Article Text

Abstract
Background To reduce the risks of hypoxia and hyperoxia in preterm infants in the delivery room; national and international guidelines recommend titrating supplemental oxygen delivery to achieve specific oxygen saturation (SpO2) targets. Our aim was to measure the proportion of time infants <32 weeks' gestation spent within and outside prescribed SpO2 targets during the first 10 min after birth.
Method Prospective observational study using data from a preductal SpO2 sensor and oxygen analyser measuring fraction of inspired oxygen (FiO2) in the inspiratory limb of the respiratory circuit. Measurements of SpO2, heart rate and FiO2 were recorded every 2 s. We assessed compliance with the upper SpO2 limit only when infants were receiving supplemental oxygen. SpO2 measurements were recorded as being below, within or above the target at each time point. We measured the number of times infants were continuously below or above the target range for more than 30 s.
Results Twenty-seven infants; mean (SD) 28 (3.4) weeks and 962 (370) g were studied. Infants were below, within and above the prescribed targets for 28%, 35% and 37% of the first 10 min after birth, respectively.
Conclusions Preterm infants spent almost two-thirds of the first 10 min after birth with oxygen saturations outside prescribed target ranges. New titration strategies are required to reduce the risks of hypoxia and hyperoxia.
- oxygen saturation
- heart rate
- delivery room
- Resuscitation
- preterm infant
Statistics from Altmetric.com
What is already known on this topic?
International Neonatal Resuscitation guidelines advise titrating supplemental oxygen to achieve recommended specific oxygen saturation (SpO2) targets.
The SpO2 targets are derived from data from healthy transitioning term infants.
Most preterm infants receive supplemental oxygen in the delivery room (DR) to achieve the same targets as healthy newly born term infants.
What this study adds?
Preterm infants receiving supplemental oxygen in the DR spend a large proportion of time outside the intended target range.
Preterm infants in the DR are exposed to both hypoxia and hyperoxia when supplemental O2 is titrated manually against pulse oximetry SpO2 measurements.
Further studies are required to determine the optimal method of titrating supplemental oxygen in the DR to maintain desired SpO2 in the target range.
Introduction
Guidelines released in 20101 by the International Liaison Committee on Resuscitation and recently reaffirmed in 20152 recommend that oxygen therapy in the delivery room (DR) be titrated to achieve the specific oxygen saturation (SpO2) levels seen in healthy term infants. National guidelines now include specific SpO2 targets for all infants.3–7 These targets are based on SpO2 data collected from infants >37 weeks' gestational age (GA) who did not receive any intervention in the DR.8 Preterm infants generally receive supplemental oxygen after birth to achieve the SpO2 values seen in healthy term infants.8 ,9 There is accumulating evidence that even limited exposure to hypoxia or hyperoxia in the DR is harmful to preterm infants.10 ,11 Several studies have reported the results of titrating the fraction of inspired oxygen (FiO2) in the first 10 min after birth in response to SpO2. 12 ,13 There have been few studies assessing how well clinicians achieve targets when preterm infants receive supplemental oxygen in the DR. The aim of this study was to measure the proportion of time preterm infants spent within, below and above prespecified SpO2 targets during the first 10 min after birth.
Methods
Setting and patients
This was a prospective observational study conducted in the DRs (birth centre and operating theatres) of the Royal Women's Hospital (RWH), Melbourne, from March to September 2014. Any infant born <32 weeks’ GA at the RWH was eligible for inclusion. Infants were excluded if they had a congenital or chromosomal abnormality. Infants were stabilised in accordance with local guidelines, and the clinical team directed care without input from the researcher.
Study procedure
Prior to birth, an oxygen analyser (Teledyne Analytical Instruments, California, USA) was inserted into the ventilation circuit to measure FiO2 every 2 s (accuracy of ±0.02). A webcam (QuickCam Pro for Notebooks, Logitech, Switzerland) was secured to the resuscitation cot to record the resuscitation at five frames per second. Immediately after birth, a pulse oximeter sensor (LNOP Neo-L Masimo Corporation, Irvine, California, USA) was placed around the infant's right wrist and connected to an oximeter (Masimo SET, Masimo Corporation, Irvine, California, USA). The pulse oximeter was set to maximum sensitivity with 2 s averaging to provide rapid detection of changes in SpO2, heart rate (HR) and signal quality. Paired individual infant SpO2 and FiO2 trend data were recorded by physiological acquisition software (Spectra, Grove Medical, London, UK) to a desktop computer.
Infants were managed by the clinical team according to the 2012 RWH Birth Centre and Operating Theatre Neonatal Resuscitation protocol which is based on the Australian Resuscitation Council (ARC) guidelines.14 The clinical team was responsible for adjusting the FiO2. Figure 1 illustrates the clinical protocol used during the study for FiO2 titration in response to SpO2 measurements. The initial FiO2 for all infants was set at 0.3. The study was approved as an audit of practice from the RWH, Melbourne Human Research and Ethics Committee.
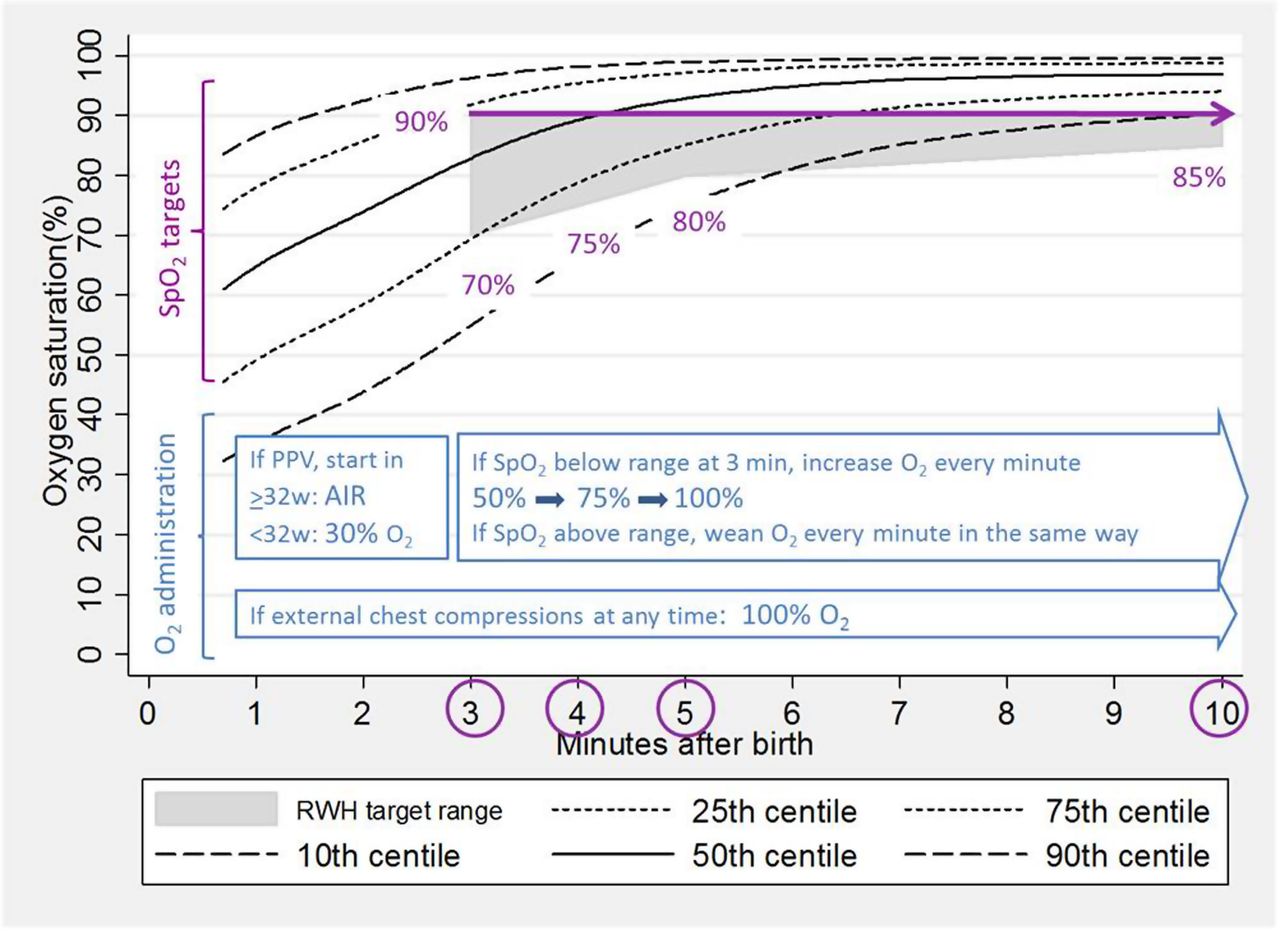
The clinical protocol for management of fraction of inspired oxygen to meet specific oxygen saturation (SpO2) targets in delivery room at Royal Women's Hospital (RWH) during the study period.
Statistical analysis
Individual infants’ SpO2, HR and FiO2 data were stored using dedicated software. Each SpO2 measurement was coded as below, within or above the prescribed RWH SpO2 target range every 2 s from 3 to 10 min after birth (figure 1). If an infant was receiving air and SpO2 measurements were above the lower limit, these measurements were classified as being within the target range. The lower limit of the target range was defined as SpO2 <70% from 3 to 4 min, <75% from 4 to 5 min, <80% from 5 to 10 min and <85% at 10 min. The measurement error of the Teledyne Oxygen Analyser is 0.02, and therefore a FiO2 >0.23 was chosen to represent oxygen therapy. Above the target range was defined as SpO2 >90% at any time between 3 and 10 min, while an infant was receiving FiO2 >0.23. Only paired data with good signal quality were included.
The proportions of time infants spent below, within and above the targets were calculated for 3–4 min, 4–5 min, 5–10 min and 3–10 min epochs. Episodes during which an infant's SpO2 remained continuously below or above the target range for more than 30 s were defined as prolonged.
Data were analysed using STATA (Intercooled V.10.0, Statacorp, Texas, USA). All data are presented as numbers with proportions for categorical variables, means with SDs for normally distributed continuous variables and medians with IQRs for continuous variables with a skewed distribution. We compared enrolled infants with eligible but not enrolled infants. Categorical data were analysed by the χ2 test or Fisher's exact test. Continuous data were analysed by Student’s t-test and normally distributed data by Mann-Whitney U test.
Results
One hundred and six infants <32 weeks were born during the study period. The research team was unavailable for the birth of 55 infants, and technical failure occurred in four infants. There was only one set of monitoring equipment; therefore, the second of 15 twin deliveries could not be studied. In addition, five infants were ineligible due to the presence of congenital abnormalities. Two infants who did not receive any interventions were included in the analysis. The characteristics of the 27 infants included in the study are shown in table 1.
Maternal and neonatal characteristics
The majority of infants received oxygen in the DR, and more than half received a FiO2 of 1.0 at some stage. Interventions received by study infants are described in table 2. Two infants did not receive respiratory support or supplemental oxygen in the DR.
Delivery room interventions*
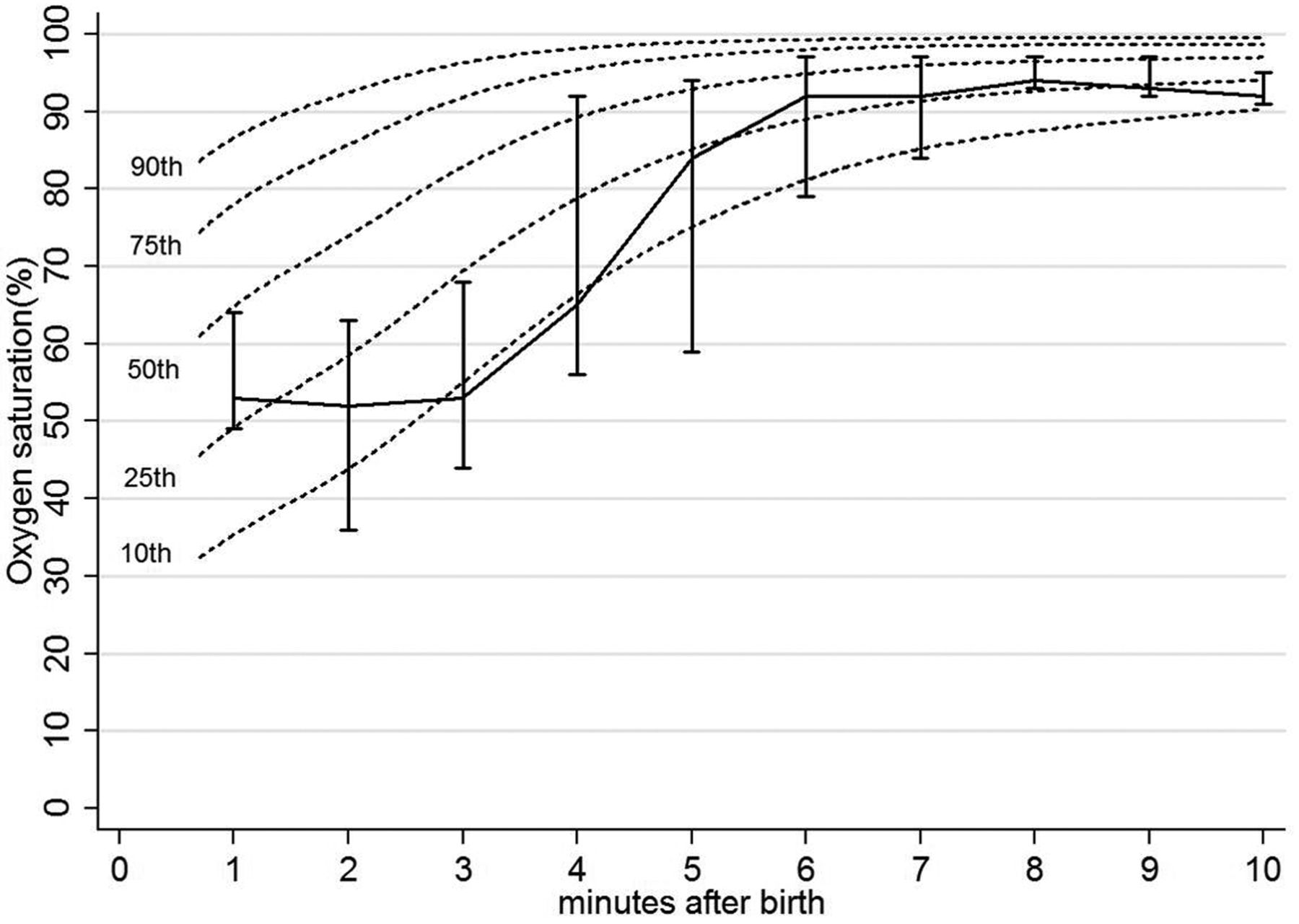
The median (IQR) time of acquisition of first data was 92 (72, 102) s after birth. The median (IQR) SpO2 at first measurement was 66 (53, 71)% and 53 (44, 68)% at 3 min of life, rising to 84 (59, 94)% at 5 min and 92 (90, 95)% by 10 min after birth (figure 2). The proportions of time infants were below, within and above SpO2 targets from 3 to 10 min after birth were 28%, 35% and 37%, respectively. In the first epoch (3–4 min after birth), infants were below, within and above the targets 62%, 30% and 8% of the time. In the second epoch (4–5 min after birth), infants spent 48% of time below, 32% within and 20% above the SpO2 targets. In the third epoch (5–10 min after birth), infants were below the targets 18%, within 36% and above 46% of the time. Table 3 details the proportion of time infants who were within and outside the SpO2 targets, median SpO2 and FiO2 during each epoch.
Proportion of time spent within prespecified SpO2 targets at different epochs after birth (n=27)

Line graph showing the 10th–90th specific oxygen saturation (SpO2) centiles for infants =37 weeks gestation.8 The vertical bars show the SpO2 (IQR) at each time point connected at the median value for study infants from 1 to 10 min after birth.
In 24 (89%) infants there were a total of 49 prolonged (>30 s) episodes when SpO2 was below the target. Nineteen (70%) infants experienced at least one prolonged episode above the SpO2 target, lasting a median (IQR) 92 (58, 180) s. Fourteen (52%) infants experienced at least one prolonged episode both below and above the target range.
The median (IQR) HR at 90 s, 2, 3, 4, 5 and 10 min after birth was 72 (92–99); 88 (71–147); 130 (100–148); 141 (109–162); 140 (117–157) and 155 (142–176), respectively.
At the time of starting 100% oxygen median (IQR), HR was 71 (52–106) bpm, 100% oxygen was started at median (IQR) 172 (133–254) s after birth and was given for median (IQR) 119 (78–275) s. Two infants were still receiving 100% oxygen at 10 min when data collection ceased. When 100% oxygen started, the SpO2 value for 10 infants was at, or below, the 10th centile; in the remaining four infants, SpO2 was at or below the 25th centile.8
Discussion
Our study found that newly born preterm infants <32 weeks’ gestation spent similar proportions of time below, within and above the hospital SpO2 targets; the greatest proportion of time was spent above the target range, most notably between 5 and 10 min after birth, exposing infants to the risks of hyperoxia. Prolonged episodes below or above the target range were common, with the median time of episodes lasting well over 1 min. This indicates that keeping preterm infants within the target SpO2 range during the first 10 min after birth is challenging.
Other studies have also reported that preterm infants in the DR spend only a small proportion of time within predefined SpO2 targets.13 ,15 ,16 In an observational study by Goos et al,15 infants <30 weeks' GA met the European Resuscitation Council (ERC) targets a median proportion only 4% of the time during the first 10 min after birth. The large proportion of time spent outside the ERC SpO2 targets is most likely to have occurred because the targets at each time point were a single value. In our study, clinicians had a broader target range of SpO2 values. In a randomised controlled trial of 106 infants <32 weeks’ gestation, Rabi et al 13 found the most successful FiO2 titration strategy to keep infants within a static 85%–92% range after birth was to initiate resuscitation in 100% FiO2, and adjust FiO2 in 20% decrements every 15 s if an infant was outside the target range and in 5%–10% decrements while SpO2 was within the target range. However, this strategy maintained infants within their target only 21% of the 5–10 min after birth. The variation of SpO2 targets and FiO2 titration strategies between studies makes it difficult to make comparisons.
We noted that saturations were frequently low during the first 3–5 min of life (figure 2); between 3 and 4 min, almost two-thirds (62%) of studied infants had a recorded SpO2 below the ARC SpO2 targets. The technology and algorithms in modern pulse oximeters have improved, but in the challenging environment of a transitioning infant in the DR, the data may be susceptible to error from poor perfusion, motion and light artefact. When the actual SpO2 is below the normal range (70%), pulse oximeters tend to overestimate the value and may not be an accurate reflection of the infants’ actual SpO2. 17 However, our findings are consistent with the study of Goos et al 15 who also found that in the first 10 min after birth, preterm infants' <30 weeks’ GA frequently had SpO2 measurements below the ERC SpO2 targets. Several observational studies have shown preterm infants have significantly lower SpO2 in the first 10 min after birth than term infants.8 ,18 ,19 As the ARC SpO2 targets are based on measurements from healthy term infants, the slower transition of preterm infants after birth and the hospital guideline of making fixed adjustments of FiO2 every 60 s may be responsible for the large proportion of time spent below the targets. The rapid decline in the proportion of low SpO2 measurements by 5 min after birth (figure 2) is likely to be due to improved aeration and an increase in the median FiO2 to 0.49 made by clinicians. The relationship between exposure to supplemental oxygen and an infant's HR and SpO2 response in the first few minutes after birth may be an important factor in a successful transition. An explanation put forward by van Vonderen et al 20 suggests that administering higher concentrations of oxygen (above room air) to preterm infants in the DR stimulates an increase in respiratory drive leading to better lung aeration. As the lungs become better aerated, the resultant increase in surface area leads to improved oxygenation, and the SpO2 measurements may overshoot the upper limit of the clinician's target resulting in periods of hyperoxia while the FiO2 is weaned. In our study, we have only reported pulse oximetry oxygen saturation data, because these data are commonly available to clinicians in DR management of preterm infants. A respiratory function monitor gives clinicians' data on pressures and volumes used during ventilation. These additional data might help clinicians to avoid hypoxia and hyperoxia. However, at this time, respiratory function monitors are not commonly available in the DR.
Our oxygen targeting protocol is designed to be pragmatic. Clinicians are encouraged to focus on ventilation after birth, to prioritise lung aeration and to use HR as a guide to an infant’s response, before adjusting oxygen therapy. This is important because HR has been identified as the most sensitive indicator of a successful response to interventions2 and a successful transition. It is reassuring that in infants managed using our protocol, HR rose rapidly from (median) 72 bpm at 90 s to (median) 130 at 3 min.
In our protocol, oxygen concentration is adjusted in three steps (once per minute) to increase FiO2 from 0.30 to 0.50 to 0.75 and finally to 1.0 in preterm infants, and likewise to decrease FiO2 to air in a similar stepwise manner. However, our study shows that adjustments in FiO2 may need to be made earlier than 3 min to assist with respiratory drive and aeration and reduce the proportion of time spent below the target range, and weaned more frequently in order to limit time spent with oxygen saturations above the desired target range.
In our study, infants spent nearly half of the third epoch (between 5 and 10 min after birth) above our target range. We observed that clinicians increased FiO2 in response to low SpO2 measurements in the first few minutes after birth. However, overshooting the SpO2 target range was common (figure 3). We found that clinicians altered the FiO2 in response to an infant's SpO2 >90%. However, infants still spent prolonged periods above the target range. Multiple studies in the neonatal intensive care unit (NICU) have shown that clinicians tend to target the higher end of a specified range for SpO2 measurements. In consequence, infants spend longer periods of time hyperoxic.21–23 van der Eijk et al suggest clinicians attempt to prevent periods of hypoxia at the expense of increased rates of hyperoxia.16 Targeting higher SpO2 values may cause longer and more frequent hyperoxia. Such exposure could potentially be reduced by effective management of FiO2, for example, weaning FiO2 down at a quicker rate and/or in larger decrements.

{kind=link}
{kind=link}
{kind=link}
Line graph showing specific oxygen saturation (SpO2) (grey diamonds) and fraction of inspired oxygen (FiO2) (darker grey boxes) of a preterm infant born at 26+4 weeks' gestation. This infant was below, within and above the Royal Women's Hospital (RWH) targets (shaded box), 37%, 16% and 47%, respectively in the first 10 min after birth.
There is no consistent definition of prolonged hypoxia or hyperoxia. Several studies in the NICU have variously defined prolonged episodes as being outside the target range for between 10 and 120 s.22–24 We defined prolonged episodes as occurring if the periods of high or low SpO2 measurement were outside the ARC target for more than 30 s. We found that prolonged episodes were common and often lasted more than 90 s. We speculate that spending prolonged periods of time below or above the targets may put infants at risk of hypoxia and oxidative stress. The potential for harm is increased in preterm infants who have poorly developed antioxidant defence systems. Future studies should determine whether a different FiO2 titration strategy reduces the frequency and duration of prolonged episodes spent outside SpO2 targets and include short-term and long-term clinical outcomes.
Our study has limitations. This affects the generalisability of our findings. Eighty-nine per cent (n=24) of infants in our study were born via caesarean section. Previous studies have shown that infants born via caesarean section take longer to reach an SpO2 >90%, and have lower SpO2 values after birth, than infants born vaginally.8 ,15 Our results may have been different had we included more infants delivered vaginally.
The SpO2 target range in our study has not been validated in a randomised trial. However, we are aware of no trials comparing different target ranges in the DR, and evidence that targeting oxygen saturation values during transition improves outcomes is lacking.
Our targets, at the time of the study, were in line with targets recommended by our national resuscitation council that recommends that the SpO2 targets for preterm infants are based on data from infants >37 weeks’ gestation who did not receive interventions in the DR. The targets in our study follow their recommendation. However, it is possible that preterm infants should have different targets compared with term infants, though this has not been tested in a clinical setting. Additionally, there is no evidence to indicate whether we should use SpO2 targets based on oxygen saturation measured in preterm infants not receiving medical interventions in the DR or those of their term counterparts.
The majority of infants in our study were not asphyctic (mean cord pH 7.30). Thus, these were mainly infants in need of stabilisation and support to aerate their lungs. It is a bit surprising that 22 of 25 infants received PPV and that 14 of 25 received 100% O2. DR resuscitation guidelines are aimed at resuscitation of infants who are not breathing. They are not so helpful when faced with a preterm infant who is breathing but requires some assistance to transition. Our data show that a SpO2 below the 10th centile was more common than a low HR to trigger the use of 100% oxygen; this may explain why so many infants received 100% oxygen.
One potential strategy to improve compliance with oxygen saturation targets is to have a device that adjusts FiO2 in response to SpO2 measurements. Several automatic FiO2 titrating systems have been trialled in the NICU.24 ,25 Claure et al 24 found that their system improved the amount of time preterm infants spent within a predefined target range of 87%–93%. Gandhi et al recently trialled the Transitional Oxygen Targeting System (TOTS), which displays an infant's SpO2 and FiO2 in real time against target SpO2 curves on a monitor in the DR, and FiO2 is manually adjusted. Infants <36 weeks’ GA in the TOTs group spent significantly more time (52%, p=0.03) within the target percentiles than the control group (37%).16
Conclusion
Preterm infants <32 weeks’ GA spent two-thirds of the first 10 min outside the prescribed ARC SpO2 target range. Further research is required to determine the best strategy to keep preterm infants within these targets. There are no randomised trials during transition comparing targeted oxygen saturation values to help guide oxygen administration in the DR. However, strategies to assess and optimise ventilation are equally important as strategies to titrate FiO2 when targeting specific SpO2 target ranges.
Acknowledgments
The authors thank clinical staff from The Royal Women's Hospital's neonatal intensive and special care unit, and the parents and infants who participated in this study.
References
Footnotes
Contributors LNW: collected, analysed and interpreted data, drafted the manuscript. JAD: conceived the study contributed to study design, collected, analysed and interpreted data, drafted the manuscript. MT, LSO, SBH and COK: contributed to study design, data interpretation and drafting the manuscript. SS: contributed to data collection. PGD: contributed to study design, data interpretation, drafting the manuscript, supervision of all aspects of the study. All authors approved the final version of the manuscript.
Funding JAD, LSO, MT and COK are recipients of a National Health and Medical Research Council (NHMRC) Postdoctoral Fellowship and who are supported by the Victorian Government's Operational Infrastructure Support Program. PGD and SBH are recipients of an NHMRC Practitioner and Principal Research Fellowship, respectively. The study was supported in part by NHMRC Program Grant No. 384100.
Competing interests None declared.
Ethics approval RWH Research and Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.