Article Text

Abstract
Objective At birth, an initial sustained inflation (SI) uniformly aerates the lungs, increases arterial oxygenation and rapidly improves circulatory recovery in asphyxiated newborns. We hypothesised that lung aeration, in the absence of an increase in arterial oxygenation, can increase heart rate (HR) in asphyxiated near-term lambs.
Interventions Lambs were delivered and instrumented at 139±2 days of gestation. Asphyxia was induced by umbilical cord clamping and then delaying the onset of ventilation until mean carotid arterial pressures (CAPs) had decreased <20 mm Hg. Lambs then received a single 30-s SI using nitrogen (N2; n=6), 5% oxygen (O2; n=6), 21% O2 (n=6) or 100% O2 (n=6) followed by ventilation in air for 30 min.
Main outcome measures HR, CAP and pulmonary blood flow (PBF) were continuously recorded.
Results HR and PBF increased more quickly in lambs resuscitated with 100% and 21% O2 than with 5% O2 or N2. HR and PBF recovery in the 5% O2 group was delayed relative to all other oxygen SI groups. HR in 5%, 21% and 100% O2 groups reached 100 bpm before the SI was complete. HR and PBF in the N2 group did not increase until 10 s after the SI was completed and ventilation was initiated with air. CAP tended to increase quicker in all O2 groups than in N2 group.
Conclusions Oxygen content during an SI is important for circulatory recovery in asphyxiated lambs. This increase in HR is likely driven by the increase in PBF and venous return to the heart.
- Neonatology
- Resuscitation
- Animal Research
Statistics from Altmetric.com
What is already known on this topic?
An initial sustained inflation (SI) has been shown to facilitate airway liquid clearance at birth leading to a greater functional residual capacity and tidal volume recruitment and a more uniform distribution of ventilation in animal models.
An initial 30 s SI rapidly increases heart rate, blood pressure, arterial oxygenation and rate of increase in pulmonary blood flow in severely asphyxiated, bradycardic newborn lambs, although the mechanism for the rapid increase in heart rate is unknown.
What this study adds?
The oxygen content of gas used to inflate the lungs during an initial SI is required for cardiopulmonary circulatory recovery in asphyxiated near-term lambs.
Following asphyxia, an SI using as little as 5% oxygen concentration was enough to improve the cardiovascular transition after birth, resulting in a more rapid recovery in heart rate and blood pressure than conventional ventilation with air.
Introduction
Asphyxiated newborn infants that are bradycardic and apnoeic at birth require urgent resuscitation, most commonly in the form of assisted ventilation. As these infants have liquid-filled lungs, the airways must be cleared of liquid to establish pulmonary gas exchange and restore spontaneous circulation.1 ,2 Currently, there is no globally accepted strategy for the resuscitation of asphyxiated newborn infants.
An initial sustained inflation (SI) has been shown to facilitate airway liquid clearance at birth leading to a greater functional residual capacity and tidal volume recruitment and a more uniform distribution of ventilation.3 By increasing the time course over which the inflating pressure is applied, an SI more efficiently moves lung liquid through the airways, into the distal air sacs and then into the surrounding interstitial tissue. By facilitating lung aeration, an initial SI also improves arterial oxygenation and increases the rate of increase in pulmonary blood flow (PBF) at birth.4 Similarly, an SI improves heart rate (HR) and cerebral tissue oxygen saturation in very low birthweight infants.5
An initial 30 s SI also rapidly increases HR and blood pressure in severely asphyxiated, bradycardic newborn lambs4 although the mechanism for the rapid increase in HR is unknown. The most logical explanation is the resupply of oxygenation to the myocardium, although the speed of the response (4–8 s) suggests the involvement of additional mechanisms. For instance, a more rapid increase in PBF, which increases pulmonary venous return and left atrial filling may contribute to the increase in HR by increasing left ventricular preload.
At birth, the entry of air into the lungs triggers a large decrease (up to 70%) in pulmonary vascular resistance (PVR) and a marked increase in PBF.6 Although increased oxygenation is a contributing factor, numerous studies have shown that lung aeration can trigger an increase in PBF without altering arterial oxygenation levels. Furthermore, it has been shown that the oxygen concentration of the inflating gas only affects the magnitude of the increase in PBF.7 ,8 As such, it is possible that the entry of gas into the airways alone, irrespective of the oxygen concentration, is enough to trigger the increase in PBF and restore cardiac function in severely asphyxic, bradycardic newborns.
Our aim was to determine how the oxygen concentration of the inflation gas influences the restoration of cardiac function in severely asphyxiated bradycardic newborn lambs. We investigated the cardiopulmonary responses to aerating the lungs with 100% nitrogen (0% oxygen) or increasing oxygen concentrations (5%, 21% or 100%) during an initial SI following severe asphyxia. We hypothesised that aerating the lungs without altering arterial oxygenation is enough to trigger the cardiopulmonary transition and increase HR in asphyxiated near-term lambs.
Methods
All experimental procedures were approved by the relevant Monash University Animal Ethics Committee in accordance with the National Health and Medical Research Council (Australia) Australian code of practice for the care and use of animals for scientific purposes (7th Edition, 2004). Pregnant ewes at 139±1.2 (mean±SD) days of gestation (term is ∼147 days) were anesthetised with 5% sodium thiopentone (20 mL; pentothal 5 mg/mL) and maintained using 0.5%–4% isoflurane. A hysterotomy was performed to expose the fetal head and neck, occlusive polyvinyl catheters were inserted into a fetal carotid artery and jugular vein and an ultrasonic flow probe (3 mm; Transonic Systems, Ithaca, New York, USA) was placed around the non-catheterised carotid artery. The fetal chest was exposed, and an ultrasonic flow probe was placed around the left main pulmonary artery via a thoracotomy, as previously described.9 The fetal trachea was intubated with a cuffed endotracheal tube (ID 5 mm, OD 6.8 mm, Portex, Kent, England) and lung liquid was drained passively for about 20 s. A transcutaneous oximeter (Masimo, Irvine, California, USA) was attached around the right forelimb for measurement of oxygen saturation. The umbilical cord was clamped and cut, lambs were delivered, dried, weighed and placed under an infant warmer (Fisher & Paykel Healthcare, Auckland, New Zealand). After delivery, asphyxia was induced by delaying ventilation onset until after the mean carotid arterial pressure had decreased <20 mm Hg. Throughout the experiment, lambs were lightly sedated by infusion of a sedative (alfaxane intravenous 5–15 mg/kg/h; Jurox, East Tamaki, Auckland, New Zealand in 5% glucose). Ewes were humanely killed (sodium pentobarbitone ∼100 mg/kg, intravenous lethobarb 324 mg/mL; Virbac, New South Wales, Australia) after delivery of the lamb.
Carotid arterial blood flow (CBF) and PBF (Powerlab; ADInstruments, Castle Hill, New South Wales, Australia) and carotid arterial pressure (CAP; DTX Plus Transducer; Becton Dickinson, Singapore) were recorded continuously prior to delivery and until the end of the experiment. Following the asphyxia period, lambs were randomly assigned to receive a 30 s SI using either 100% nitrogen (0% oxygen; N2; n=6) to investigate the effect of aerating the lungs without altering oxygenation levels or using different oxygen concentrations of 5% (5% O2; n=6), 21% (21% O2; n=6) and 100% (100% O2; n=6; figure 1). The SI was delivered by a T-piece device (Neopuff; Fisher & Paykel Healthcare, Panmure, Auckland, New Zealand) with a peak inspiratory pressure (PIP) of 35 cm H2O. Following the SI, all lambs received positive pressure ventilation (Babylog 8000+ventilator; Drager, Lubeck, Germany) and ventilated using a set tidal volume of 8 mL/kg for 30 min (PIP 35 cm H2O, positive end expiratory pressure (PEEP) 5 cm H2O, inspiratory time 0.5 s and expiratory time 0.5 s) in air (21% oxygen). Tidal volume (VT) and airway pressure were recorded continuously during the ventilation procedure (Powerlab, ADInstruments).

