Article Text

Abstract
Background Manual resuscitation devices for infants and newborns must be able to provide adequate ventilation in a safe and consistent manner across a wide range of patient sizes (0.5–10 kg) and differing clinical states. There are little comparative data assessing biomechanical performance of common infant manual resuscitation devices across the manufacturers’ recommended operating weight ranges. We aimed to compare performance of the Ambu self-inflating bag (SIB) with the Neopuff T-piece resuscitator in three resuscitation models.
Methods Five experienced clinicians delivered targeted ventilation to three lung models differing in compliance, delivery pressures and inflation rates; Preterm (0.5 mL/cmH2O, 25/5 cmH2O, 60 per minute), Term (3 mL/cmH2O, 30/5 cmH2O, 40 per minute) and Infant (9 mL/cmH2O, 35/5 cmH2O, 30 per minute). The Neopuff was examined with three gas inflow rates (5 litres per minute (LPM), 10 LPM and 15 LPM) and the Ambu with no gas inflow.
Results 3309 inflations were collected and analysed with analysis of variance for repeated measures. The Neopuff was unable to reach set peak inflation pressures and exhibited seriously elevated positive end expiratory pressure (PEEP) with all inflow gas rates (p<0.001) in this infant model. The Ambu SIB accurately delivered targeted pressures in all three models.
Conclusions The Ambu SIB was able to accurately deliver targeted pressures across all three models from preterm to infant. The Neopuff infant resuscitator was unable to deliver the targeted pressures in the infant model developing clinically significant levels of inadvertent PEEP which may pose risk during infant resuscitation.
- Resuscitation
- Infant
- Self Inflating Bag
- T-Piece Resuscitator
- Neopuff
Statistics from Altmetric.com
What is already known on this topic?
Flow dependent T-piece resuscitators (TPRs) have become popular devices for newborn resuscitation in the developed world for term and preterm infants.
There is insufficient evidence currently to support the use of positive end expiratory pressure with positive pressure ventilation in neonatal resuscitations.
There are little data to support the use of flow dependent TPRs for infant resuscitation in the term newborn to 10 kg weight range.
What this study adds?
The flow independent Ambu self-inflating bag can deliver targeted pressures in lung models from preterm to 10 kg body weight.
The Neopuff T-piece resuscitator (TPR) design imposes increased resistance to passive lung deflation.
Neopuff TPRs used in infant resuscitation may not deliver required peak inspiratory pressure and develop significant unintended elevations in positive end expiratory pressure which may reduce the effectiveness of resuscitation.
Introduction
Resuscitation of newborns at birth in transition from the fetal state differs from resuscitation of infants and adults. The dramatic changes in pulmonary and cardiovascular systems at this time are highly interrelated with the elimination of fetal lung fluid,1 ,2 initiation of respiration and establishment of a functional residual capacity (FRC), with concurrent, unique changes in the newborn circulation. The fetal circulation with parallel ‘loops’ of the ductus arteriosus, foramen ovale and ‘placental respiration’ via the umbilical arterial/venous connections is coupled with low systemic and high pulmonary vascular resistance. The rapid and dramatic changes that occur following birth, dictate either a safe normal transition or pathological state which may require some level of assistance or full resuscitation. Surfactant deficiency, structural pulmonary immaturity together with possible disease states that can lead to preterm birth such as premature rupture of membranes, chorioamnionitis, placental disease and intrauterine growth restriction, can all affect the transition physiology and complicate both the need for resuscitation and the clinical response.
