Article Text

Abstract
Aims To study the incidence and treatment of retinopathy of prematurity (ROP) in England, 1990–2011.
Methods English national Hospital Episode Statistics were analysed, for babies born in hospital and for inpatient admissions, to obtain annual rates of diagnosis of, and treatment for, babies with ROP. National data on low birthweight (LBW) babies, born <1500 g and therefore eligible for ROP screening, were used as denominators in calculating rates of ROP per 1000 babies at risk.
Results The recorded incidence of ROP increased tenfold, from 12.8 per 1000 LBW babies in 1990 to 125.5 per 1000 LBW babies in 2011. Tretment rates for ROP by cryotherapy or laser rose from 1.7 to 14.8 per 1000 LBW babies between 1990 and 2011. In 1990, 13.3% of babies with ROP were treated with cryotherapy, which fell to 0.1% in 2011. Rates for laser treatment rose from 1.8% of babies with ROP in 1999 to 11.7% in 2011.
Conclusions Increased neonatal survival, improved awareness of ROP and dissemination of guidance on screening and treatment of ROP will all have contributed to the substantial rise in recorded incidence of ROP between 1990 and 2011. Retinal ablation is now almost always performed using laser treatment rather than cryotherapy.
- Child health (paediatrics)
- Retina
- Epidemiology
Statistics from Altmetric.com
Introduction
Retinopathy of prematurity (ROP) is a vasoproliferative disease of immature retina. The end stages of the disease were first reported in 1942 and named retrolental fibroplasia but, with increasing knowledge, renamed ROP. Its pathogenesis is multifactorial, but high oxygen saturation levels in the preterm infant are key. In a preterm infant, the relative hyperoxia (compared with intrauterine relative hypoxia) prevents retinal vascular development. The subsequent ischaemia stimulates increased production of vascular endothelial growth factor (VEGF).1 Unregulated retinal neovascularisation occurs. The pathogenesis of ROP is more complex than the VEGF theory alone; both maternal and foetal factors play a role. ROP is therefore associated with sick neonates.2
The International Classification of ROP was first published in 1984 to support standardised recording of clinical signs.3 The Cryotherapy for ROP (CRYO-ROP) study showed that ablation of ischaemic retina improves both structural and functional outcomes.4 Since then, clinicians have been obliged to screen babies at risk and treat as per published guidelines. In the UK, screening began after the Royal College of Ophthalmologists (RCOphth) and British Association for Perinatal Medicine published guidelines in 1990.5 ,6 The guidelines were updated in 1996.7 UK practice was audited showing that the great majority of neonatal units performed screening, although variations existed regarding treatment.8 As a result, in 2008, the guideline was rewritten in collaboration with the Royal College of Paediatrics and Child Health (RCPCH) and Bliss (the premature baby charity).9
Prior to 2003, and on the basis of CRYO-ROP, babies with threshold ROP were treated in both eyes. Threshold ROP is defined as five continuous, or eight cumulative, clock hours of stage 3 ROP in zone 1 or 2, with plus disease. Since the Early Treatment of ROP (ET-ROP) study in 2003, babies with pre-threshold ROP were also treated.10 Pre-threshold ROP includes plus disease found in zone 1, stage 3 ROP in zone 1, and stage 2 or 3 ROP with plus disease in zone 2. Treatment of ROP is determined by disease severity; therefore, treatment incidence can be used as a marker of severity. This is not a simple relationship as the definition of disease requiring treatment changed with the publication of ET-ROP.
There is conflicting evidence on the trend of incidence of severe ROP in the UK.11–13 This study aimed to examine trends in incidence of ROP, its treatment and the underlying population at risk of ROP in England, using health service use and demographic data.
Methods
Study population
Routinely collected statistical records of babies under 1 year of age, in hospital in England between 1990 and 2011, were studied using Hospital Episode Statistics (HES). HES was analysed, specifically for this study, to identify records with a diagnosis of any stage of ROP, treatment of ROP with cryotherapy and treatment of ROP by laser.