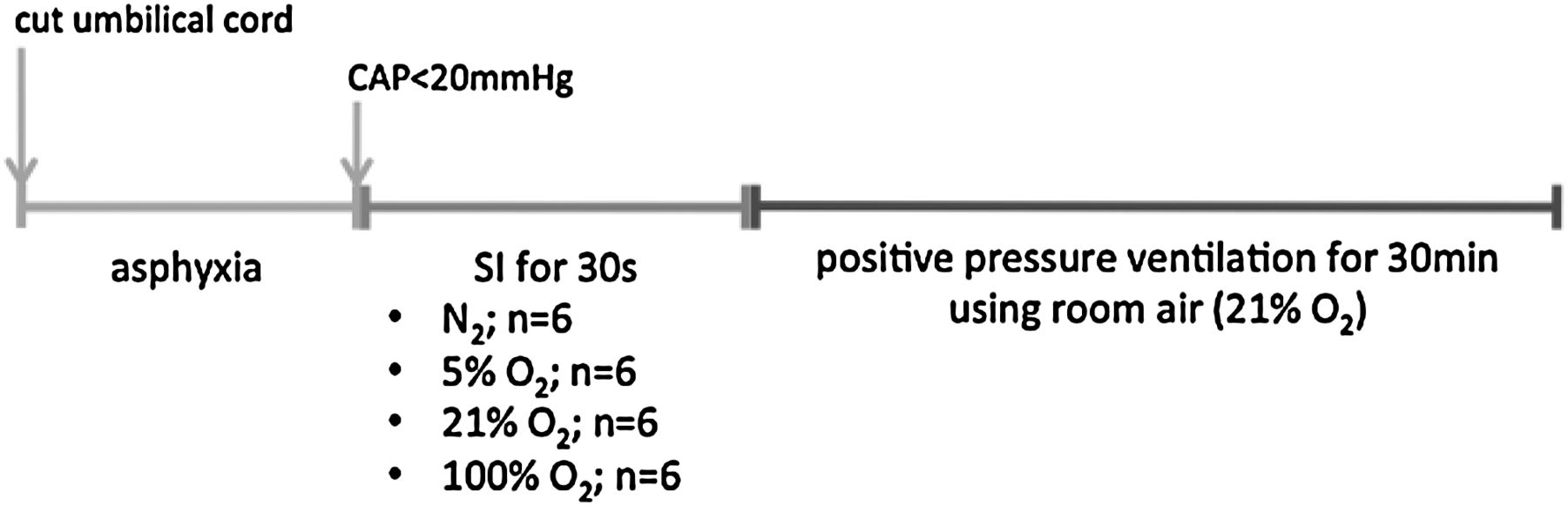
Diagram of the experimental timeline. Following the fetal surgery, the umbilical cord was clamped and cut and lambs were delivered. After delivery, asphyxia was induced by delaying ventilation onset until after the mean carotid arterial pressure (CAP) had decreased <20 mm Hg. Following the asphyxia period, lambs received a 30 s SI using either 100% nitrogen (0% oxygen; N2; n=6) or using different oxygen concentrations of 5% (5% O2; n=6), 21% (21% O2; n=6) and 100% (100% O2; n=6). Following the SI, all lambs received positive pressure ventilation in air (21% oxygen) for 30 min. SI, sustained inflation.
Arterial blood samples were taken at 1, 5, 7.5, 10, 15, 20 and 30 min after the onset of ventilation and measured for arterial partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), pH and arterial oxygen saturation (SaO2; ABL30, Radiometer, Copenhagen, Denmark).
Analytical methods
Mean HR, CAP, PBF and CBF were averaged over 5 s epochs every minute for the first 5 min after initiation of the SI. Epochs were then averaged at 10, 15, 20, 25 and 30 min. Carotid arterial pulsatility index (CaPI), a measure of downstream resistance to blood flow,10 was calculated as
End-diastolic PBF was averaged from five consecutive cardiac cycles at these same epochs. Vt, PIP and lung compliance (LC) were averaged over 1 min epochs 1, 5, 10, 20 and 30 min after SI onset. LC was calculated as:
Carotid arterial blood oxygen content from arterial blood gases was measured to estimate cerebral oxygen delivery11 and cerebral O2 extraction,12 according to the formulas:
where
In addition, to identify changes during and immediately after the SI, average values of HR, CAP, PBF and CBF were calculated every 10 s for the first 2 min of ventilation.
Statistical methods
Physiological data were analysed using 2-way repeated measures analysis of variance with group (30 s using N2 and 100% O2, 21% O2 and 5% O2) and time as factors. Post hoc comparisons between groups and time-points were performed using the Holm–Sidak test. Data are presented as mean±SEM unless otherwise stated. Statistical difference was defined as p<0.05.
Results
There were no differences in HR, blood pressure or oxygen saturation before cord occlusion between the groups. However, pH was slightly lower in the 5% O2 SI lambs (7.2±0.1 compared with 7.3±0.1 in the other groups) and base excess was higher in the 21% O2 SI lambs (−0.5±2.0 compared with −2.9±2.0, −6.2±3.5 and −4.6±2.0 in the N2, 5% and 100% O2 SI lambs, respectively) before cord occlusion. The mean duration (10–13 min) of asphyxia was similar between all groups (table 1). At the completion of the asphyxia period, lamb HR, mean CAP and arterial blood gases were not different between groups (table 1).