Bradycardia, asystole and apnoea require assistance with manual ventilation, and at birth, a crucial component is to support the establishment of a FRC and initiate effective alveolar ventilation.3 Provision of positive pressure ventilation (PPV) is the cornerstone of resuscitation and some form of manual ventilation device with mask or endotracheal tube is required. The devices used can be either flow independent such as self-inflating bags (SIBs) or flow dependent such as T-piece resuscitators (TPRs) or anaesthetic bag systems. Two international standards organisation (ISO) documents guide manufacturers and industry regulators as to the minimum mechanical performance expectations for these devices.4 ,5 They describe test conditions of set lung compliance and resistance to delivered tidal volume for infants and newborns less than 5 kg body mass and infants between 5 kg and 10 kg. Many brands of SIBs and TPRs are rated by the manufacturer for use in infancy/paediatrics up to 10 kg in body mass, thus crossing the two recommended weight ranges. There are little data on how these manual resuscitation systems perform biomechanically across this range of body mass (0.5–10 kg), disease states and starting cardiopulmonary states. The use of the TPR device for resuscitation at birth is widespread6–10 but there are limited data to support its use on the full term newborn (birth weight ≈ 3.5 kg) or infant (weight ≤10 kg). The Neopuff TPR (NTPR) device uses circuit flow occlusion to inflate the lung to a preset peak inspiratory pressure (PIP) and an adjustable flow resistance (figure 1) to provide preset positive end expiratory pressure (PEEP) or continuous positive airway pressure (CPAP) dependant on circuit gas in flow and delivery mode. Previous studies have focused on lower compliance (0.5–1.0 mL/cmH2O) short time constant lung models indicative of the preterm lung.11–14 A recent UK newborn resuscitation practice survey indicates that TPRs are in widespread use during term newborn resuscitation.9 In New South Wales, Australia, where over 60% of all births occur in rural or non-tertiary units,15 the NTPR is in common use for term newborn resuscitation. The recent 2015 ILCOR guideline for paediatrics16 does not provide information on inflation pressures for use in infant resuscitation. Australia has a web based resuscitation programme for healthcare professionals called RESUS4KIDS that includes information on the use of the NTPR in infancy.17 Suggested starting ventilation settings from the RESUS4KIDS site for infants requiring resuscitation (eg, with bronchiolitis) are PIP of 20 cmH2O PEEP 5 cmH2O inflow of 15 litres per minute (LPM) and a rate of 20 inflations per minute (IPM).18 Studies of infants ventilated with severe bronchiolitis indicate the need for higher levels of pressure support with reported PIPs ranging from 26 cmH2O to 40 cmH2O with inflation rates of 20–30 bpm.19–21

Cross-section diagram of Neopuff T-piece circuit. (Diagram supplied by Fisher and Paykel, Auckland New Zealand).
We aimed to examine the biomechanical performance of one brand of SIB, the Ambu Spur II (Ambu A/S Ballerup, Denmark) with fitted Ambu manometer and PEEP valve and one brand of TPR the Neopuff (Fisher & Paykel, New Zealand) infant resuscitator both rated by the manufacturer as suitable for use in infants up to 10 kg body mass in three lung/resuscitation models. These models were: an extremely preterm newborn model (body mass equivalent 1 kg), a term newborn model (body mass equivalent 3 kg) and an infant model (body mass equivalent 10 kg). Each model incorporates appropriate test lung compliance, resistance and ventilation settings. The flow dependent NTPR was tested across the range of the manufacturer’s recommended gas inflow rates22 of 5 LPM , 10 LPM and 15 LPM. Outcome measures were the delivered respiratory mechanical data at the interface of the test lung. Our null hypothesis was that both systems would perform adequately and similarly, regardless of the type of device (SIB or NTPR) or gas inflow rates to the flow dependant device (NTPR).
Methods
The preterm model consisted of a test lung with compliance of 0.5 mL/cmH2O (Draeger, Lubeck, Germany) typical of preterm surfactant deficiency with targeted ventilation parameters of 60 IPM, PIP of 25 cmH2O and PEEP of 5 cmH2O. The term newborn model consisted of a test lung with compliance of 3 mL/cmH2O (Smart Lung Infant, IMT Medical, Buchs, Switzerland) typical of an asphyxiated apnoeic infant with targeted ventilation parameters of 40 IPM, PIP 30 cmH2O and PEEP of 5 cmH2O. The infant model was based on a 10 kg 6–12-month-old child with severe bronchiolitis with test lung compliance of 9 mL/cmH2O (Michigan Instruments USA) with targeted ventilation parameters of rate 30 IPM, PIP of 35 cmH2O and PEEP of 5 cmH2O. Test lung resistance was 50 cmH2O/L/s for all three models. A single NTPR (part number: RD900AEU) and delivery circuit (part number RD 1300-10) with a measured compliance of 0.4 mL/cmH2O, tubing flow resistance of 6 cmH2O/L/s at 30 LPM and five single use Ambu SIB (SPUR II) fitted with disposable PEEP 20 valve (part number 199 102 001) and disposable manometer (part number 322 003) were used in this bench study. A Florian respiratory function monitor (RFM) (Accutronics, Medical Systems AG, Zug, Switzerland) was connected via the hot wire pneumotach and pressure sensor line sited between the device providing PPV and the test lung. The Florian monitor was calibrated with an external syringe of known volume and pressure/flow via a ventilator calibration analyser (PF300, IMT Medical, Buchs, Switzerland) with pressure resolution of 0.1 cm H2O with pressure accuracy of ±0.75%, and flow calibration with resolution of 0.05 L/min with accuracy of ±1.75%. The analogue signals output from the RFM were collected and digitised at 200 Hz with analysis software (Grove Medical, London, UK). The test lungs and monitoring system were pressurised to static pressure of 50 cm H2O and given no fall in pressure over 120 s, the system was deemed leak-free.
Five experienced paediatricians who routinely used both devices in neonatal and infant settings, were asked to provide PPV for 2 minutes to each randomly sequenced lung model at the prescribed targeted ventilation parameters using SIB and NTPR (randomly set for 5 LPM, 10 LPM or 15 LPM gas inflow). The SIB PEEP valve was set to 5 cmH2O using the attached manometer as per manufacture’s insert instructions,23 and no gas inflow was provided to SIB. When using SIB, operators targeted the prescribed lung model PIP with the attached manometer. When using NTPR the required pressures (PIP and PEEP) for each lung model were set as per manufacture’s instructions22 before each inflation run. The RFM pneumotach was re-zeroed and NTPR gas inflow were set and checked using the ventilator calibration analyser (IMT Medical) at the start of each randomised gas inflow change or lung change. Operator was blinded to RFM display and inflation rate was guided by audible metronome for each lung model inflation rate. The Spur II SIB was tested and found to comply with ISO standard for operator powered resuscitators4 for body mass range of <5 kg and 5–10 kg. The NTPR was found to comply with ISO standards for flow driven resuscitators5 for body mass range of <5 kg and 5–10 kg.
Data analysis
Analysis was conducted using Stata (V.13 MP, Statacorp, College Station, Texas, USA). The first five inflations were discarded and inflations for the next 60 s were analysed with each sequence. A total of 3309 inflations were analysed; 2613 for NTPR and 696 for Ambu SIB. Measured parameters included the PIP, PEEP, tidal volume and inflation/deflation times. The total system deflation time constant was calculated from regression on F-V loop (s) by Grove analysis software for SIBs and for the NTPR across all gas inflow rates.
Analysis of variance (ANOVA) for repeated measures was used to determine differences in delivered ventilation between device type, lung model and inflow rates. Differences between means determined by ANOVA were reported with p values adjusted F test using Box's conservative ε. p Values of <0.05 were considered statistically significant. The ANOVA for repeated measures allows a valid statistical comparison between different rates, devices and lung compliance delivered by the same individual when the repeat measurements between individuals are not independent. Bonferroni corrections of estimates were made to adjust for multiple comparisons.
Results
Preterm model
The measured mean PIPs were similar, close to targeted PIP of 25 cmH2O and not significantly different across devices and flows. The measured mean PEEPs were statistically different across device and flow with the highest mean PEEP of 6.1 cmH2O at inflow of 5 LPM with the NTPR (table 1 and figure 2). The measured mean PEEP was 4.8 cmH2O for the SIB. The measured mean inflation time was 0.30 s with SIB, and between 0.47 s and 0.48 s for NTPR p<0.001(table 1). The delivered tidal volumes were similar across all groups ranging from 10.4 mL with NTPR at 5 LPM to 11.4 mL with NTPR at 15 LPM (table 1). The mean total system deflation time constant was significantly shorter with SIB (0.06 s) and was inversely related to the NTPR inflow rate ranging from 0.21 s to 0.10 s, p<0.001 (table 1).
Measured respiratory parameters with differing resuscitation models, device type and Neopuff gas flow rates

Preterm newborn model: Set pressures 25/5 cmH2O, rate 60 inflations per minute (IPM) and test lung compliance 0.5 cmH2O/mL. NP, Neopuff; PEEP, positive end expiratory pressure; PIP, peak inspiratory pressure; SIB, self-inflating bag.
Term model
Compared with the targeted PIP (30 cmH2O), the measured mean PIPs were 30.0 cmH2O with SIB, 21.6 cmH2O for NTPR with inflow 5 LPM, 27.2 cmH2O for NTPR with inflow 10 LPM and 28.6 cmH2O for NTPR with inflow 15 LPM p<0.001. The measured mean PEEP was highest with the NTPR at 5 LPM with a mean of 6.4 cmH2O p<0.001 and lowest with SIB at 5.0 cmH2O (table 1 and figure 3). The inflation time was significantly shorter with the SIB 0.28 s compared with NTPR (0.52–0.54 s), p<0.001. The delivered mean tidal volumes ranged from 31.3 mL with NTPR with inflow of 5 LPM to 55.6 mL with NTPR with inflow of 15 LPM compared with 45.1 mL with SIB, p<0.001 (table 1). The mean total system deflation time constant was significantly shorter with SIB (0.10 s) and was inversely related to the NTPR inflow rate ranging from 0.44 s to 0.22 s, p<0.001 (table 1).

Term newborn model: Set pressures 30/5 cmH2O, rate 40 inflations per minute (IPM), test lung compliance 3.0 cmH2O/mL. NP, Neopuff; PEEP, positive end expiratory pressure; PIP, peak inspiratory pressure; SIB, self-inflating bag.
Infant model
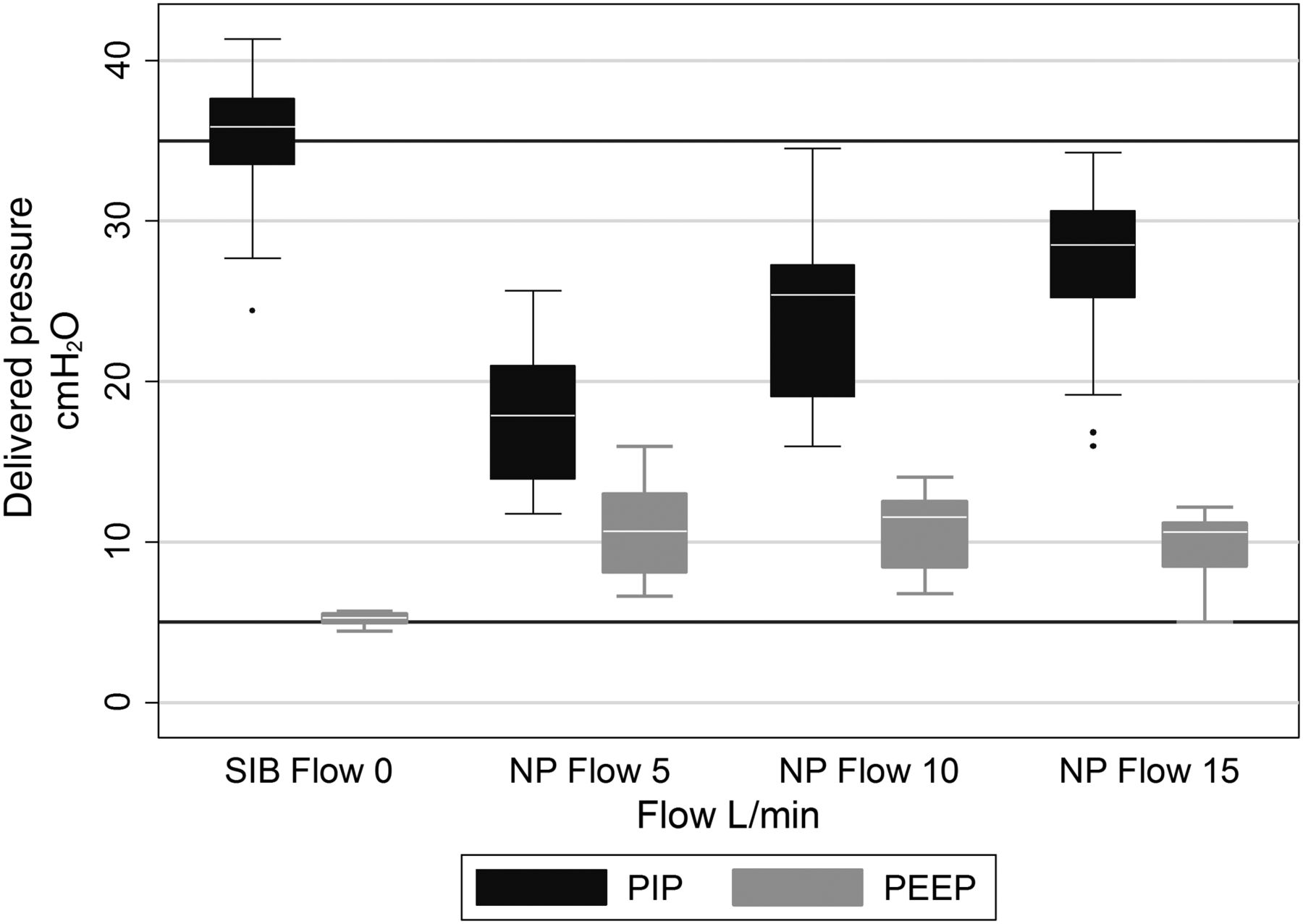
Compared with the targeted PIP (35 cmH2O), the measured mean PIPs were 35.3 cmH2O with SIB, 18.0 cmH2O for NTPR with inflow 5 LPM, 24.4 cmH2O for NTPR with inflow 10 LPM and 28.2 cmH2O for NTPR with inflow 15 LPM, p<0.001. The measured mean PEEP was 5.2 cmH2O with SIB and for the NTPR PEEP was significantly elevated at all three gas inflows ranging from 9.8 cmH2O to 10.8 cmH2O, p<0.001 (table 1 and figure 4). The mean inflation time was significantly shorter with SIB at 0.33 s compared with NTPR (0.80–0.83 s, p<0.001). The delivered mean tidal volumes ranged from 56.6 mL with NTPR at inflow rate of 5 LPM to 148.4 mL at inflow rate of 15 LPM which compared with 88.2 mL with SIB, p<0.001 (table 1). The mean total system deflation time constant was significantly shorter with SIB (0.46 s) and was inversely related to the NTPR inflow rate ranging from 2.81 s to 1.55 s, p<0.001 (table 1).

Infant model: Set pressures 35/5 cmH2O, rate 30 inflations per minute (IPM), test lung compliance 9.0 cmH2O/mL. NP, Neopuff; PEEP, positive end expiratory pressure; PIP, peak inspiratory pressure; SIB, self-inflating bag.
Discussion
This is the first study we are aware of, that examines the biomechanical performance of two common infant manual resuscitators across the manufacturers’ quoted body mass ranges. The Ambu Spur II was able to accurately deliver the targeted PIP and PEEP in all three models corresponding to body mass range of extremely preterm to 10 kg. The NTPR was not able to deliver the targeted PIP in the 10 kg infant model with performance inversely related to gas inflow rates (table 1 and figure 4). The NTPR in the infant model exhibited seriously elevated inadvertent PEEP levels with means similar across all three gas inflow rates (table 1). Tidal volumes were noted to be excessive with the preterm model assuming a 1 kg infant with mean volumes between 10.4 mL/kg and 11.4 mL/kg for both devices. Similarly in the term model, assuming a 3 kg infant, the mean TV ranged from 10.4 mL/kg with NTPR at 5 LPM to 18.5 mL/kg at 15 LPM compared with the Ambu SIB with a mean value of 15 mL/kg. In the 10 kg infant model, the mean tidal volumes ranged with the NTPR from 5.6 mL/kg at 5 LPM to 14.8 mL/kg at 15 LPM compared with 8.8 mL/kg with the Ambu SIB. We speculate that the greater tidal volumes observed with NTPR at flow rates 10 LPM and 15 LPM in the term and infant models are related to the longer inspiratory times due to operators attempting to reach required PIP. The impact of excessive tidal volumes may be mitigated by mask leak however; this is clinically unmeasured and highly variable. Further, should the clinically unrecognised mask leak be ‘corrected’ by improved mask technique24 or endotracheal intubation, the infant may be exposed to a potentially large change in delivered tidal volumes.
Limitations of our study are shared with other manikin and test lung studies of the ability to generalise results to actual human resuscitations. Further, our results cannot be used to comment on the performance of other brands of TPRs or SIBs.
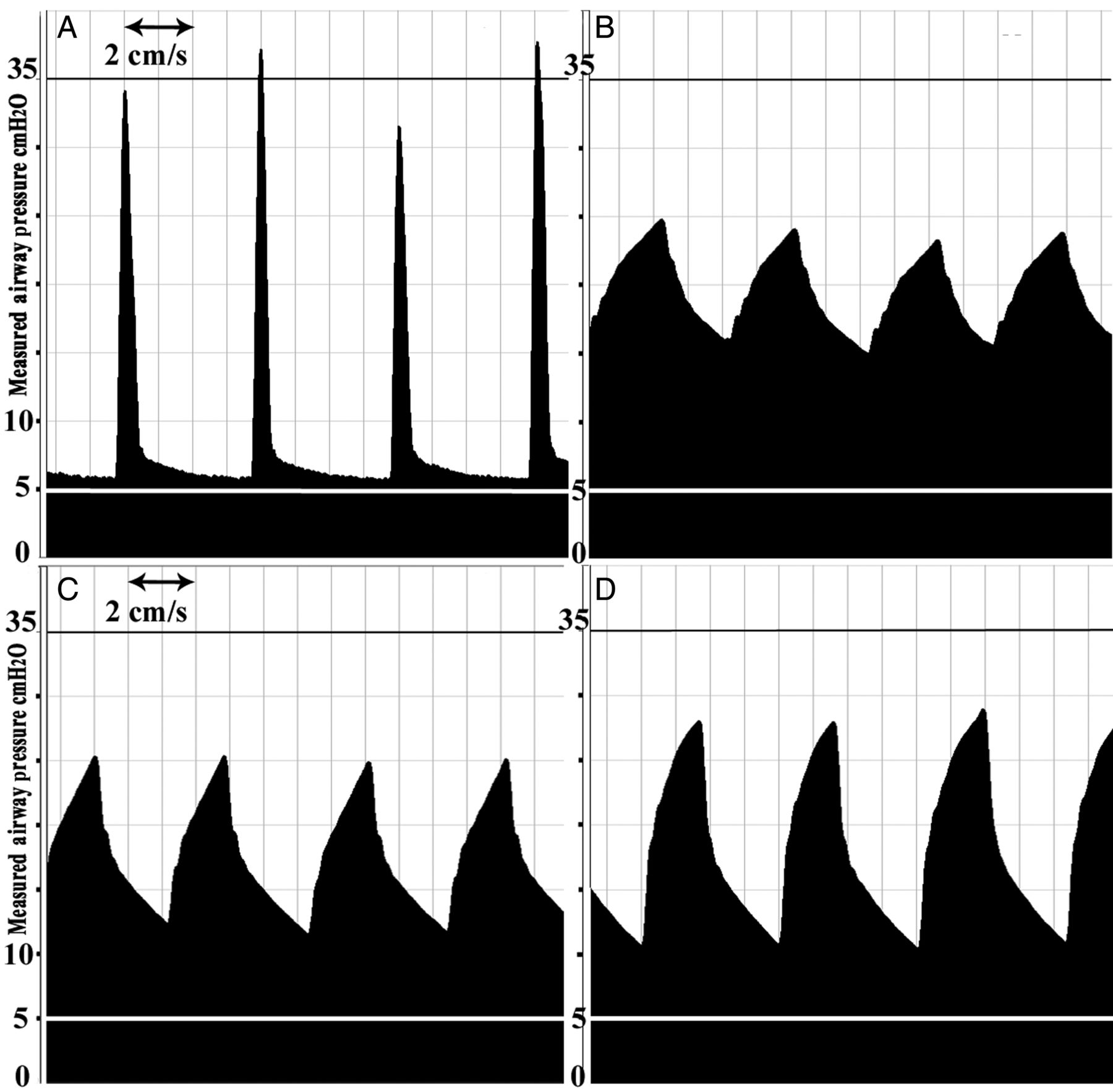
The measured total system deflation time constant (table 1) incorporates both test lung and device imposed resistance and compliance to provide the Grove Spectra derived value. Three lung deflation time constants are required to allow 95% of the previous tidal volume to deflate passively.25 ,26 Device imposed expiratory resistance increases total respiratory system time constant that can result in incomplete emptying of the previous inflation volume, possible inadvertent PEEP with the potential for gas trapping, and increase in lung volume. In an infant this can increase distal airway pressure in the alveoli resulting in decreased lung compliance, and pulmonary air leak.27–30 The mean total system deflation time with SIB in our infant model was 0.46 s which was less than the measured lung deflation time of 1.67 s at a delivery rate of 30 IPM. This explains the lack of any significant inadvertent PEEP observed. In the infant model using NTPR for all three gas inflow rates (5 LPM, 10 LPM and 15 LPM) total system deflation time constants (2.81 s, 1.92 s and 1.55 s) were greater than measured deflation times (1.17 s, 1.19 s and 1.20 s). This indicates insufficient lung deflation time resulting in the observed inadvertent PEEP (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Recordings of infant model airway pressure waveforms for Ambu self-inflating bags (A) and Neopuff T-piece resuscitators at flow rates of 5 litres per minute (LPM), 10 LPM and 15 LPM (B–D).
The results of our study indicating an inability of the NTPR to deliver PIP close to those set in the 10 kg infant model combined with the inadvertent PEEP observed suggest, effective resuscitation of infants with similar lung compliance could be inadequate. The compliance setting we chose for our term lung model may be considered conservative (3 mL/cmH2O) with some human studies suggesting higher term infant values (4–5 mL/cmH2O).31 ,32 This could alter performance of the NTPR at all gas inflow rates in term resuscitation with the development of clinically important inadvertent PEEP.
The provision of a set PEEP is determined in the NTPR by gas inflow rate and the dialled flow resistance of the adjusted PEEP setting (figure 1). The NTPR and the Ambu SIB with both manometer and PEEP valve would allow appropriate manual inflations for preterm infants given the data in this study and our previous work demonstrating adequate and consistent PEEP delivery with the Ambu SIB with PEEP valve.33 However, Finer et al reported eight occurrences out of 120 video studies of actual resuscitations of preterm newborns <1 kg using NTPR of seriously elevated PEEP levels above set values. The range of measured PEEP in these cases was 6.7 cmH2O to 15.8 cmH2O with set PEEP of 5 cmH2O. Finer concluded ‘the NTPR has the potential to cause an inadvertent and potentially toxic increase of PEEP which might not be noticed by the operator’.12 Hinder et al29 recently showed in preterm and term lung models an associated rise in PEEP with rising lung compliance at different PIPs when using NTPR.
Disease states in newborns such as meconium aspiration, bronchopulmonary dysplasia and bronchiolitis or severe asthma in infants requiring mask ventilation may have significantly elevated FRCs or air trapping and so may respond adversely to the levels of inadvertent PEEP seen with the NTPR. The Ambu SIB with PEEP valve delivers consistent and accurate PEEP levels in the infant model approximating a 10 kg infant in our study without the risk of inadvertent PEEP.
The attraction of the TPR devices is their ability to deliver preset pressures, provide sustained inflations and deliver a continuous positive end expiratory pressure (CPAP) via mask in newborns and infants with serious respiratory distress who do not require positive pressure inflations. The NTPR is frequently used to stabilise breathing infants needing CPAP in New South Wales Australia.18 Given the results in our study, inadvertent PEEP may be a serious issue complicating the use of the NTPR used to provide CPAP in a spontaneously breathing infant.
Conclusion
The Ambu Spur II with fitted manometer and PEEP valve accurately delivered targeted PIP and PEEP across the three models corresponding to the manufacturer’s quoted body mass range. The NTPR accurately delivered targeted set PIP and PEEP in the preterm model, in the term model with inflow rates of 5 LPM it could not deliver targeted PIP with some degree of inadvertent PEEP, and in the infant model it could not deliver targeted set PIP with significant inadvertent PEEP at all inflow rates (5–15 LPM). The manufacturer should consider the value of inflow rates of 5 LPM and the upper range of body mass suitable for use with this device.
Acknowledgments
The authors thank Ambu Australia for supply of self-inflating bags to examine in this study.
References
Footnotes
Contributors MT is primary researcher responsible for conceiving, designing, data collection, statistical analysis and writing manuscript. RM and DS contributed towards interpretation, manuscript construction and review. DS contributed to interpretation, manuscript construction and review. MH contributed by assisting in design, data collection, statistical analysis, manuscript writing and review.
Competing interests None declared.
Ethics approval This study was approved by the Western Sydney Local Health District Human Research and Ethics committee (SAC2014-5-6.9(3999)).
Provenance and peer review Not commissioned; externally peer reviewed.