Article Text

Abstract
Objective To analyse the delivery room management of babies born between 22 and 26 weeks of completed gestational age and to identify the factors associated with the withholding or withdrawal of intensive care.
Study design Population-based cohort study.
Patients and methods Our study population comprised 2145 births between 22 and 26 completed weeks enrolled in the EPIPAGE-2 study, a French cohort of very preterm infants born in 2011. The primary outcome measure was withholding or withdrawal of intensive care in the delivery room.
Results Among infants born alive at 22–23 weeks, intensive care was withheld or withdrawn for >90%. At 24 weeks, resuscitative measures were withheld or withdrawn for 38%, at 25 weeks for 8% and at 26 weeks for 3%. Other factors besides gestational age at birth associated with this withholding or withdrawal for infants born at 24–26 weeks were birth weight <600 g, emergency delivery (within 24 h of the mother's admission) and singleton pregnancy. Although rates of withholding or withdrawal of intensive care varied substantially between maternity units (from 0% to 100%), the variability was primarily explained by differences in distributions of gestational age at birth.
Conclusions Although gestational age is only one factor predicting survival of preterm infants, practices in France appear to be based primarily on this factor, which thus has direct effects on the survival of extremely preterm infants. The ethical implications of basing life and death decisions only on gestational age before 25 weeks require further examination.
- Neonatology
- Epidemiology
Statistics from Altmetric.com
What is already known on this topic
Decision-making for extremely preterm infants is ethically complex and wide variations of practice exist within and between countries.
Decision-making is often based on gestational age.
What this study adds
In France, decision-making for providing resuscitative measures is based almost exclusively on gestational age.
In our population-based study, we found that there were no survivors at gestational ages <24 weeks and that survival at 24, 25 and 26 weeks remained lower (31%, 60% and 75%, respectively) than those in other countries with active policies for neonatal resuscitation before 24 weeks.
Introduction
Despite the medical advances of the past 30 years, extremely preterm infants remain at high risk of death, neonatal morbidity and neurodevelopmental impairment.1–7 Accordingly, intensive care decisions for these births continue to raise important ethical questions and controversies about the appropriateness of either intensive life support or comfort care. Determining the criteria on which doctors and parents can base an ethically acceptable decision remains difficult. Although gestational age is imprecise and only one of several factors predicting survival and long-term outcomes, it is still used for decision-making in the delivery room in many countries.8 While many countries have defined grey zones of gestational age ranges within which prognosis is uncertain and decisions to provide intensive care are made on a case-by-case basis,9 they often delineate borders of the zone differently.7 ,10–14 Some countries, such as Switzerland and the Netherlands, are more hesitant to provide intensive care9 ,15 while other countries, such as Sweden and Japan, are more prone to intervene.16 ,17 Delivery room survival rates thus differ widely between countries ranging from 8% to 84% at 23 weeks and 60–93% at 24 weeks. Consequently, rates of survival to discharge also vary widely, ranging from 1% to 52% at 23 weeks and from 31% to 67% at 24 weeks.5 ,16 ,18
The proposed grey zone in France is 24–25 weeks. It is generally accepted that children born at 22–23 weeks should be provided with comfort care, whereas intensive care is routinely provided to babies born at or after 26 weeks of gestation. Recently available information promoting more individualised approaches may, however, encourage medical teams to consider factors other than gestational age in deciding on management.19–21
The aim of this study was to assess the French experience of delivery room management of extremely preterm infants based on Etude Epidémiologique sur les Petits Ages Gestationnels 2 (EPIPAGE-2), a recent cohort of very preterm births.