Characteristics at onset of ventilation
HR increased early and rapidly in 21% and 100% O2 SI lambs, increasing above baseline (ie, before ventilation onset) within 10 s after SI onset (figure 2A). Similarly, although not as rapid, HR increased in 5% O2 SI lambs before the end of the SI, reaching a mean of 122±9.6 bpm by the end of the 30 s SI. HR in N2 SI lambs did not increase during the SI and only increased above baseline during the subsequent ventilation period at 50 s after SI onset, that is, at 20 s after completion of the SI. By 2 min, HR was not different between groups (figure 2B).
Mean PBF did not increase above baseline values in N2 SI lambs until lambs were ventilated with air, ∼1 min after SI onset. Mean PBF increased with the onset of SI in all O2 SI lambs, although PBF increased more rapidly in 21% O2 and 100% SI lambs compared with 5% SI lambs (figure 3A). During the ventilation period following the SI, end-diastolic PBF increased above baseline measurements in 100% O2 and N2 SI lambs before 5% and 21% O2 SI lambs (figure 3C). However, end-diastolic PBF did not increase in N2 SI lambs until after the lambs received 21% oxygen. Mean or end-diastolic PBF did not differ between groups after 10 min of ventilation (figure 3B, D).

Heart rate (HR) from 1 to 2 min (A) and 0 to 30 min (B) in lambs receiving a single 30 s sustained inflation (SI) using nitrogen (30 s SI N2; ○) or using different oxygen concentrations of 5% (30 s SI 5% O2; •), 21% (30 s SI 21% O2; ▪) or 100% (30 s SI 100% O2; ▴) before the onset of ventilation (BV) and with the initiation of ventilation (designated as time 0). Data are mean (SEM). +p<0.05 vs BV time point for N2 SI. γp<0.05 vs BV time point for 5% O2 SI. #p<0.05 vs BV time point for 21% O2 SI. *p<0.05 vs BV time point for 100% O2 SI.
Mean CAP increased similarly in 21% and 100% O2 SI lambs 30 s after SI onset, although the increase appeared to be more rapid in 100% O2 SI lambs (figure 4A). Mean CAP increased in 5% O2 SI lambs 60 s after SI onset. CAP did not increase in N2 lambs until 90 s after SI onset and, therefore only increased after the lambs were ventilated in air. Following the SI, CAP continued to increase more rapidly in 100% SI lambs compared with the other groups. CAP did not differ between groups at 5 min after ventilation onset (figure 4B).

