incidence of enterostomy-related complications was 41%. The complications encountered were prolapse (8), proximal enterostomy retraction (4), parastomal hernia (3), superficial skin breakdown (2), distal stoma stenosis (2), wound dehiscence (2), stoma necrosis (1), omental prolapse (1) and enterostomy-related fistula (1). No child had more than one complication documented.
Low birth weight, young gestational age at birth, young conceptual age at enterostomy formation, low weight at enterostomy reversal, long inpatient stay, failure to be discharged home before reversal and longer duration of PN requirement were all associated with a higher chance of enterostomy-related complications (table 1). Diagnosis was not an underlying predictor of enterostomy-related complications.
Comparison of patients born before and after 36 weeks gestation
When the data were analysed according to gestational age at birth, 21 (55%) patients born at less than 36 weeks gestation experienced enterostomy-related complications versus 3 (15%) patients born at 36 weeks or more (p=0.005). The majority (71%) of those born at less than 36 weeks gestation had NEC while the majority (60%) of patients born after 36 weeks had intestinal atresia. Patients born before 36 weeks gestation had a enterostomy for 95 (42–218) days before reversal compared with patients born after 36 weeks who had the enterostomy for a median of 136 (55–272) days (p=0.033). All 20 patients born after 36 weeks gestation were discharged home before reversal, whereas only 58% of those born before this time were discharged before enterostomy reversal.
Reversing the enterostomy allows the infant to thrive
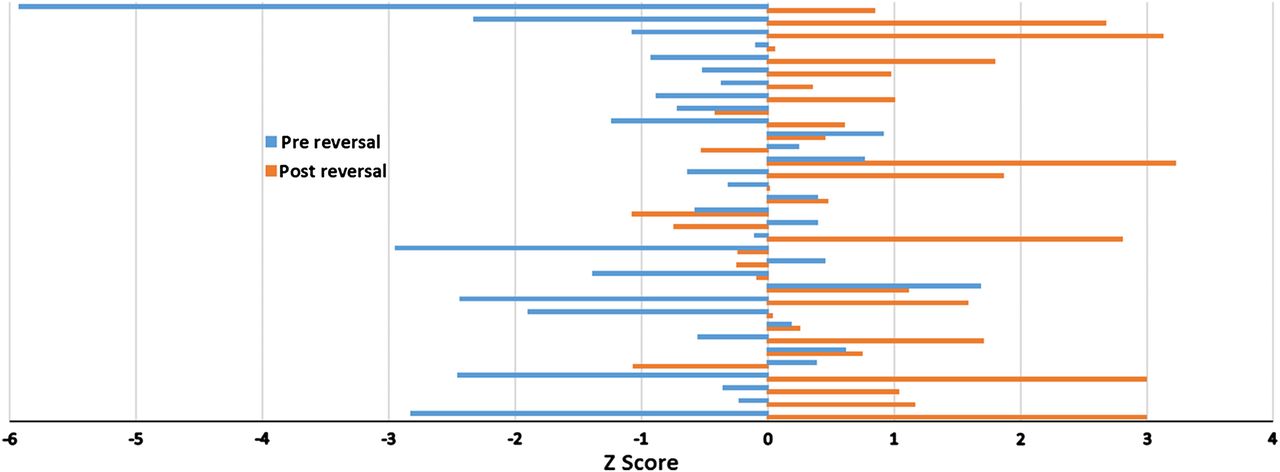
The individual z scores before and after reversal for all eligible patients (n=33) are represented in figure 1 and mean scores are given in table 2. Prereversal, 23 patients had a negative z score and 10 had a positive z score with a mean score of −0.747. Postreversal, eight patients had a negative z score and 25 had a positive z score with a mean score of 0.892. There is a statistically significant difference between the mean score prereversal and postreversal (p=0.001), suggesting that enterostomy reversal allows the patient to thrive. There is no significant difference between the mean z scores before and after reversal for those who experienced complications versus those who did not. This suggests that growth failure does not predispose to developing complications. Further analysis of the z score data finds no significant difference in mean z scores between patients born before 36 weeks gestation versus those born after, nor for those with NEC versus those with other diagnoses.
Table showing mean z scores pre-enterostomy and post-enterostomy reversal
{kind=link}
Graph to show weight gain pre-enterostomy and post-enterostomy reversal. Prereversal values are shown in blue and postreversal values are shown in orange.
Discussion
Temporary enterostomy formation is a common, often life-saving management strategy for a number of congenital and acquired surgical conditions in infants. Enterostomy-related complications are encountered in a significant number of patients but those infants who are most at risk are poorly defined. In addition, published data relating to the optimal timing of enterostomy reversal are confusing, particularly with regard to the potential effect of an enterostomy on growth and weight gain such that some argue for late enterostomy reversal while others make the case for early closure with data to support either view.4 ,6 The application of standardised growth charts and z scores is a well-described method of measuring and quantifying growth during development but this technique has not been previously used to explore the relationship between enterostomy complications and timing of closure previously.10 This study reviews complications encountered in infants with small bowel enterostomies and uses z scores to assess growth before and after enterostomy reversal. A limitation of using z scores to assess growth is that it is unclear whether weight gain is true growth or extra weight such as fluid; however, when multiple weights are measured weeks apart, as in this study, it is more likely to be due to true growth.
The study finds that complications related to small bowel enterostomies are significantly more likely in infants of low birth weight and those of low gestational age at birth, the majority of which had NEC. Unfortunately with the numbers in each group it is not possible to perform regression analysis to differentiate between NEC and low gestational age. These infants were also more likely to remain in hospital and require PN prior to enterostomy closure. In the group with complications, the enterostomies were closed earlier (14.5 vs 19.1 weeks), which is likely to be related to difficulty establishing exclusive enteral feeding with concomitant PN dependence, as well as comorbidities such as chronic lung disease, which ultimately combine to prevent hospital discharge. The presence of an enterostomy-related complication is also likely to have influenced the timing of enterostomy closure in some infants although this decision was not always documented clearly in the medical records.
Published neonatal enterostomy complication rates range from 18% to 68% and the complication rate in this series was 41%.3 ,6 ,11 ,12 Several prior studies have sought risk factors for enterostomy-related complications. Singh et al12 found no risk factors but both Lee et al6 and Aguayo et al11 identified younger gestational age and smaller preoperative weight as significant risk factors. This study concurs with these two authors as complications related to small bowel enterostomies are significantly more likely in infants of low birth weight and low gestational age. Such infants, most of whom had NEC, were more likely to remain in hospital and require PN prior to enterostomy closure. Although the development of complications is multifactorial, these data highlight which patients are likely to require longer inpatient stays and the added risks that this brings. Indeed, Lee et al6 found a lower enterostomy complication rate in those with an enterostomy for a shorter period of time. A notable negative finding from this study is that siting the enterostomy through the laparotomy incision did not affect the complication rate. This is consistent with a previous study by Kronfli et al13 despite their hypothesis that those sited through a separate incision are less likely to develop infection.
A number of studies have sought to determine the optimal time to close enterostomies in infants.4 ,6 ,8 ,11 ,14 While some argue for early closure, from a weight of 1.9 kg,4 others report quite contrary views, with one study reporting that a closure weight below 2.66 kg is a significant risk factor for complications including poor growth.6 A more recent study of patients with NEC found that enterostomy reversal before 10 weeks postformation resulted in longer inpatient stay and prolonged use of PN compared with those reversed later, although they report no difference in enterostomy complications or mortality.15 Another centre reports reversal of NEC stomas at 8–10 weeks regardless of patient weight.14 It is notable that the systematic review of enterostomy closure following surgery for NEC performed by Struijs et al8 found no evidence to support either early or late enterostomy closure. In our centre, a ‘rule of thumb’ principle is used to guide the timing of closure, which includes a minimum time of 6 weeks from enterostomy formation and a preferred minimum weight of 2.5 kg. However, other factors are considered such as the need for ongoing tertiary neonatal care (such as respiratory support) and exceptions are made in those infants clearly compromised by situations such as a ‘high’ enterostomy with large volume output or a complication that renders enterostomy care challenging. These factors, along with an infant's standardised weight-for-age trend, should be used when considering the timing of enterostomy reversal.
Short-term weight gain on its own has previously been shown following ileostomy closure in NEC but standardised growth was not taken into account.4 We found a significant improvement in z score following enterostomy reversal regardless of gestational age at birth, underlying diagnosis or presence of enterostomy-related complications. This offers reassurance regarding growth in these patients who have often failed to thrive in early life. The data support consideration of early restoration of intestinal continuity in neonates with growth failure with the caveat that this decision must be balanced against the risks of early closure such as reoccurance in NEC.
This work has a number of limitations due to its retrospective nature, the content of data recorded in case notes and the heterogeneous patient group. Additionally, individual patient management was tailored by their consultant; data on issues such as perioperative management, the overall condition of the infant at the time of enterostomy formation, and availability of operating theatre time were considered unfeasible to collate in retrospect. Despite this we find that smaller, younger infants are more susceptible to enterostomy-related complications, in keeping with a number of other studies. We have also shown that the reversal of enterostomies allows infants to thrive in terms of weight gain on a standardised growth chart. Ideally more data are needed from prospective studies to confirm this finding and determine any other relevant prognostic factors.
Conclusions
Around 40% of infants with an enterostomy will have an enterostomy-related complication. Those most at risk are those babies of low birth weight and young gestational age although complications are not restricted to this high-risk cohort. Whatever their weight, gestation or underlying pathology, most infants thrive better after enterostomy closure and this should be considered when planning the optimal time for this procedure.
Acknowledgments
The authors would like to thank Dr Nim Subhedar for his assistance with accessing case notes at the Liverpool Women’s Hospital and Patrick Green for his advice regarding statistical analysis in this manuscript.
References
Footnotes
Correction notice This paper has been amended since it was published Online First. The corresponding author's email address was incorrect on the previous version of this paper.
Contributors Study design and conception (GB, SK, HC); data collection, analysis and interpretation (GB, SK, HC); drafting manuscript (GB, HC, SK); approval of final manuscript (GB, SK, HC).
Competing interests None declared.
Ethics approval Alder Hey Hospital audit and Liverpool Women's Hospital audit departments.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Database of retrospectively collected data available by request.