Patients and methods
Study population
The EPIPAGE-2 study is a population-based cohort study of preterm children born between 22 and 34 weeks of completed gestational age in France in 2011, including pregnancy terminations, stillbirths and live births.22
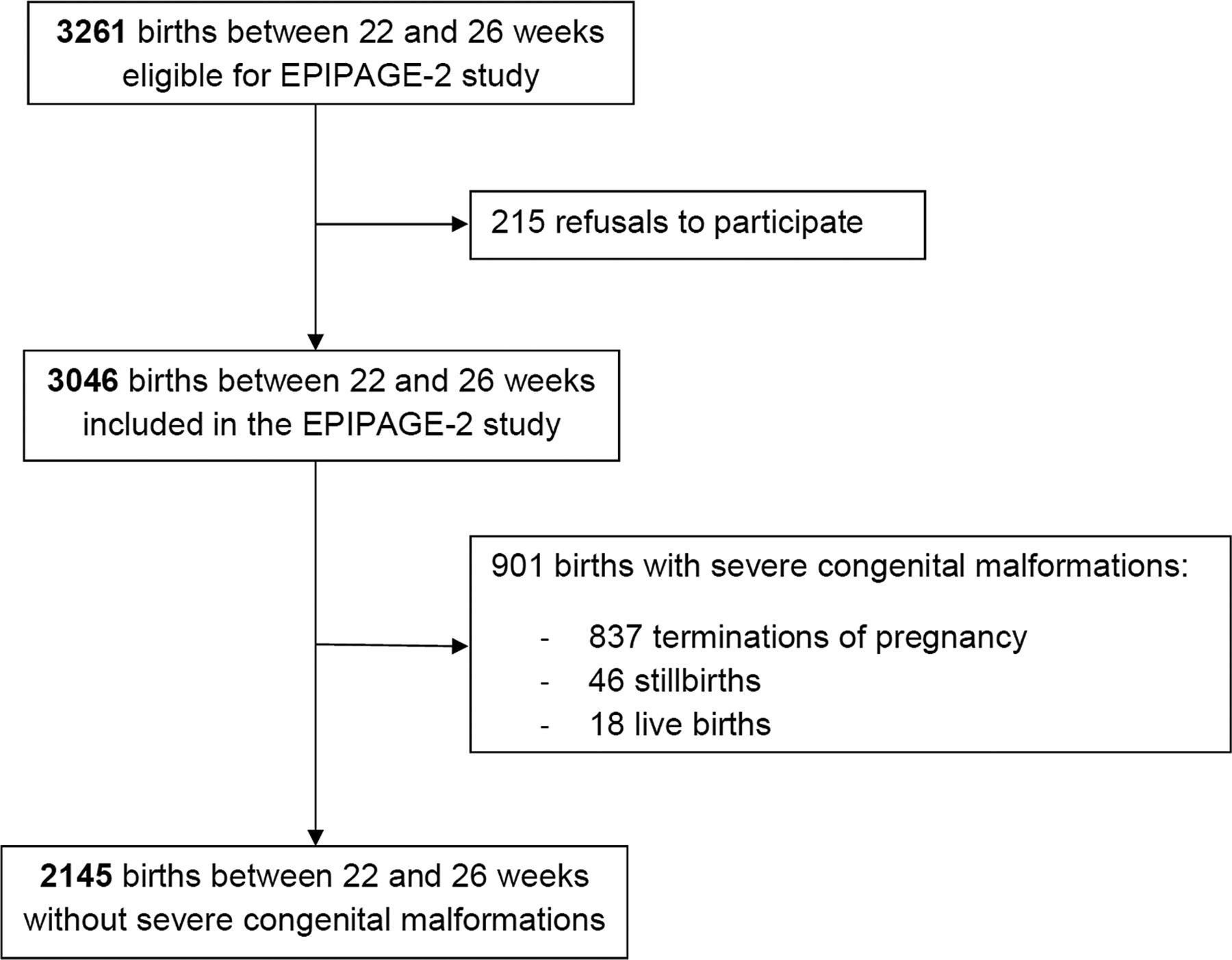
Our specific study included all births between 22 and 26 weeks of gestational age enrolled in the EPIPAGE-2 cohort without any severe congenital malformation (N=2145). Families received information and agreed to participate in the study before any data collection began.
Data collection
Data were collected at birth and during the neonatal hospitalisation, extracted from medical records kept in the maternity wards and neonatal units. We collected mothers’ socio-demographic and obstetric characteristics: age, country of birth, singleton or multiple pregnancy and any in vitro fertilisation treatment. The main causes of the preterm births were classified in one of four groups (preterm labour, preterm premature rupture of membranes, hypertensive disorder or placental abruption, and suspected fetal growth restriction at a prenatal ultrasound). Chorioamnionitis was defined as medically suspected chorioamnionitis within 48 h before birth. Data were also collected about antenatal corticosteroid administration, tocolysis, mode of delivery (caesarean or vaginal) and emergency delivery (time from admission to delivery <24 h).
Newborns’ characteristics were sex, birth weight (<600 g, 600–750 g, ≥750 g) and gestational age, defined in completed weeks of gestation and based on the last menstrual period and ultrasound assessment. We also had information on the life support and resuscitative measures performed at birth: oxygen therapy, nasal continuous positive airway pressure (nCPAP), endotracheal intubation, chest compressions and epinephrine administration. No intensive care was defined by a ‘no’ answer to each of these items. When ‘yes’ was answered to any of these items, we considered that the infant received intensive care.
We recorded the level of the hospital of birth (I, II or III). In France, level III maternity units are referral centres for the management of extremely preterm infants because they provide neonatal intensive care facilities.
Withholding or withdrawal of intensive care in the delivery room
The withholding/withdrawal of intensive care in the delivery room were assessed through the following dichotomous (yes/no) item in the questionnaire completed by the maternity unit staff: “Was intensive care withheld or withdrawn in the delivery room?” A ‘yes’ answer to this question could describe either the total absence of intensive care in the delivery room or the discontinuation of resuscitation. This response was cross-checked by examining the resuscitative measures performed according to the delivery room records.
Status at birth and mortality
We distinguished three different statuses at birth: terminations of pregnancy (none born alive), stillbirths and live births.
Statistical analysis
In the first step of analysis, we described status at birth and mortality rates according to gestational age and analysed perinatal care procedures and decisions to withhold or withdraw intensive care by gestational age.
Specific procedures were compared between the infants who had received intensive care and those for whom intensive care was withheld or withdrawn.
The second step consisted in identifying factors associated with the withholding/withdrawal of intensive care. These analyses were restricted to the live births between 24 and 26 weeks as almost no infants born at 22–23 weeks received intensive care. Using a two-level hierarchical logistic regression model, we investigated variations in the percentages of withholding/withdrawal of intensive care between maternity units, measured by the significance of the residual variance of the empty model.23 We then included individual factors in the model to examine whether they explained these variations. This approach enabled us to identify individual factors associated with the withholding/withdrawal of intensive care. To select the variables to be included in the multivariate models, we first used χ2 tests to study the associations between individual characteristics of mothers and children and the withholding/withdrawal of intensive care. This bivariate analysis identified variables for the multivariate model. We retained variables associated at a p <0.20 with withholding/withdrawal of intensive care, except those involving medical decisions (antenatal corticosteroid administration, tocolysis and mode of delivery) as these practice indicators could be a consequence rather than a cause or predictor of the intensive care decision.
All statistical tests were two-tailed, with p<0.05 defined as significant. Stata V.12.0 software was used for all analyses.
Results
Our population included 2145 births (figure 1). The proportion of live births increased from 13% at 22 weeks to 80% at 26 weeks. Among infants born alive at 22–23 weeks, more than 90% died in the delivery room, at 24 weeks, 40%, at 25 weeks, 8%, and at 26 weeks, 4%. No infant born at 22 weeks and only one born at 23 survived to discharge; this proportion was 31% at 24 weeks, 60% at 25 and 76% at 26 (table 1).
Status at birth and mortality rates by gestational age

{kind=link}
Flowchart of the study population.
Among the 249 deaths in the delivery room, 213 (86%) occurred after withholding/withdrawal of intensive care. Specific perinatal care procedures varied according to gestational age at birth (table 2). At 22 weeks, the rate of this withholding/withdrawal reached 96%. Only one (2%) of the infants born alive at 22 weeks received antenatal corticosteroids and four (7%) were born after caesarean deliveries. One (2%) received oxygen therapy and was intubated. At 23 weeks, intensive care was withheld or withdrawn for 91%. Ten (12%) received antenatal corticosteroids and 5% were born after a caesarean delivery. The percentages receiving oxygen therapy (14%), nCPAP (12%) and endotracheal intubation (9%) remained low. Almost 50% of infants at 22–23 weeks were born outside a level III maternity and with limited tocolysis.
Perinatal care procedures for extremely preterm infants born alive by gestational age
At 24 weeks, intensive care in the delivery room was withheld or withdrawn for 38%. Of the infants born alive at 24 weeks, 57% received antenatal corticosteroids and 14% were delivered by caesarean. Oxygen therapy was provided to 67%, nCPAP to 61% and 70% underwent endotracheal intubation.
At 25–26 weeks, intensive care was withheld or withdrawn for <10% of those born alive. More than 85% of the babies were born in a level III maternity unit, and almost 80% received antenatal corticosteroids. Caesareans were performed to deliver 34% of those born at 25 weeks and 60% of those born at 26 weeks. At 25 weeks, 89% of the babies born underwent endotracheal intubation and 93% at 26 weeks.
Most babies who died in the delivery room did so after intensive care was withheld, especially in the 22–24-week group. Resuscitation failure after intubation occurred in 9% at 24 weeks, 3% at 25 weeks and 2% at 26 weeks.
Overall, information on withholding/withdrawal of intensive care in the delivery room was available for 983 of the 1036 live births in the study (table 3). Among the 770 infants who received intensive care, 8 (1%) died in the delivery room versus 96% of those for whom intensive care was withheld/withdrawn.
Comparison of infants with intensive care and for whom intensive care was withheld or withdrawn for medical management and mortality rate (N=983 infants born alive between 22 and 26 weeks)
Of the 860 children born alive at 24–26 weeks, 99 (11.5%) had intensive care withheld or withdrawn in the delivery room. These children were born in 165 different maternity units: 85% in level III units, 12% level II and 3% level I.
Factors significantly associated with withholding/withdrawal of intensive care in the bivariate analysis were the absence of in vitro fertilisation, singleton pregnancy, chorioamnionitis, emergency delivery, low gestational age at birth and low birth weight (table 4).
Comparison of infants with intensive care and for whom intensive care was withheld or withdrawn according to social and medical characteristics (restricted to 860 infants born alive between 24 and 26 weeks)
After adjustment (table 5), factors independently associated with withholding/withdrawal of intensive care were extremely low gestational age at birth, birth weight <600 g, emergency delivery and singleton pregnancy.
Multilevel analysis (random intercept model) of factors associated with withholding or withdrawal of intensive care in the delivery room (N=860 infants and N=165 maternity units)
Rates of withholding/withdrawal of intensive care varied between maternity units from 0% to 100% and averaged 18.5% in level I maternity units, 20.0% in level II units and 10.0% in level III.
Multilevel model 1 showed a significant variation in the frequency of withholding/withdrawing of intensive care between maternity units. After adding gestational age to the model (model 2a), differences in the distribution of gestational ages between maternity units explained 77% of this variance. This figure did not change after including other individual variables (model 2b).
Discussion
This French population-based study showed that in 2011 most infants born before 24 weeks did not receive intensive care. Withholding/withdrawal of intensive care remained frequent at 24 weeks, but were rare at 25–26 weeks. Factors besides gestational age associated with this withholding/withdrawal were low birth weight, emergency delivery and singleton pregnancies.
The strength of our study lies in our specific cohort design: EPIPAGE-2 is one of the largest cohorts of very preterm births in Europe and reflects current medical practices in France.22 The large number of births included in this study ensured sufficient power and precision for estimations. This study analysed the current practical management of extremely preterm infants in delivery rooms in France for the first time and reported outcomes in all level I, II and III centres.
One potential limitation of our study comes from the variable of interest, assessed with the dichotomous (yes/no) question: “Was intensive care withheld or withdrawn in the delivery room?” We verified that this variable was reliable by cross-checking the answers with delivery room records for the use, non-use or discontinuing of any resuscitation measures (oxygen therapy, nCPAP, endotracheal intubation, chest compressions and epinephrine administration).
The survival rates to discharge are lower in France at 23, 24, 25 and 26 weeks than in Sweden, the USA, Japan or Australia.16 ,17 ,24 ,25 The rates in France at 23 and 24 weeks are also lower than in the UK.5
Our results suggest that the very low survival rates at 23–24 weeks in France compared with other countries are explained by the withholding/withdrawal of intensive care in the delivery room: almost no infant born before 24 weeks and 60% of those born at 24 weeks were admitted to NICUs. Therefore, the survival to discharge rate was zero before 24 weeks and 31% at 24 weeks. The proportion of stillbirths and live births appears to shift at around 24 weeks. This might be due to deliberate misclassification of some live births that were recorded as stillbirths since intensive care was not provided at 22, 23 or 24 weeks, but no data are available to support this hypothesis.
We also reported that most of the infants born alive at 25–26 weeks were admitted to the NICU (Neonatal Intensive Care Unit). Therefore, the lower survival rates at discharge at 25 and even 26 weeks in France compared with other countries cannot be explained by the withholding/withdrawal of intensive care in the delivery room. One explanation of better results in other countries could be that more frequent active management of extremely preterm infants can improve survival for those born at higher gestational ages (“getting better when treating more extremely preterm infants”). A pessimistic view of the prognosis for very preterm infants may also increase the rate of withdrawal of life-sustaining interventions in the NICU due to possible fears about immediate and long-term adverse outcomes. This may also explain our results at 24–26 weeks.
In France, the policy of not intervening before 24 weeks is partially based on the interpretation of the EPIPAGE 1 study, which reported no survival at gestational ages <24 weeks.2 Janvier and Mercurio provide a thoughtful analysis of the reasoning of perinatal teams faced with guidelines on management of extremely preterm infants.26 These policy statements often refer to low survival and high handicap rates to justify the withholding/withdrawal of intensive care and are often based on national data to justify their approach, thus creating a self-fulfilling prophecy.
Our aim was to assess the practices of delivery room management of extremely preterm infants in France. We believe that this is an important prerequisite for any consideration of practice or policy changes related to delivery room management of newborns in this gestational age range. However, our aim is not to propose new policy statements but rather to present the data. Only after extensive deliberation with neonatologists and obstetricians can we expect to change the French gestational age ‘grey zone’ or to do away completely with gestational age-based policies. To the extent possible, parents and other stakeholders should also be consulted in such decisions.27
Nevertheless, we do not believe that it is reasonable to take such important life-and-death decisions on gestational age alone. Moreover, we found that, at least at 24 weeks of gestation and above, gestational age was not the only factor associated with the decision to actively resuscitate or provide comfort care.
Birth weight <600 g was associated with higher rates of withheld or withdrawn intensive care after adjustment for gestational age. Medical teams may consider that infants who are small for gestational age at these extreme gestational ages have a less favourable outcome prognosis than those with appropriate size for gestational age.28 Emergency deliveries were also associated with a higher rate of withheld or withdrawn intensive care. These latter situations could be associated with a failure to administer antenatal corticosteroids or at least a full course, which might explain the association between emergency delivery and withholding/withdrawal of intensive care. However, one might reasonably have expected a lower rate of withheld or withdrawn intensive care in any case because in such situations it is sometimes difficult accurately to estimate gestational age or fetal weight and the capacity to discuss the management at birth in advance with the parents is limited.
Conclusion
This study analysed the current practical management of extremely preterm infants in delivery rooms in France for the first time. Gestational age was the primary factor influencing the withholding/withdrawal of intensive care but other factors included low birth weight, emergency delivery and singleton pregnancy. This study is a first step in deciphering the management of extremely preterm infants at birth in France, its ethical issues and the complexity of the decision-making process. Additional specifically designed studies would be very helpful for the development of national recommendations, which would help to improve the outcomes of these very fragile neonates.
Acknowledgments
The authors are grateful for the participation of all the families of extremely preterm infants in the EPIPAGE-2 cohort study and for the cooperation of all maternity units in France.
References
Footnotes
Collaborators EPIPAGE-2 Ethics Group: Pierre Kuhn; Bruno Langer; Nadia Mazille and Bénédicte Lecomte; Anne Bellot; Peggy Dupont-Chauvet; Pierre Betremieux; Alain Beuchée; Frédérique Charlot; Florence Rouget; Gérard Thiriez; Olivia Anselem; Elie Azria; Laurence Boujenah; Laurence Caeymaex; Pierre-Henri Jarreau; Jean-François Magny; Mostafa Mokhtari; Aurélien Jacquot; Anne Lemaître; Caroline Miler; Rachel Vieux; Catherine Arnaud; Patrick Truffert; Umberto Simeoni; Claude Bouderlique-Collin, Anne Chauty; Christophe Savagner; Olivier Claris; Anaëlle Coquelin.
Affiliations of the EPIPAGE-2 Ethics Group: University Hospital Strasbourg, France (Kuhn, Langer, Mazille); University Hospital Estaing, Clermont Ferrand, France (Lecomte); University Hospital Caen, France (Bellot, Dupont-Chauvet); University Hospital Rennes, France (Betremieux, Beuchée, Charlot, Rouget); Department of Neonatal Pediatrics, University Hospital Besançon, France (Thiriez); Department of Neonatal Pediatrics and Intensive Care, Cochin Hôtel Dieu Hospital, Paris, France (Anselem, Jarreau); Department of Obstetrics, Groupe Hospitalier Paris Saint Joseph, Paris Descartes University, Paris, France (Azria, Boujenah); Department of Neonatal Pediatrics and Intensive Care, CHI, CRC, Creteil, France (Caeymaex); Department of Neonatal Pediatrics and Intensive Care, Necker Enfants Malades University Hospital, Paris, France (Magny); Department of Neonatal Pediatrics and Intensive Care, Kremlin-Bicêtre University Hospital, Le Kremlin-Bicêtre, France (Mokhtari), Department of Neonatal Pediatrics and Intensive Care, Arnaud de Villeneuve Hospital, Montpellier, France (Jacquot, Lemaître); Department of Neonatal Pediatrics and Intensive Care, Adolphe Pinard Maternity Unit, Nancy, France (Miler, Vieux); UMR 1027 INSERM, Paul-Sabatier Toulouse III University, Toulouse, France (Arnaud); Department of Neonatal Pediatrics, Jeanne de Flandres Hospital, Lille, France (Truffert); Department of Neonatal Pediatrics and Intensive Care, La Conception Hospital, Marseille, France (Simeoni); Department of Neonatal Pediatrics and Intensive Care, Angers University Hospital, Angers, France (Bouderlique-Collin, Savagner); Department of Neonatal Medicine, Nantes, France (Chauty); Department of Neonatal Pediatrics and Intensive Care, University Hospital, Lyon, France (Claris), INSERM UMR 1153, Perinatal and Pediatric Epidemiology Team, Paris, France (Coquelin).
Funding This study was supported by a grant from the Fondation de France (http://www.fondationdefrance.org), which had no role in the design and conduct of the study, the collection, analysis or interpretation of data or writing of the report.
Competing interests None declared.
Ethics approval National Data Protection Authority (CNIL no. 911009) and Consultative Committee on the Treatment of Information on Personal Health for Research Purposes (no. 10.626) and Committee for the Protection of People Participating in Biomedical Research (n) CPP SC-2873).
Provenance and peer review Not commissioned; externally peer reviewed.