Dataset
HES is the routine administrative dataset that includes statistical information about all National Health Service inpatient events, including babies born in hospital and admissions for day case care, from all hospitals in England. HES data were provided, as individual-level records of episodes of care, by the Health and Social Care Information Centre (it was not able to provide HES data for 2012 and 2013). The first full calendar year of data collection was 1990. From 1990 to 1998, the only available data in HES were built around ‘episodes’ of care, in which each period of care of each patient by an individual doctor is counted, but from which the number of individuals in receipt of care cannot be determined. From 1999, the data were linkable—and linked by the team that runs the Oxford Record Linkage Study (ORLS)14 ,15—therefore, different admissions relating to an individual baby could be identified. Numbers of admissions of babies with ROP and numbers of individual babies with ROP were distinguishable.
Birthweight data
Current UK guidelines advocate ROP screening for all babies born before 32 weeks' gestation and/or <1501 g birth weight. To identify babies eligible for screening, we used publicly available data on birth weight from the Office of Population Censuses and Surveys (OPCS) for England and Wales (as it was until 1996) and by the Office for National Statistics (as it is now).16 ,17 HES data are available for England, whereas birthweight data are published for England and Wales combined. Between 1999 and 2011, live births in Wales accounted for 5.1% (±0.1%) of births in England and Wales. As the percentage is small, and stable, we have accepted the difference in population between HES and birthweight information. As we show below, the discrepancy between numerators and denominators is minor compared with the large changes in diagnosis and treatment rates over time.
Published birthweight data between 1990 and 1998 were subdivided into 500 g intervals: <499, 500–999 and 1000–1499 g. After 1998, these were published as ‘<1500 g’, without further subdivision. The consistently available data on low birthweight (LBW) babies were those on ‘<1500 g’ babies. Annual rates of babies eligible to be screened for ROP have been presented using the total number of babies born <1500 g as the numerator and all live births in England and Wales as the denominator. We acknowledge that, unavoidably, this definition will have excluded a small number of babies born at <32 weeks' gestation but weighing >1500 g.
Annual rates of ROP were expressed per 1000 LBW babies. Birthweight data from England and Wales were used as a denominator to calculate the incidence of ROP among babies eligible for screening.
Clinical codes used
Analyses were undertaken using programmes written by ORLS staff, specifically for record-linked HES data. Records for ROP (any stage of disease) were analysed by identifying all birth, day case and inpatient admission records with code H35.1 (International Classification of Diseases (ICD), tenth revision, used from the mid-1990s) or the code for retrolental fibroplasia (362.2 ICD ninth revision) before then. All analyses were confined to children under 1 year of age.
Operation codes for cryotherapy were obtained from OPCS classification of surgical operations and procedures, fourth revision (OPCS-4), code C82.2, from 1990 onwards. Laser codes (C82.6 and C81.2) were not available until 1999. We calculated incidence of treatment of ROP using cryotherapy and laser as the numerator, and ROP episodes (1990–2011) and ROP individuals (1999–2011) as the denominator. When presenting the data, we show numbers and rates: numbers reflect volume of clinical service, and rates reflect epidemiology of disease and its treatment.
Results
The number of babies born in England and Wales was 706 140 in 1990, and rose to 723 913 in 2011. The number of babies born under 1500 g was 6511 in 1990, rising to 8719 in 2008, and decreasing to 8405 in 2011. The number of babies receiving treatment for ROP was 11 in 1990 and 124 in 2011. Eleven babies had cryotherapy in 1990, peaking at 32 in 1992, and decreasing to fewer than five in 2011; 7 babies had laser treatment in 1999 and 123 in 2011.
Eligibility for screening
The number of live births has fluctuated since 1990, with a dip between 2000 and 2002. The incidence of LBW increased substantially between 1990 and 1998 (table 1).
Live birth data for England and Wales
The early birthweight data (1990–1998) show that the percentage of babies born <999 g, expressed as a percentage of all LBW babies, increased year on year. In 1990, 55% of 6511 babies born under 1500 g weighed <999 g, by 1998 this had increased to 65% of 7920 babies.
Incidence of ROP
The incidence of a recorded diagnosis of any stage of ROP among LBW babies increased tenfold from 12.8 per 1000 LBW babies in 1990 to 125.5 in 2011. Episode-based and person-based rates are shown in figure 1: the episode-based rates (counting each baby for each admission with ROP) and person-based rates (counting each baby once only) show a similar upward trend. The linked data show that an individual baby was admitted on average 1.46 (±0.07) times a year with a coded diagnosis of ROP.

Retinopathy of prematurity (ROP) diagnosis per 1000 low birthweight (LBW) babies recorded as hospital episodes (solid line) and as individual babies (dashed line).
ROP treatment per 1000 LBW babies
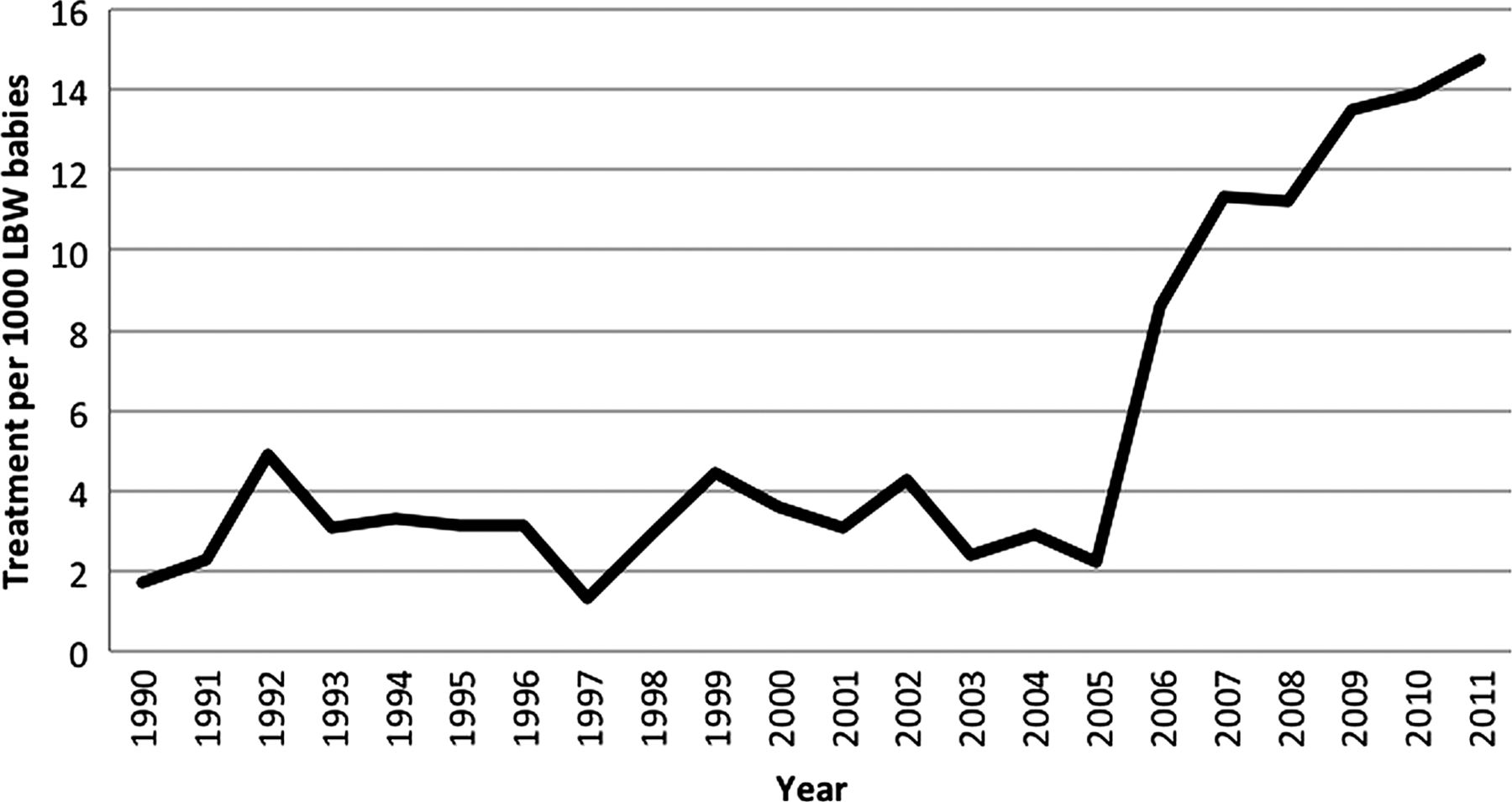
ROP treatment by cyrotherapy or laser rose from 1.7 per 1000 LBW babies in 1990 to 14.8 in 2011 (figure 2), a ninefold increase similar to that seen in ROP itself. There was a dramatic rise in the number of babies treated from 2005, most likely secondary to ET-ROP publication.10

Treatment of retinopathy of prematurity (cryotherapy and laser) in England per 1000 low birthweight (LBW) babies.
ROP treatment
The percentage of babies receiving treatment dipped in 2005 but peaked in 1992 and 2007 (figure 3). The rate of treatment per baby is a better measure than treatment per admission; a baby may have been admitted more than once in a year where an ROP diagnosis was recorded, yet without receiving a procedure. The majority of babies received a procedure once, but some were discharged with an ROP diagnosis on more than one occasion (figures 1 and 3).

Treatment procedures for retinopathy of prematurity (ROP) per 100 discharges with diagnosis of ROP (solid) and per 100 babies with ROP (dashed).
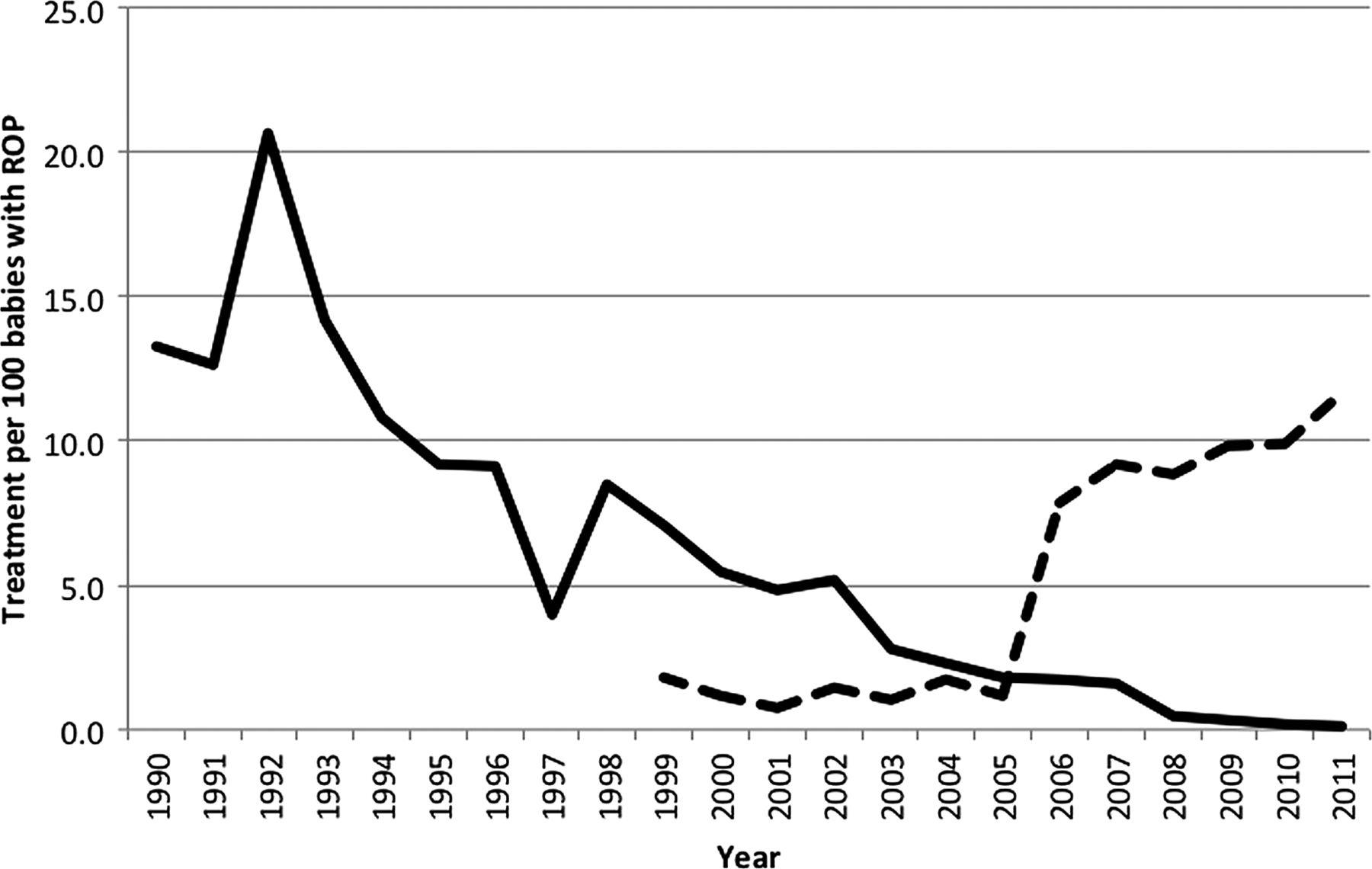
The choice of treatment modality for ROP has changed dramatically (figure 4). In 1990, 13.3% of babies with ROP were treated with cryotherapy versus 0.1% in 2011. The percentage of babies with ROP who underwent laser treatment rose from 1.8 in 1999 to 11.7 in 2011.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cryotherapy treatment (solid) and laser treatment (dashed) per 100 babies with a diagnosis of retinopathy of prematurity (ROP) in England.
Discussion
This study shows that the recorded incidence of any stage of ROP among LBW babies has increased markedly in England over a 21-year period. The scale of increase in ROP is much greater than the rise in numbers of babies born at low birth weights. The proportion of babies treated for ROP has increased in line with the increase in incidence of diagnosed ROP. Treatment of ROP has switched from cryotherapy to the almost sole use of laser.
Incidence of ROP
The most striking finding is the tenfold increase in reported incidence of ROP among LBW babies from 1990 to 2011. Several factors may have contributed: increasing numbers of extremely LBW babies born within the 1500 g group, increasing survival of LBW babies, increased recognition of ROP and increased use of guidelines for screening and treatment.
ROP development is strongly correlated with gestational age and LBW, with the latter being the greater predictor of severity.18 If babies are born at earlier gestations, with lower birth weights, more babies will be at risk of developing ROP. Conversely, survival rates of babies born at earlier gestation are lower and these babies are less likely to require screening. The proportion of babies born <1000 g as a percentage of all LBW babies increased between 1990 and 1998, suggesting that more babies were at risk of developing ROP in 1998 than in 1990.
Babies must survive to 32 postmenstrual weeks of age, or 4 weeks postbirth, in order to be screened. We have no data on babies born at risk of ROP but who die prior to screening. Since the early 1990s, neonatal morbidity and mortality has reduced.19 ,20 ,21 The EPICure studies showed that babies born before 26 weeks' gestation survived to discharge at a rate of 40% in 1995, but 53% in 2006.12 Although the incidence of LBW babies remained static, the number of babies who require screening has increased. Extrapolating from the EPICure studies, it is unlikely that increased survival alone can explain the tenfold increase in ROP incidence.
The first publication of the International Classification of ROP not only clarified the stages or ROP, but it contained a small set of retinal images. Clear evidence came from the CRYO-ROP study that treatment reduced the incidence of blindness. As a result, UK guidelines were published regarding the screening and treatment of babies in neonatal units. Published literature, and images of ROP, has greatly increased since then, allowing easy access to information. With new imaging techniques, it is possible to reveal disease that may have been missed using conventional examination techniques. RCOphth and RCPCH have published standardised documentation for recording of staging and diagnosis in medical records, ensuring consistency both within hospitals and nationally.22 This increase in knowledge and understanding will have had a positive impact on the detection of ROP and will have contributed to the rise in recorded incidence.
This is the first longitudinal study of the incidence of ROP in England. Studies limited to specific groups of at-risk babies, small geographical areas or groups of hospitals, or short periods of time have been published with conflicting evidence, for example, increase in severe ROP incidence in Leicestershire, while reduction of incidence and severity of ROP in Lothian.11–13 ,23 ,24
Treatment of ROP
ROP treatment has changed through the study period. Initially, cryotherapy was proven to be beneficial and was used in isolation. With the development of portable laser, and lately anti-VEGF injections, cryotherapy use has diminished markedly in England. Laser is associated with less morbidity and can be performed in the neonatal unit without transferring the baby to an operating theatre. Laser is less destructive than cryotherapy, and more accurate and targeted treatment is possible.
Our data show peaks of treatment of ROP in 1992 and 2007, consistent with new guidelines published in 1990 and ET-ROP publication in 2003. The proportion of LBW babies treated remains steady until the publication of ET-ROP (figure 2). Figure 3 shows the proportion of babies with ROP requiring treatment falls between 1990 and 2005, suggesting increased detection of the pretreatment stages of ROP. This is consistent with improved screening practices within the UK.
Strengths and weaknesses
We have used HES data for England and birthweight data for England and Wales combined. As babies born in Wales represent a small and stable percentage of the total live births, it is reasonable to accept this. Its effect is that calculations based on the artificially inflated denominator produce slightly lower population-based rates.
The HES system provides a unique, continuous source of data that enable the incidence of a disease and its treatment to be monitored over an extended period of time. However, an inherent weakness is that data collection relies on the coding and input of clinical terms from clinical records, and, if key clinical phrases are missing, or undecipherable, it is possible to underestimate true rates. Despite this, our data correlate closely with data collected from the independent dataset of the National Neonatal Research Database, in the years covered by both.25 The forthcoming British Ophthalmic Surveillance Unit audit on treatment of ROP should provide more data of contemporary surgical volume.
We used the full run of HES, rather than starting with linked data in 1999, because we wanted to give as full a profile as possible of the history of recorded ROP and its treatment.
Conclusion
This paper provides national data on trends in ROP incidence and treatment in England over a 21-year period. Increased neonatal survival, improved awareness of ROP and dissemination of guidance on screening and treatment of ROP will all have contributed to the substantial rise in recorded incidence of ROP. The data can be used as a baseline for further studies of incidence, severity and treatment.
Acknowledgments
David GR Yeates designed the software required to analyse the HES data and Nick Hall provided programming support.
References
Footnotes
-
Contributors CKP posed the research question. MJG provided the raw data and methodology. SLP interpreted and acquired data and wrote the paper. CKP, MJG, ARW and PD contributed to and reviewed the paper.
-
Funding The Unit of Health-Care Epidemiology was funded by the English National Institute for Health Research (grant number RNC/035/02) to build and analyse the linked data. The views expressed in this paper do not necessarily reflect those of the funding body.
-
Competing interests None.
-
Ethics approval Ethical approval for a programme of work constructing and analysing the record linked HES dataset was obtained from the Central and South Bristol Multi-Centre Research Ethics Committee (04/Q2006/176).
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance