Article Text

Abstract
Objectives Determine how consistently providers follow neonatal resuscitation programme (NRP) guidelines in the management of asystolic infants requiring intensive resuscitation in a simulated environment and determine time to first administration of intravenous adrenaline.
Design Neonatal fellows (n=10) underwent delivery room simulation involving an asystolic infant as part of their educational curriculum. Each intervention performed by the resuscitation team during the scenario was timed and compared against recommended timeline (RT) as suggested by NRP.
Results Ten simulations were conducted. Heart rate auscultation and initiation of positive pressure ventilation occurred on average within 10 s of the RT. Asystole was correctly identified by auscultation in 6 (60%) cases. Initiation of cardiopulmonary resuscitation on average was 60 s later than RT. Time to place an umbilical catheter was almost twice the RT (354±100 s) and time to first dose of intravenous adrenaline was almost 120 s later than the RT. Average time to discontinuation of resuscitation was 17 min, 43 s, which was 10 min, 42 s after initial intravenous adrenaline.
Conclusions Critical resuscitation steps during intensive resuscitation often occur later than the RT. Identifying asystole by auscultation is difficult, takes time and can delay responses. Even a trained team during a simulation code took over 7 min to administer the initial dose of intravenous adrenaline. Recommendations related to discontinuation of resuscitation should clearly delineate what constitutes effective resuscitation (minimum of early intubation, intravenous adrenaline). We recommend the ‘timer’ to discontinuation of resuscitation only starts following the first dose of intravenous adrenaline.
- Resuscitation
- Neonatology
Statistics from Altmetric.com
What is already known on this topic
Early data from the 1980s and 1990s indicated that babies with a heart rate of 0 at 10 min after delivery were likely to have poor outcome.
Therapeutic hypothermia appears to have modified the long-term outcome in such cases.
Current recommendations are to consider discontinuation of resuscitation with no detectable heart rate for 10 min.
What this study adds
During simulated resuscitation, the initiation of chest compressions and intravenous adrenaline administration occur later than recommended.
Recommendations for timing need to be revised and based on real-world observation.
Guidelines recommending discontinuation of resuscitation with no heart rate for 10 min need to be revisited.
Introduction
The overwhelming majority of newborns do not require any resuscitation in the delivery room.1 Approximately 10% require assistance to start breathing, but <1% require intensive resuscitation (chest compression±adrenaline (epinephrine)).2–4 Infants born with an absent heart rate (HR) at birth that extends through 10 min remains a rare event with the exact incidence unknown. Data from the pre-hypothermia era indicated that babies with an HR of 0 at 10 min after delivery were likely to die or have severe neurological deficits in survivors.5 However, the introduction of therapeutic hypothermia (TH) appears to have modified the long-term outcome for these babies. In a recent report of five studies (including three randomised hypothermia studies) totalling 90 infants with an Apgar of 0 at 10 min, with 56 treated with hypothermia and 34 controls, a primary outcome of death or abnormal neurodevelopmental outcome (18–24 months) occurred in 73% of cooled and 79.5% normothermic infants.6 Thus, the potential of a normal outcome has substantially improved compared with earlier studies (from ∼0% to ∼25%). Whether this reflects potential benefits of TH and/or more effective resuscitation interventions remains unclear. The most recent recommendation from the International Liaison Committee on Resuscitation (ILCOR) (2010) states, “In a newly born baby with no detectable heart rate which remains undetectable for 10 minutes, it is appropriate to then consider stopping resuscitation”. “The decision to continue resuscitation is complex and maybe influenced by several considerations including the availability of TH”.1 A critical gap in the ILCOR statement is a failure to categorise more explicitly what constitutes effective and timely resuscitation, and when the 10 min timeframe actually begins. Additionally, the decision to discontinue resuscitation remains a challenging one.
Neonatal fellows and attendings are expected to be competent in the resuscitation of the asystolic newborn in the delivery room. It has been found that most newborns requiring resuscitation do not receive interventions according to a recommended timeline (RT) and the median time taken to perform all tasks is greater than the recommendations.7 Exposure to this and other complex delivery room scenarios is limited in real life but can be augmented with finely orchestrated teamwork and deliberate practice optimally achieved in the simulated environment.
As part of the standard neonatal fellowship curriculum at our institution, fellows leading a resuscitation team undergo simulations related to a wide-ranging number of clinical scenarios, one of which is the management of the asystolic term newborn in the delivery room. Simulations are video recorded and there are debriefing sessions after each simulation to discuss the medical aspects of the scenario including timing, sequence and effectiveness of interventions, how the fellow/team responded to the specific scenario and management issues that can be handled differently if presented with a similar scenario in the future.
A recent clinical case of an asystolic infant who eventually achieved recovery of spontaneous circulation well beyond the ‘10 min’ timeframe, when reviewed, indicated that some of the life-saving interventions were performed beyond the suggested neonatal resuscitation programme (NRP) timeline. Using this case as a framework, we sought to determine the sequence and timeliness of interventions in a simulation model of asystole at birth using a high-fidelity neonatal simulator. We specifically focused on the sequence of intubation relative to the initiation of chest compressions and the timing of the first dose of intravenous adrenaline. Our hypothesis was that effective resuscitation and the ability to achieve restoration of spontaneous circulation requires two components: the establishment of functional residual capacity and administration of intravenous adrenaline to increase diastolic blood pressure and coronary perfusion pressure. The study objectives were twofold: first, to determine in a simulated environment how consistent providers are in following the NRP guidelines in the management of an infant requiring intensive resuscitation including chest compressions and the intravenous administration of adrenaline, and second, to determine the time to first administration of intravenous adrenaline.
Illustrative case
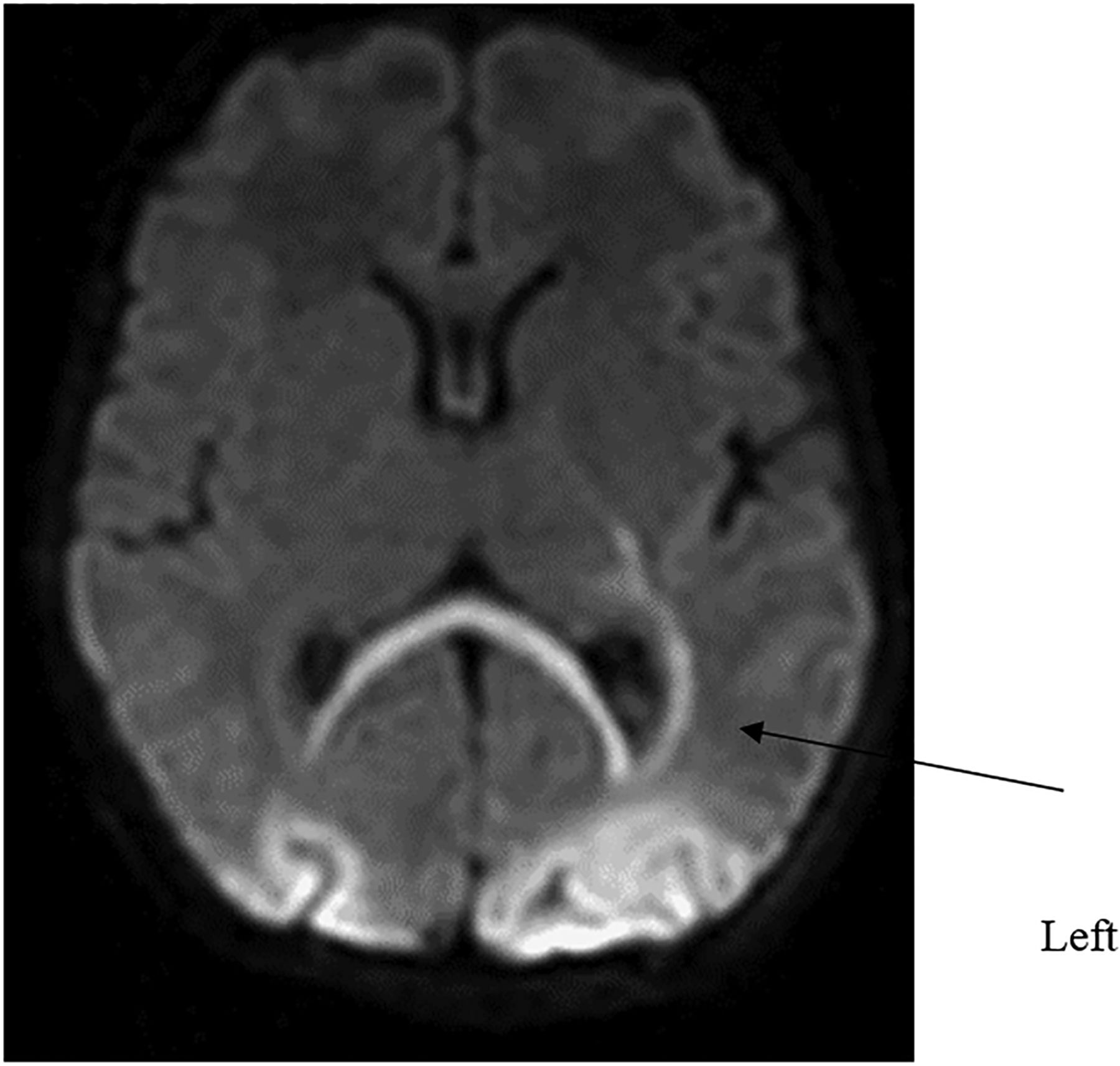
Baby boy M was born at 37 5/7 weeks weighing 3250 g to a 34-year-old mother via repeat caesarean section secondary to arrest of descent after failed vaginal birth after caesarean. He unexpectedly emerged limp, apnoeic and poorly perfused and was placed on a warmer, dried and stimulated but remained apnoeic. The timeline of resuscitation can be seen in figure 1. Positive pressure ventilation (PPV) was initiated and there was no HR appreciated upon auscultation. At 1.5 min of life, he was intubated with resulting chest rise and equal breath sounds. Chest compressions were initiated immediately after intubation. A dose of adrenaline (1 mL/kg) was given via the endotracheal tube (ETT) at 6 min with a repeat ETT (1 mL/kg) dose given at 9 min. At 12 min of life, an umbilical venous catheter (UVC) was eventually successfully placed, and the first dose of intravenous adrenaline (0.3 mL/kg) was given. There continued to be no appreciable HR, and a 10 mL/kg normal saline bolus was given. Repeat intravenous doses of adrenaline were administered at 15 and 18 min. At 20 min, packed red blood cells were arbitrarily given. At this point, the family was counselled regarding the potential poor prognosis and the consideration for discontinuation of cardiopulmonary resuscitation (CPR) was discussed. Concurrent with the discussion at approximately 27 min, the baby was noted to be making some respiratory effort and the HR was auscultated as >100 bpm. The Apgar score at this time was 3 (2 for HR and 1 for respiratory effort). He was transferred to the neonatal intensive care unit at 32 min with HR>100 bpm and good air entry bilaterally. The umbilical cord arterial blood gas showed a pH 7.20, pCO2 60, pO2 16 and base excess (BE) −4.5, and the baby's initial arterial blood gas showed a pH 6.99, pCO2 33, BE −23 and lactate 16. The baby was assessed at 1 h of age and was determined to have severe encephalopathy. The amplitude integrated EEG at that time showed severe suppression, and selective head cooling was started at 90 min. During cooling, he exhibited seizures. The MRI scan on day of life (DOL) 7 was abnormal (figure 2). The study revealed restricted diffusion involving left posterior limb of the internal capsule and restricted diffusion most pronounced in the left parieto-occipital cortex, involvement of the splenium of the corpus callosum, as well as subdural haematomas in the posterior fossa. He was taking full oral feeds by DOL 10 and was discharged home on DOL 12. At his 18-month follow-up, he had evidence of a right-sided hemiparesis (predominantly affecting the upper extremity), but was mobile with a cognitive score of 85 (done with the Bayley Scale of Infant and Toddler Development).
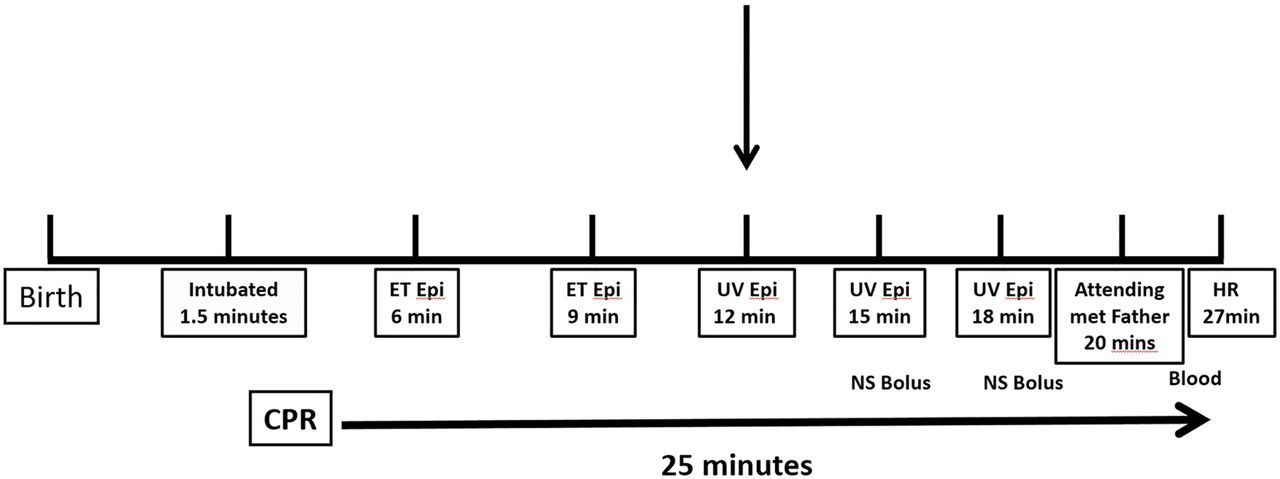
Timeline of interventions during the clinical case requiring intensive resuscitation. CPR, cardiopulmonary resuscitation; ET, endotracheal; HR, heart rate; NS, normal saline.
{kind=link}
{kind=link}
MRI on day of life 7—note the restricted diffusion involving left posterior limb of the internal capsule and the restricted diffusion most pronounced in the left parieto-occipital cortex, (arrow) as well as involvement of the splenium of the corpus callosum.
Methods
Neonatal fellows (n=10) underwent a delivery room simulation involving an asystolic infant as part of the standard educational curriculum. The resuscitation team, which includes a neonatal fellow, neonatal nurse practitioner and neonatal intensive care unit nurse, was called urgently via the standard resuscitation code call system, on 10 separate occasions to the simulation room, located adjacent to Labor and Delivery. They were given the scenario of a term baby, with a history of acute onset bradycardia being delivered via emergent caesarean section. The SimNewB simulator (Laerdal Medical) was used to perform resuscitation. Each intervention performed by the team was timed and included the following: time to application of PPV, time to assessment of HR, accuracy of HR assessment, time to intubation and time to discontinue resuscitation. The time of each step of resuscitation was recorded and entered on a checklist, which indicated the desired steps in sequence (table 1). The HR sound was set at near maximum in all cases. The recorded times were then compared against the ‘recommended times’ as suggested by NRP.8 It was emphasised as part of our practice that intubation should precede chest compressions and the adrenaline should be administered intravenously. The attending was called during each scenario and made the decision to discontinue resuscitation. As a division, it had been discussed that discontinuation of resuscitation in an asystolic infant should be considered only after 10 min following an initial dose of intravenous adrenaline. Each resuscitation was video recorded and a debriefing was conducted with all team members shortly after each simulation.
Timeline of simulated interventions in the delivery room compared with recommended times
Results
A total of 10 simulations were performed. The RT and average recorded time for each intervention can be seen in table 1. Auscultation of HR occurred at 26±15 s and initiation of PPV at 40±15 s, both interventions occurring on average within 10 s of the RT. Placement of a preductal pulse oximetry probe occurred at 157±120 s, almost a full minute later than the RT. Initiation of CPR also occurred, on average, 60 s later than the RT of 60–90 s. The time to place an UVC was almost twice the desired goal (354±100 s). The time to administration of the first dose of adrenaline was >120 s later than the desired time at ∼390 s. The time to intubation proceeded the time to initiation of CPR in 7/10 (70%) scenarios. Asystole was only correctly identified in 6/10 (60%) scenarios. An HR was perceived as present in 4/10 (40%) scenarios. The average time of cessation of resuscitation was 17 min and 43 s, and the average time between the first dose of adrenaline and cessation of resuscitation was 10 min and 42 s.
Discussion
The findings in this simulation conducted study indicate that when a resuscitation team is called to the delivery/simulation room for a newborn with bradycardia and/or asystole there are numerous challenges that may influence the quality of the resuscitation. First, key resuscitation interventions occurred later than the RT and included a delay in initiating chest compressions, delay in placement of the UVC, and consequently, the administration of the first dose of intravenous adrenaline. This reinforces the findings of McCarthy et al,7 who showed that the initial steps of resuscitation did not occur within the timeframe recommended in resuscitation guidelines. Additionally, these findings highlight the fact that discontinuation of resuscitation with an absent HR for 10 min despite resuscitation may be premature and not have allowed sufficient time for potentially effective resuscitation interventions to have occurred. Moreover, our clinical and simulated findings illustrate that intensive resuscitation requires skill and teamwork.
Neonatal resuscitation success has classically been heralded by an increase in HR determined by auscultation. HR also determines the need for changing interventions and escalating care. HR assessment is a challenge faced by resuscitation teams. Indeed, while the HR assessment by auscultation occurred very close to the RT in all 10 scenarios, asystole was only correctly identified 60% of the time. This is similar to the findings of Chitkara et al,9 who showed in a simulated model that errors in HR determination by either palpation or auscultation varied from 26% to 48% of initial assessments and from 26% to 52% of subsequent overall assessments. This highlights the critical need for an improved method of newborn HR assessment in the delivery room, particularly in the infant requiring resuscitation. Pulse oximetry (PO) is the current recommendation by ILCOR; however, several recent studies have shown that PO does not provide a rapid assessment, and in many cases underestimates the HR, potentially leading to unnecessary interventions. In 2012, Mizumoto et al10 compared the use of PO and ECG in HR rate assessment in the delivery room and found that in 20 observed deliveries ECG took an average of 38 s to determine HR while PO took over 2 min. This finding was supported by another recent study by van Vonderen et al,11 who evaluated PO versus ECG HR assessments every 30 s over the first 10 min of life. This group found that PO took longer than ECG to provide an HR reading and that PO underestimated the HR falsely detecting bradycardia in up to 50% of the cases in the first few minutes after birth. In the clinical case presented in this report, auscultation was the method used to detect HR. We speculate that there was likely a low but clinically undetected HR.
At our institution, it is preferred practice to intubate a baby prior to the initiation of CPR. This is based on the principle that effective ventilation is the most important intervention in the restoration of circulation, in the bradycardic or even ‘asystolic’ newborn and that the initiation of chest compressions may interfere with the ability to deliver effective ventilation via facemask. In a 2014 manikin study by Huynh et al,12 trained neonatal providers were unable to assess the effectiveness of ventilation via facemask during synchronised chest compressions. In this study, we observed that the average time to intubation preceded the average time to CPR by approximately 30 s. We also educate our trainees that intravenous adrenaline should be used in resuscitation, given the lack of beneficial evidence regarding the role of endotracheal adrenaline in this clinical situation. Moreover, Barber and Wyckoff4 showed the time of spontaneous circulation after the last dose of adrenaline was shorter after intravenous adrenaline compared with ETT adrenaline responders. Intravenous adrenaline was administered as the first dose immediately following UVC placement in every simulated case. In the clinical case, two doses of adrenaline were given via the ETT because of the difficulty in placing an UVC line.
The limitations to this study include a convenient sample size. Although a manikin study, this should not have affected the timeliness of responses. Similar delays in resuscitation were noted in the clinical case. Importantly, the time sequence used in the study as recommended by NRP (8) has not been rigorously evaluated, but rather reflects good practice guidelines. Moreover, other international resuscitation councils may use different timelines.
The clinical case of the asystolic newborn in this report provides a real-life illustration of many of the observations noted during the simulations. While it is likely that CPR was excellent, it is also plausible that the infant was not asystolic for 27 min, rather that the HR was not detected by auscultation, consistent with what was observed during the simulations. Additionally, we speculate, although intubated there was a component of ineffective ventilation that contributed to asystole.3 The NRP recommended time for placement of an UVC is at approximately 3–4 min into a resuscitation. In this study, we observed that the average time to UVC placement was almost 6 min, and in the case presented, the UVC was only successfully placed at 12 min with the first intravenous dose of adrenaline administered shortly thereafter.
Conclusions
The optimal timing of discontinuing resuscitation of a newborn in the delivery room remains an unresolved clinical dilemma for the clinician. This observational simulation study, along with the illustrative clinical case, should encourage neonatologists and other care providers to rethink the timing of cessation of resuscitation. Starting the clock at the time of birth is premature, potentially leading to the cessation of resuscitation of infants with potentially favourable long-term prognoses. We suggest that the clock should start ticking following the first dose of intravenous adrenaline. To achieve optimal resuscitation technique, deliberate practice in the simulated environment is essential.
References
Footnotes
Contributors SM conceptualised and designed the study, ran the simulations, conducted the debriefings, drafted the initial manuscript and approved the final manuscript as submitted. JP contributed to study design, assisted with the simulations, reviewed and revised the manuscript and approved the final manuscript as submitted.
Competing interests None declared.
Ethics approval The neonatal simulation educational programme, while conducted as a quality improvement initiative, has been approved by the institutional review board of Weill Cornell Medical College.
Provenance and peer review Not commissioned; externally peer reviewed.