Mean pulmonary blood flow (PBF) and end-diastolic PBF 1 to 2 min (A, C) and 0 to 30 min (B, D) in lambs receiving a single 30 s sustained inflation (SI) using nitrogen (30 s SI N2; ○) or using different oxygen concentrations of 5% (30 s SI 5% O2; •), 21% (30 s SI 21% O2; ▪) or 100% (30 s SI 100% O2; ▴) before the onset of ventilation (BV) and with the initiation of ventilation (designated as time 0). Data are mean (SEM). +p<0.05 vs BV time point for N2 SI. γp<0.05 vs BV time point for 5% O2 SI. #p<0.05 vs BV time point for 21% O2 SI. *p<0.05 vs BV time point for 100% O2 SI.
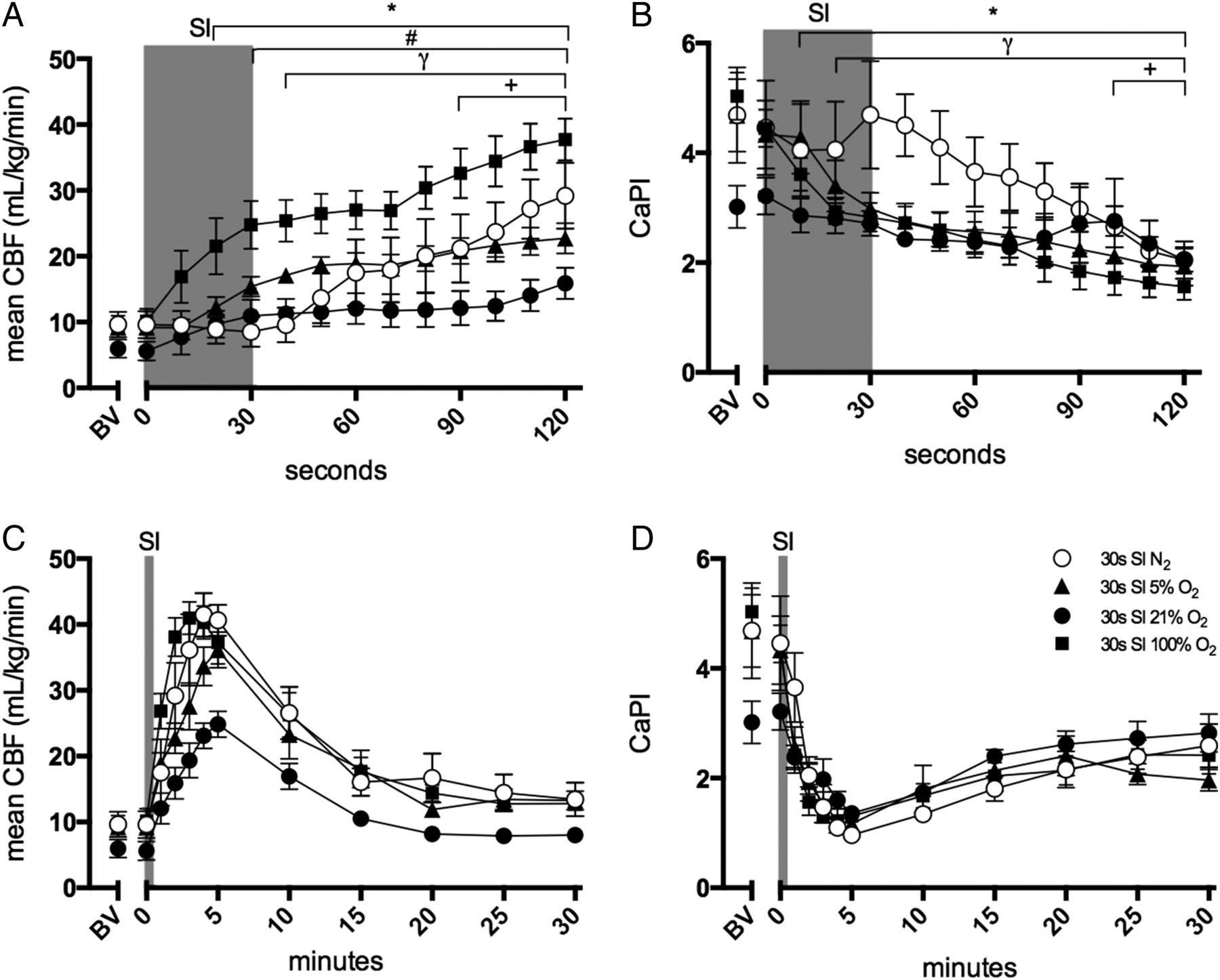
The increase in mean CBF was greatest in 100% O2 SI lambs (figure 5A) and it commenced rapidly following the SI onset. Although CBF also increased rapidly in N2 SI lambs this did not occur until after the SI was completed (∼45 s after SI onset), when the lambs were being ventilated in air. In all groups, the increase in CBF peaked after 5 min of ventilation before decreasing. After 5 min of ventilation, CBF tended to be lower (by 5–10 mL/kg/min) in 21% O2 lambs compared with the other groups; however, this was not statistically significant (figure 5B). CaPI was lower in 21% O2 lambs than in 100% O2 lambs at the end of the asphyxia period, immediately before onset of the SI (figure 5C). In N2 SI lambs immediately following the SI, CaPI transiently increased before decreasing to values that were similar the other groups 1 min after ventilation onset (figure 5D). Cerebral oxygen delivery was higher in 100% O2 SI lambs, compared with all other groups, at 1 min after ventilation (figure 6). In all groups, cerebral oxygen delivery increased after ventilation onset, peaking at 5 min before decreasing again (figure 6). Cerebral oxygen delivery did not differ between groups at 5 min after ventilation onset.
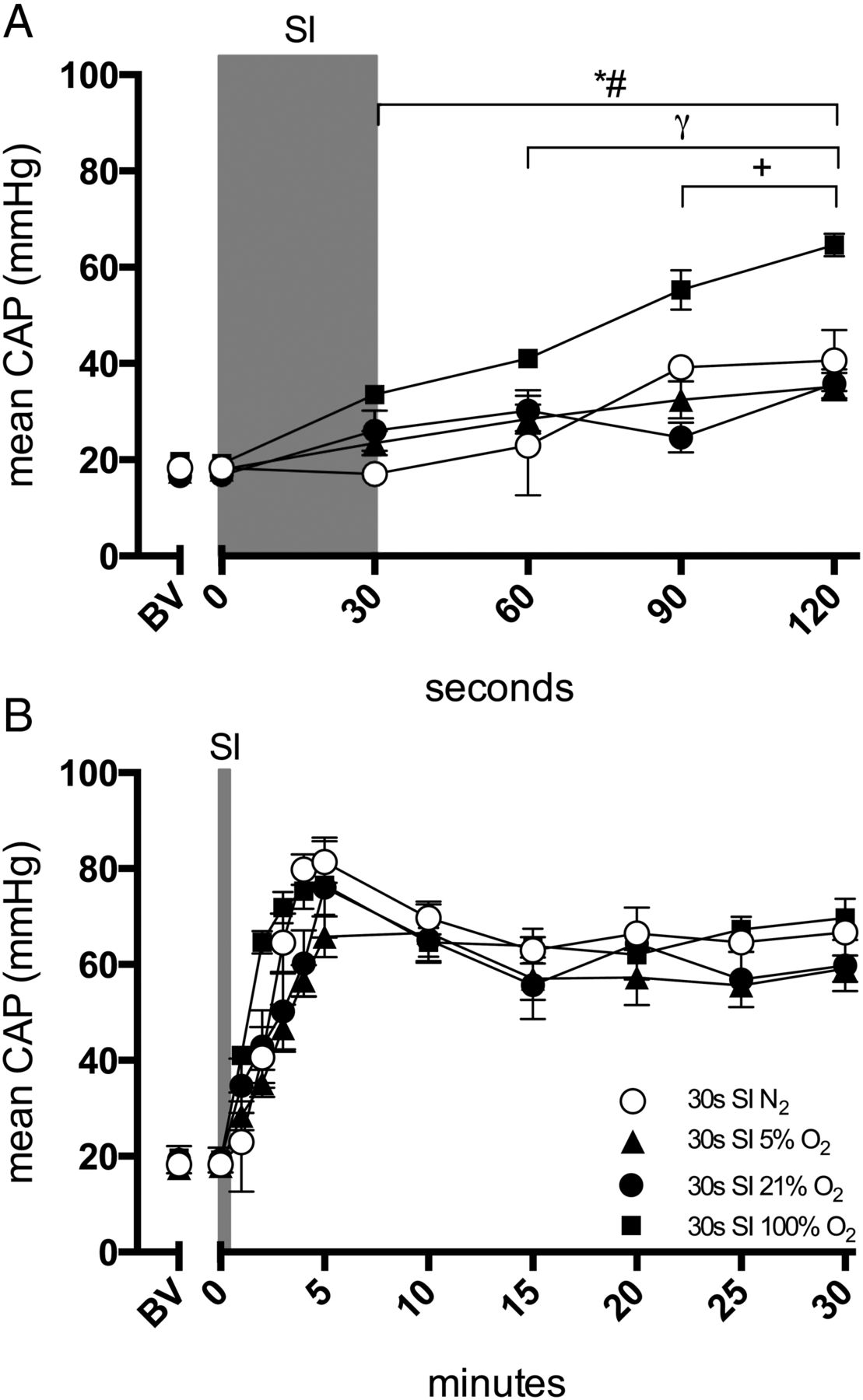
Mean carotid arterial blood pressure (CAP) 1–2 min (A) and 0–30 min (B) in lambs receiving a single 30 s sustained inflation (SI) using nitrogen (30 s SI N2; ○) or using different oxygen concentrations of 5% (30 s SI 5% O2; •), 21% (30 s SI 21% O2; ▪) or 100% (30 s SI 100% O2; ▴) before the onset of ventilation (BV) and with the initiation of ventilation (designated as time 0). Data are mean (SEM). +p<0.05 vs BV time point for N2 SI. γp<0.05 vs BV time point for 5% O2 SI. #p<0.05 vs BV time point for 21% O2 SI. *p<0.05 vs BV time point for 100% O2 SI.

Mean carotid arterial blood flow (CBF) and carotid arterial pulsatility index (CaPI) 1–2 min (A, C) and 0–30 min (B, D) in lambs receiving a single 30 s sustained inflation (SI) using nitrogen (30 s SI N2; ○) or using different oxygen concentrations of 5% (30 s SI 5% O2; •), 21% (30 s SI 21% O2; ▪) or 100% (30 s SI 100% O2; ▴) before the onset of ventilation (BV) and with the initiation of ventilation (designated as time 0). Data are mean (SEM). +p<0.05 vs BV time point for N2 SI. γp<0.05 vs BV time point for 5% O2 SI. #p<0.05 vs BV time point for 21% O2 SI. *p<0.05 vs BV time point for 100% O2 SI.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cerebral oxygen delivery in lambs receiving a single 30 s sustained inflation (SI) using nitrogen (30 s SI N2; ○) or using different oxygen concentrations of 5% (30 s SI 5% O2; •), 21% (30 s SI 21% O2; ▪) or 100% (30 s SI 100% O2; ▴) before the onset of ventilation (BV) and with the initiation of ventilation (designated as time 0). Data are mean (SEM).
All groups achieved the target VT of 8 mL/kg within 1–2 min of tidal ventilation onset. During the ventilation period, no differences were found in VT, PIP or dynamic LC or arterial blood gases between the groups throughout the tidal ventilation period. Similarly, AaDO2, PaCO2, PaO2 and SaO2 were not different between groups.
Discussion
We have previously demonstrated that asphyxiated, bradycardic newborn lambs given a 30 s SI had an earlier and more rapid recovery in HR compared with lambs given five consecutive 3 s SIs or conventional ventilation.13 The aim of this study was to determine whether this rapid recovery in HR in response to a 30 s SI results from better aeration of the lungs, with or without improved oxygenation. The findings of this study show that a 30 s SI administered to asphyxiated, bradycardic lambs did not increase HR or PBF, unless O2 was present in the gas mixture; these parameters only increased after the lambs were ventilated in air. While increasing the O2 content to 5% and then 21% significantly improved the HR recovery at each concentration, no further improvement was found by increasing the O2 to 100%.
The initiation of the SI with O2 present in the gas mixture resulted in an increase in PBF, CAP and CBF irrespective of the O2 content. The increase in HR, PBF and CAP was more rapid in lambs that received 21% and 100% O2, compared with those that received 5% O2. Interestingly, no difference in the rate of increase in HR, PBF or CAP was observed between 21% and 100% O2 SI groups, although the CAP tended to be greater at the end of the SI in lambs receiving 100% O2. However, CBF was significantly higher in lambs receiving 100% O2 at 1 min after SI onset, despite those lambs tending to be better oxygenated. Better oxygenation would normally result in a reduction in CBF, perhaps indicating that immediately following a severe asphyxic episode, the cerebral circulation is so vasodilated that it is mostly pressure passive and largely insensitive to arterial oxygen levels. As such, this may greatly increase the risk of hyperoxia-induced brain injury.
The extent of oxygen supplementation during newborn resuscitation remains controversial. Our finding that the initial increase in PBF and HR was similar between 21% and 100% O2 SI groups is consistent with previous studies14–16 that show newborns can be resuscitated just as efficiently with air as with 100% O2. As ventilation with 100% oxygen, particularly following asphyxia, is associated increased upregulation of inflammatory cytokines, oxidative stress and pulmonary vascular reactivity, high oxygenation levels should be avoided.17–21 Tissue and blood samples were not collected to detect injury in this study.
As techniques such as an SI can aerate the lungs and increase arterial oxygenation, they may reduce the need for supplemental oxygen in the delivery room. A randomised, controlled trial has found that infants given a SI (following by nasal continuous positive airway pressure) required less intubation, mechanical ventilation and developed less bronchopulmonary dysplasia (BPD), compared with infants receiving bag and mask ventilation without PEEP.22 Similar findings have been reported in another randomised trial and two retrospective studies.23–25 The neonates that were given a SI were less likely to need mechanical ventilation and develop BPD and require shorter periods of oxygen therapy. Similarly, very low birthweight infants showed increased HRs and cerebral tissue oxygenation following an effective SI.5
In lambs that received N2 (0% O2), PBF remained low throughout the entire SI, whereas in each of the other groups it tended to increase. The finding that PBF only increased in N2 SI lambs after they were ventilated in air indicates that oxygen is a key component of the increase in PBF, HR and CAP in the immediate postasphyxiated period. This is likely to result from a direct effect of increasing oxygen levels on both the myocardium and the pulmonary vasculature. While an oxygen-induced increase in myocardial contractility from a near asystolic state is essential for the increase in PBF, the decrease in PVR is also a major contributor to the increase in cardiac output at birth by increasing PBF. This results in an increase in pulmonary venous return and the restoration of ventricular preload lost upon umbilical cord clamping.26 ,27 Thus, the increase in cardiac output (indicated by increase in HR and CAP) and the increase in PBF following severe asphyxia are interdependent, with each relying very much on the other. While we found that minimum diastolic PBF (which is usually an indicator of PVR) was higher in 100% O2 lambs at 2 min after SI onset, this was likely due to a high systemic arterial pressure (CAP) affecting flow through the ductus arteriosus in these lambs. However, it is interesting that the PBF, minimum diastolic PBF and end-diastolic PBF were all similar at 1 and 2 min after SI onset, despite having very different oxygenation levels. This suggests that the effect of O2 concentration on HR recovery was mostly due to an effect on the myocardium.
CaPI decreased with the onset of a SI with oxygen, irrespective of the O2 concentration, which indicates a decrease in cerebral vascular resistance,10 resulting in increased CBF. As hypoxia and hypercapnia are potent cerebral vasodilators, the cerebral vasculature within these lambs would likely have been maximally dilated in response to the asphyxia.28 This autoregulatory response is designed to sustain blood flow and oxygen delivery to the brain.28 In addition to these autoregulatory mechanisms, another compensatory response to acute reductions in cerebral oxygen delivery is increased oxygen extraction. Over the first 5 min following ventilation onset, cerebral oxygen delivery increased 6-fold due to both an increase in oxygen content and an increase in CBF. However, this was followed by a reduction in CBF, which is a compensatory mechanism to autoregulate cerebral oxygen delivery. Following an initial asphyxic insult, rapid cerebral reperfusion and increases in blood oxygen content expose the brain to an increased risk of oxidative stress, blood–brain barrier permeability and haemorrhage.29 ,30 This was likely to be exacerbated in lambs that received 100% O2, as they had a more rapid and greater increase in mean CBF within the first 2 min, resulting in greater oxygen delivery to brain. In contrast, those lambs that received 21% O2 had a reduced peak CBF and a more gradual reduction to CaPI, suggesting a greater capacity to autoregulate cerebral oxygen delivery within physiological ranges.
As sustained increases in intrathoracic pressure are known to increase PVR, thereby reducing venous return and cardiac output,31 there is some concern that a SI will impede the cardiovascular transition at birth. However, a previous study in preterm lambs has shown that a SI of 40 cm H2O did not impede and tended to enhance the increase in PBF immediately after birth.4 This study further highlights that a SI of 35 cm H2O does not impede the pulmonary transition at birth as PBF and HR increased during the SI when oxygen was used, regardless of concentration. As the increase in PBF and HR was delayed in 5% O2 SI lambs, compared with 100% and 21% O2 SI lambs, oxygenation status influences the magnitude of increase. However, it is interesting that the increase in HR and CAP measured in N2 lambs was greater than we observed in our previous studies in lambs that were resuscitated in air (21% O2) with conventional ventilation.13 We consider that this is due to the much greater ability of a SI to aerate the lung. As such, the SI with N2 must have effectively cleared the distal airways of liquid allowing a more rapid penetration of oxygen into the distal gas exchange units following the onset of ventilation with air.
Several studies have demonstrated that ventilating fetal sheep with nitrogen decreases PVR and increases PBF.7 ,8 ,32 ,33 Based on these observations, it was hypothesised that expansion of newborn lungs by gas is enough to decrease PVR and that oxygen and carbon dioxide content of the gas only influences the magnitude of the decrease in PVR.32 ,33 However, as explained above, it is not surprising that we did not observe an increase in PBF during a SI using nitrogen in asphyxiated lambs. This is because in our study the lambs were severely asphyxiated, and as a result, myocardial function was reduced as indicated by a low CAP (<20 mm Hg). In this instance, as an increase in PBF is also dependent upon restoring myocardial contractility, not just a decrease in PVR, it is not surprising that an SI using N2 failed to stimulate an increase in PBF. However, as 5% O2 was able to initiate both an increase in PBF and an increase in CAP, only a small increase in oxygenation is required.
In summary, we found that oxygen content of gas used to inflate the lungs during an initial SI is required for cardiopulmonary circulatory recovery in asphyxiated near-term lambs. We also found that following asphyxia, an SI using as little as 5% oxygen concentration was enough to improve the cardiovascular transition after birth, resulting in a more rapid recovery in HR and CAP than conventional ventilation with air. This study provides a novel insight into the complex mechanisms involved in the respiratory and circulatory transition at birth.
Acknowledgments
We thank Ms. Karyn Rodgers for her assistance with these experiments.
References
Footnotes
Contributors KSS participated in the study design, collected the data, analysed the data, reviewed the literature and wrote a first draft. TO, GRP, KJC and TJMM participated in study design, collected data and edited the manuscript. SBH participated in the study design and coordination, collected and analysed data and edited the manuscript.
Funding This work was supported by the National Health and Medical Research Council (NHMRC) of Australia program grant (No. 384100), fellowship (GRP: 1026890, TJM: APP1043294, SBH: 545921), a Rebecca L. Cooper Medical Research Foundation Fellowship (GRP) and the Victorian Government’s Operational Infrastructure Support Program.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms