Article Text

Abstract
Objective To longitudinally evaluate motor development and predictive factors in school-age children with oesophageal atresia.
Design Cohort study with prospective longitudinal follow-up.
Setting Outpatient clinic of a tertiary university paediatric hospital.
Patients Children with oesophageal atresia born between January 1999 and May 2006 were assessed at 5 and 8 years of age.
Interventions None.
Main outcome Motor performance was evaluated at 5 and 8 years using the Movement Assessment Battery for Children (M-ABC). Additionally, we evaluated perinatal characteristics, duration of anaesthesia within the first 24 months, socioeconomic status, sports participation and school performance at time of follow-up and intelligence and sustained attention at the age of 8 years.
Results In 5-year-olds (n=54), the mean (SD) z-score M-ABC was slightly, but significantly lower than age-predicted normative values (−0.75 (0.83), p<0.001). In 8-year-olds (n=49), the z-score M-ABC was −0.53 (0.91) (p<0.001), intelligence was normal, but sustained attention was impaired: z-score speed (−1.50 (1.73)) and raw score attentional fluctuation (3.99 (1.90)) (both p<0.001). Motor problems mainly concerned gross motor performance. Duration of anaesthesia and sustained attention were negatively associated with motor development; sports participation was positively associated.
Conclusions Longer duration of anaesthesia and sustained attention problems were associated with gross motor problems in school-age patients with oesophageal atresia. Parental awareness of risks for motor problems may provide the opportunity to offer timely intervention.
- motor performance
- esophageal atresia
- Neurodevelopment
- developmental outcome
Statistics from Altmetric.com
What is already known on this topic?
Children with oesophageal atresia are at risk of long-term morbidity.
Mental development of oesophageal atresia patients is normal in infancy and at preschool age.
Gross motor difficulties have been reported in 5-year-old patients with oesophageal atresia.
What this study adds?
Gross motor problems persist in school-age patients with oesophageal atresia.
Oesophageal atresia patients have normal intelligence, but problems with sustained attention.
Sustained attention problems and duration of general anaesthetic procedures were negatively associated with motor performance; sports participation was positively associated with motor performance.
Oesophageal atresia (OA) is a major congenital anatomical anomaly characterised by a discontinuity of the oesophagus. It affects one in 2500 newborns and requires early neonatal surgery.1 Advances in surgical and neonatal management have progressively increased survival rates; in the absence of risk factors like extreme prematurity or major cardiac anomalies survival is nearly 100%.1 Consequently, attention has shifted from mortality towards the evaluation of long-term morbidity.
There is a growing number of studies evaluating motor and cognitive development in children who survived invasive neonatal surgery.2 Motor problems and cognitive deficits have been reported in children with congenital anatomical anomalies, including children with OA.3 ,4 Our group previously showed normal mental development but impaired motor outcome in 2-year-old3 and gross motor problems in 5-year-old children with OA.5 The above studies reported negative associations between motor performance and duration of hospitalisation, number of surgical interventions and associated congenital anomalies.3–5
As respiratory and gastrointestinal morbidity in children with OA improve with age,6 we hypothesised that motor problems at a young age will have decreased at school age. The aim of the present study was to longitudinally evaluate motor development in OA at the ages of 5 and 8 years and to identify associated factors.
Method
Participants
All newborns diagnosed with OA between January 1999 and May 2006 and subsequently treated at the intensive care unit of a level-III university hospital, that is, the Erasmus MC–Sophia Children's Hospital, were eligible. Since 1999, children born with major anatomical congenital anomalies and their families are followed by a multidisciplinary team.3 ,5 ,7–9 The Board of the Medical Ethics Committee of the Erasmus MC stated that the rules laid down in the Dutch Medical Research Involving Human Subjects Act do not apply for the present study. All parents were informed that data were used for research purposes.
Procedures
The present study is part of a structured follow-up programme for children born with OA with nine standardised assessments from the age of 6 months until the age of 17 years.3 ,5 ,7–9 The following data were collected: gender, gestational age, birth weight, ethnicity, type of OA, the presence and type of associated congenital anomalies, genetic syndromes, sepsis, duration of ventilatory support, duration of initial hospitalisation, duration of parenteral nutrition, antireflux surgery, number of procedures under general anaesthesia within the first 24 months of life, total duration of anaesthetic exposure within the first 24 months of life, and hospital admissions with duration of hospitalisation within the first 5 years. Longitudinal follow-up data are prospectively collected at 5 and 8 years of age. Motor development was evaluated by an experienced paediatric physiotherapist. Information about education, sports participation (yes/no) and physical therapeutic support (yes/no) was recorded. Psychological assessment at 8 years was performed by an experienced paediatric psychologist. We classified socio-economic status (SES) as low, middle or high based on the highest degree of maternal education.10
Primary outcome
Motor development
Motor skills were examined with the Movement Assessment Battery for Children (M-ABC).11 ,12 The M-ABC consists of separate age-related item bands with increasing difficulty as children get older. Each band contains eight items, which evaluate three domains: manual dexterity (3 items), ball (2 items) and balance skills (3 items). Until October 2012, we used the first edition of the M-ABC, but in November 2012, we switched to the second edition. Both editions contain similar content and are assumed to be comparable.13 M-ABC percentile scores are divided into three categories, namely normal, borderline and motor problem.
Secondary outcomes
Intelligence
For children born after December 2001, the Dutch version of the Wechsler Intelligence Scale for Children (WISC-III-NL) was used to assess full-scale IQ (FSIQ), total verbal IQ (TVIQ) and total performance IQ (TPIQ).13 For children born earlier, the short version of the Revised Amsterdam Intelligence Test (RAKIT)14 ,15 and the short version of the TVIQ scale of the WISC-III-NL were used. For both tests, the IQ has a mean (SD) of 100 (15) in the normative population.
Sustained attention
Attention was assessed with the Dot cancellation test (Bourdon-Vos test). This test is a continuous performance paper and pencil test that measures sustained attention in terms of speed and attentional fluctuations. Speed and attentional fluctuations are continuous variables, respectively, expressed in z-score and raw score (higher score indicating more fluctuations).16
Statistical analysis
Data are presented as mean (SD) unless otherwise indicated. To compare data of participants and non-participants, Mann-Whitney U tests were used for continuous data and χ2 tests for categorical data. The Kruskal-Wallis test was used to test for differences in neurodevelopmental outcome across SES categories. To compare data with reference values, paired samples t-tests were used for continuous data and χ2 tests for categorical data. To test for differences between 5 and 8 years, linear mixed models were used for continuous data and McNemar's tests for categorical data. Only the data of children tested at both ages were used in the McNemar's tests.
To combine the outcome scores of the M-ABC-I and M-ABC-II, percentile scores were transformed into z-scores using probit transformations (ie, an inverse normal transformation). Motor performance changes over time were investigated in longitudinal analyses using linear mixed models with z-score M-ABC as dependent variable (with mean=0 and SD=1, reference population). In each model, the independent variables were age and one of the following predictors: birth weight, the presence of associated congenital anomalies, ventilatory support, sepsis, duration of parenteral nutrition, duration of general anaesthetic events and duration of hospitalisation. A random intercept was included to account for the within-subject correlations. Linear mixed models allow subjects for who some data are missing to be included in the analyses, provided that the data are missing at random, as explained previously.7 Correlation of motor performance between ages 5 and 8 years was calculated using the intraclass correlation coefficient.
With the exception of the attention fluctuations score, intelligence and sustained attention scores were converted into z-scores using normative data. The raw score for attention fluctuations was compared with the mean raw score (ie, 2.3). A higher raw score means more attentional fluctuations. A paired samples t-test was used to determine whether the data of the intelligence tests had the same mean score and could be pooled.
Correlation coefficients between z-score M-ABC at the age of 8 years and sports participation and sustained attention were calculated. Furthermore, correlation coefficients between participants' characteristics and sustained attention were calculated. Pearson's correlation coefficients were calculated for continuous data and Spearman's for dichotomous data. All statistical tests were two sided; significance level was p<0.05. Statistical analyses were performed using IBM-SPSS-Statistics-21 (SPSS, Chicago, Illinois, USA).
Results
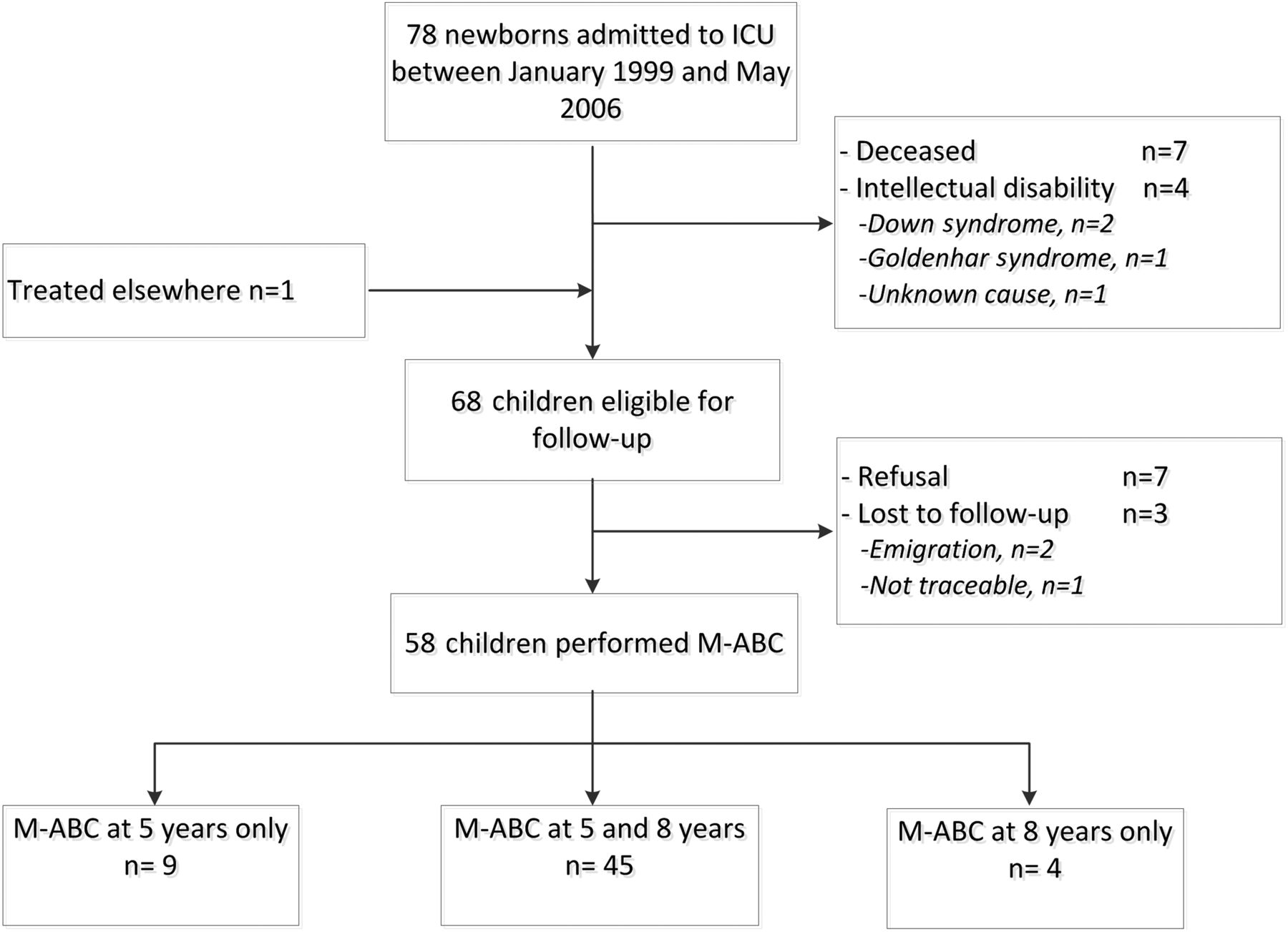
Of the 78 newborns with OA admitted between February 1999 and August 2006, seven died (9.0%). The parents of seven children refused to participate (9.0%) and three children were lost to follow-up (3.8%). One child had been operated elsewhere and was first seen at 8 years. Four children with intellectual disability ((genetic syndrome (n=3) and unknown cause (n=1)) could not be tested. Thus, 58 children were included in the analysis (figure 1).

Flow chart follow-up programme. OA, oesophagus atresia; ICU, intensive care unit; M-ABC, Movement Assessment Battery for Children.
Perinatal characteristics are shown in table 1. Surgical procedures included thoracotomy for oesophageal correction (all patients), cardiac surgery (n=3) and Nissen fundoplication (n=14).
Characteristics of participating and non-participating children
More children received physiotherapeutic support at the age of 5 than at the age of 8 years (25% vs 10%, respectively; p<0.001). Participation in sports activities did no differ between 5-year-olds and 8-year-olds (55% vs 73%, respectively; p=0.117).
Five 8-year-olds (10.2%) followed special education, 10 regular education with remedial teaching (20.4%) and 34 regular education without remedial teaching (69.4%) (χ2=2.86, p=0.239 compared with age peers in the general Dutch population) special education: 5%; regular education with extra support: 20%; and regular education: 75%).17
SES was determined for the parents of 56 participants (97%) and classified as low in 12.5% (n=7), middle in 50% (n=28) and high in 37.5% (n=21). Neurodevelopmental outcome was not different across the SES categories for: motor performance at 5 years (χ2=1.201, p=0.549) and 8 years (χ2=0.393, p=0.822), IQ (χ2=3.215, p=0.200) and sustained attention (speed: χ2=0.021, p=0.990; fluctuations χ2=0.694, p=0.707).
Motor development
Forty-five children (78%) were tested with the M-ABC at both ages (figure 1).
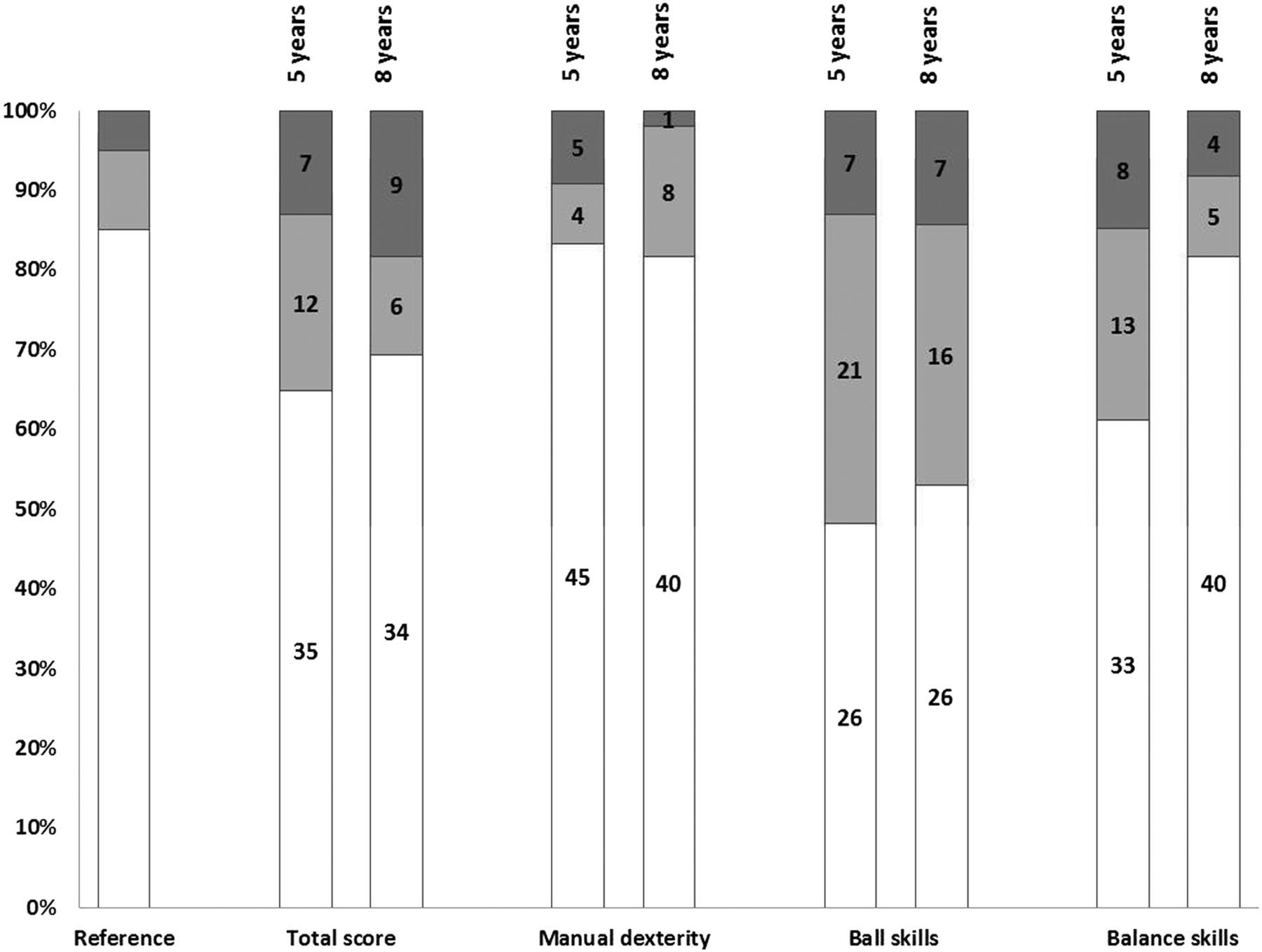
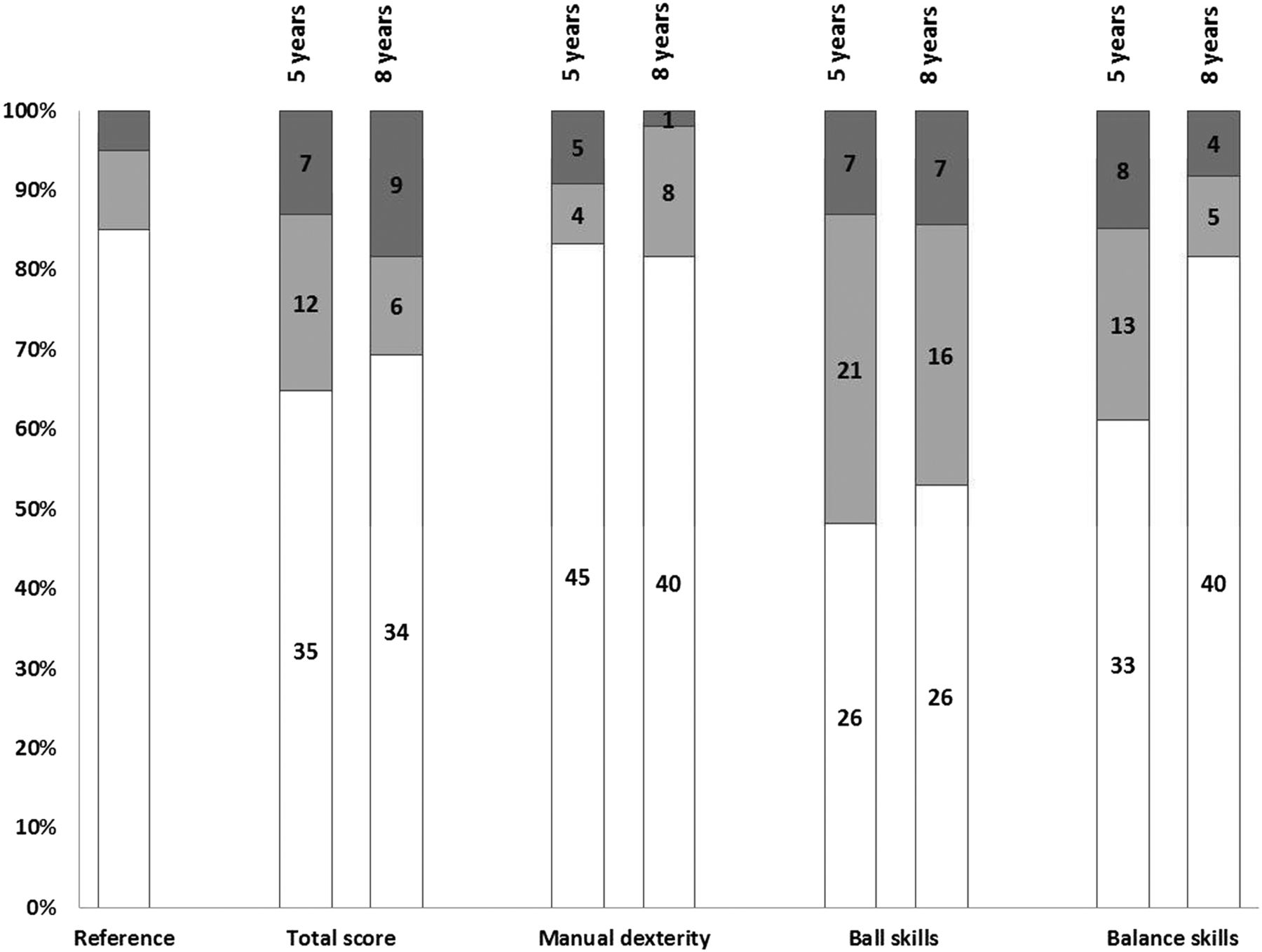
At 5 years, mean z-score M-ABC was lower than normative values (z-score M-ABC=−0.75, n=54, p<0.001). Sixty-five per cent had an M-ABC score within the normal range, which percentage is lower than that in the reference population (85%) (figure 2). Problems were observed mainly for the gross motor abilities, such as ball skills (48% normal) and balance skills (61% normal), but not for fine motor skills. One child with Opitz syndrome was included and completed the M-ABC satisfactorily at 5 years. Although the result suggested delayed motor development overall results did not change after exclusion of this child (data not shown).
{kind=link}
{kind=link}
Motor developmental outcome in 5-year-old and 8-year-old children treated for oesophagus atresia. Total Movement Assessment Battery for Children score and the separate domain scores: manual dexterity, ball and balance skills. In white, we indicate the children with normal motor development, grey represents the children with borderline motor development and in dark grey we show children with a definite motor function problem. Number of categorised children are indicated in the bars. The first bar indicates motor developmental outcome in the Dutch reference population.
At the age of 8, mean z-score M-ABC was lower than normative values (z-score M-ABC=−0.53, n=49, p<0.001). Sixty-nine per cent had an overall M-ABC score within the normal range. Considering the different domains, 53% scored within the normal range for ball skills, 82% for balance skills and 82% for manual dexterity.
Motor performance did not improve from 5 to 8 years of age (z-score M-ABC=+0.24, 95% CI −0.03 to +0.49, p=0.074). There was a significant correlation between z-score M-ABC at 5 and 8 years (r=0.346, p=0.007).
Intelligence
Intelligence was assessed in 46/49 children (full-scale WISC-III-NL, n=37; RAKIT and TVIQ of the WISC-III-NL, n=9). Data of three children who had recently been tested elsewhere were not included. The data on total intelligence were pooled, because there was no difference between the RAKIT and WISC-III-NL full-scale intelligence scores (p=0.26). Mean (SD) FSIQ was 102 (14), mean (SD) TVIQ was 103 (14) and mean (SD) TPIQ was 98 (14); the distributions of all scales were consistent with Dutch normative data.
Sustained attention
Sustained attention was assessed in 41/49 children; two missed the appointment; two had been tested elsewhere; reasons for four were unknown. Sustained attention was weaker compared with norms: mean (SD) z-score for Dot cancellation test speed −1.50(1.73); p<0.001 and mean (SD) raw score for Dot cancellation test fluctuations +3.99 (1.90); p<0.001.
Determinants of developmental outcome
Longitudinal linear mixed model analyses revealed that the duration of anaesthetic exposure within the first 24 months was negatively associated with z-score M-ABC (p=0.018) (table 2).
Associations with motor developmental outcome
At 8 years, sustained attention was negatively associated with z-score M-ABC in terms of speed and attentional fluctuations, whereas sports participation was positively associated with z-score M-ABC (table 3). Other potential risk factors, such as sepsis, prolonged parenteral nutrition or prolonged hospitalisation, did not influence developmental outcome (data not shown).
Associations with motor developmental outcome at the age of 8 years
Discussion
The present study is—to our knowledge—the first that longitudinally evaluated developmental outcome and associated factors in children operated on for OA. Assessments showed impaired motor performance up until 8 years without improvement over time. Intelligence was normal, indicating that these children do not suffer from general developmental delay. Sustained attention and duration of anaesthetic exposure within the first 24 months of life were negatively associated with motor performance.
Most of the comparable studies reported normal motor performance within the first 3 years of life in comparison with population norms3 ,4 or with healthy controls.18 In line with previous studies of our research group, the present study found impaired gross motor performance at 5 years. Further, motor development at 5 years was predictive of motor performance at 8 years, which suggests sustained risk of impairment. Similarly, in children with non-cardiac anatomical congenital malformations, motor development at 6, 12 and 24 months was predictive of motor performance at 5 years.8
In our cohort, we observed normal intelligence but impairments in sustained attention at 8 years. Little is known about long-term cognition of patients with OA; most studies found normal mental development within the first years of life.3 ,4 ,18 Two studies reported impaired intelligence at school age.19 ,20 However, these findings should be interpreted with caution because both studies were retrospective and selection bias might have occurred. Moreover, Kubota and colleagues did not report on selection procedures.20 In the present study, we found impaired sustained attention at the age of 8 years. Attention problems have also been reported in children with congenital diaphragmatic hernia and in neonatal ECMO survivors.9
Despite a normal intelligence, 10% of the children needed special education, which is twice as high as in the normal Dutch population.17 In previous literature, 11% to 53% of patients with OA had special educational needs in relation to learning disabilities, speech–language problems or intellectual disability.19 ,21
Previously identified risk factors for developmental problems, such as sepsis, prolonged parenteral nutrition or hospitalisation, were not found risk factors in the present study. In previous studies, motor performance was negatively associated with the longer duration of hospitalisation, more surgical interventions and additional congenital anomalies.3 ,5 The impact of general anaesthesia on developmental outcome is still speculative;22 studies reported associations with learning disabilities,23 behavioural problems24 ,25 and developmental disorders.25 We found a negative association of anaesthetic exposure with motor developmental outcome. This finding cannot be ignored but should be interpreted with caution because we do not know what anaesthetics were used. Still, the question is whether developmental problems can be explained by neurotoxic effects of anaesthetics. Frequent or prolonged anaesthesia may also be indicative of the presence of comorbidities that may independently affect developmental outcome.26
Approximately half of the children had impaired ball and balance skills at 5 years. Interestingly, balance skills improved afterwards as a result of more exercise. Sports participation was indeed positively associated with improved motor abilities. Although children with poor motor performance may refrain from sports activities, we believe that sports participation should be encouraged. It helps develop motor skills, increases health-related physical activity and improves quality of life.27 ,28
Some limitations should be discussed. First, data on prescribed anaesthetics were not available. All patients were operated on more than 8 years ago, when electronic patient data systems were not yet in use. Second, sustained attention could not be assessed in eight children which might have led to some selection bias. Third, assessment lasted a whole day. Although we schedule sufficient breaks, the children's performance might have been influenced by fatigue. However, the strength of this study is the highly structured follow-up with a considerable study population in view of the rare diagnosis.3 ,5 ,7–9 Lastly, we did not enrol healthy controls as this is hardly feasible for a longitudinal study in school-age children. However, within the infrastructure of routine patient care, we exclusively used standardised assessments with population norms obtained in healthy Dutch children.
Conclusions
Children operated on for OA may be at risk of long-term developmental difficulties—especially in the area of gross motor performance. Sports participation should be encouraged as it can improve motor development. The duration of anaesthetic exposure within the first 24 months of life was associated with gross motor problems. The same was true for impaired sustained attention at 8 years. Future studies should focus on neurocognitive evaluation and the effects of anaesthetics, neurotoxic drugs and perioperative management during the critical neonatal phase.
Acknowledgments
The authors thank the paediatric surgical long-term follow-up team, consisting of paediatricians, paediatric surgeons, psychologists, speech–language pathologists and paediatric physiotherapists and especially Saskia J. Gischler and Marjolein Spoel (medical staff) and Anne Zirar-Vroegindeweij and Annabel van Gils-Frijters (psychologists). Ko Hagoort provided editorial advice.
References
Footnotes
Contributors WJH collected data, performed data analysis and drafted the first version of the manuscript. FJA collected data, performed data analysis, drafted the manuscript and critically reviewed the manuscript. MHMvdC-vZ designed the study, collected data, performed data analysis, drafted the manuscript and critically reviewed the manuscript. JMvR performed data analysis and critically reviewed the manuscript. RMHW critically reviewed the manuscript. DT designed the study and critically reviewed the manuscript. HI designed the study, collected data, critically reviewed the manuscript and is responsible for the overall content as guarantor.
Funding Financially support: Stichting Swart van Essen, Rotterdam.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.