Article Text

Abstract
Objectives: To examine the transport times of immediate and emergency retrievals for neonatal and paediatric patients retrieved by ground and air from general hospitals to tertiary centres.
Designs: We conducted a database review of the records of 17 011 requests for retrieval to a centralised transport service in New South Wales and the Australian Capital Territory, Australia from 2000 to 2006.
Results: Immediate and emergency retrievals included 4575 (43.7%) neonatal and 5887 (56.3%) paediatric retrievals. The median stabilisation time was 97 min for neonatal compared with 50 min for paediatric retrievals. Neonatal retrievals had a significantly longer stabilisation time (approx ×2), handover time (approx ×1.2) and mission time (approx ×1.3) compared to paediatric retrievals.
Conclusions: Establishing reference times for the transport process is a valuable quality assurance tool. Such data will be valuable for staff and budgeting purposes and for evaluating new interventions that reduce retrieval times.
Statistics from Altmetric.com
There are few data regarding response, stabilisation and retrieval time in large centralised retrieval services. Such data would be valuable for quality assurance, staff and budgeting purposes and for evaluating new interventions that reduce retrieval times.1–4 Indeed, the need for such data for quality improvement is emphasised by the American Academy of Pediatrics (AAP)2 3 and the AAP Section on Transport Medicine (SOTM).4 Their guidelines stress that quality assurance should continually monitor and evaluate the transport program to ensure that quality patient care is provided and that the program meets defined standards including response and turnaround times. Furthermore, new interventions that reduce retrieval times could be evaluated using these times as a reference. The purpose of this study was to examine the transport times of immediate and emergency retrievals for neonatal and paediatric patients retrieved by ground and air from general hospitals and maternity homes in New South Wales (NSW) and the Australian Capital Territory (ACT) to tertiary centres in NSW and ACT over a 6-year period.
METHODS
Data source and patient population
Data were obtained from the New South Wales Newborn and Paediatric Emergency Transport Service (NETS) database for all newborns and children who were retrieved between January 2000 and December 2006. Operationally, NETS data were prospectively collected and collated within the NETS base by the transport teams.5 6
State-wide health service and NETS organisation
NETS is an integrated centralised emergency transport service covering the state of New South Wales (NSW) and the Australian Capital Territory (ACT). The goal has been to provide intensive care in the referring hospital before transport as well as during it. A fuller description of NETS and the NSW and ACT health service organisation has been published previously.5–7
NSW and the ACT have highly regionalised neonatal and paediatric intensive care. There are 10 neonatal and paediatric intensive care units clustered within the Sydney, Newcastle and Canberra metropolitan areas and there another 150 non-tertiary and rural hospitals across the region which are potential points of referral.
NSW (including the ACT), and thus NETS, covers an area of 815 810 km2 (10.5% of Australia’s total area) and has a population (including the ACT) of 7 173 700 (33% of the total Australian population) with ∼40% living in rural areas.8
The retrieval process
The retrieval process is started when a clinician from the referring hospital contacts NETS. The calls are answered by a clinical coordinator who immediately connects the caller with a NETS medical consultant. A clinical conference call is set up with specialists from the hospital nominated as the preferred destination for the patient.
Telephone triage categorises the clinical urgency of the case as: (1) immediate priority – in extremis or deteriorating or needs urgent, time-critical therapy; (2) emergency priority – serious condition and treatment required is not possible in the referring hospital; (3) elective priority – timing discretionary.
The standard composition of the transport team is doctor/nurse (senior registrar or fellow grade and transport nurse). For more stable patients, the team is nurse or nurse/nurse. The team configuration and skills and equipment for paediatric and neonatal transport for both air and ground retrievals meet established guidelines similar to those of the American Academy of Pediatrics.2–4 9
Statistical analysis
Results are presented as percentages or median with interquartile range (IQR, 25th to 75th centile). The Mann–Whitney U test was used where appropriate. All computations were performed using the Statistical Package for Social Sciences for Windows v 11.5.0 (SPSS, Chicago, IL). The level of statistical significance for all analyses was set at p<0.05 using two-tailed comparisons. The final analysis was restricted to immediate and emergency priority patients.
RESULTS
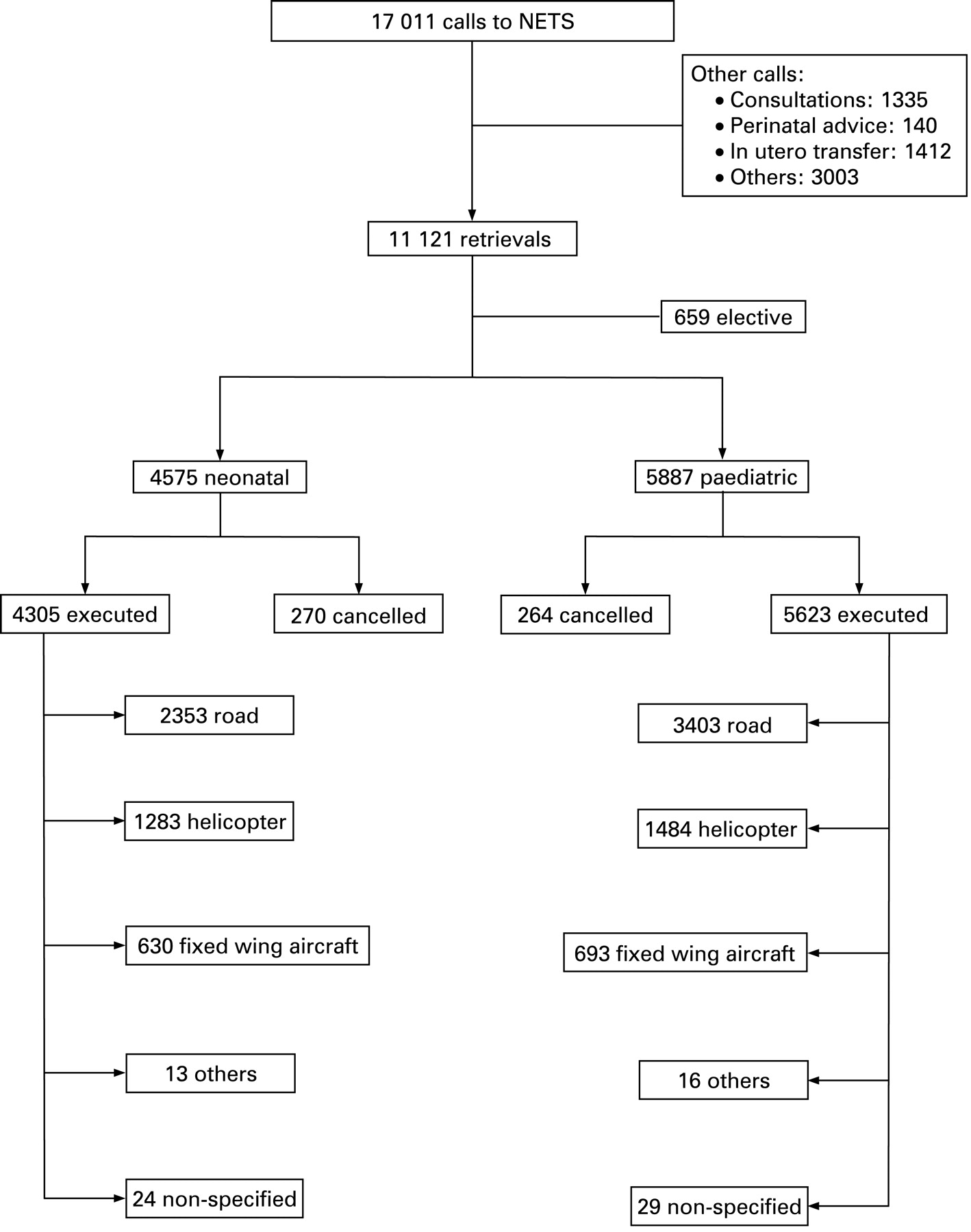
The NETS Clinical Coordination Centre handled 17 011 calls during the study period (an average of 2431 calls per year). Of these, 65.3% were calls for retrievals and 8.3% were for in utero transfer to tertiary centres (fig 1). Road ambulances were used in 58.0% of retrievals, followed by helicopters (27.9%), fixed wing aircraft (13.3%) and others (eg, commercial and charter aircraft).
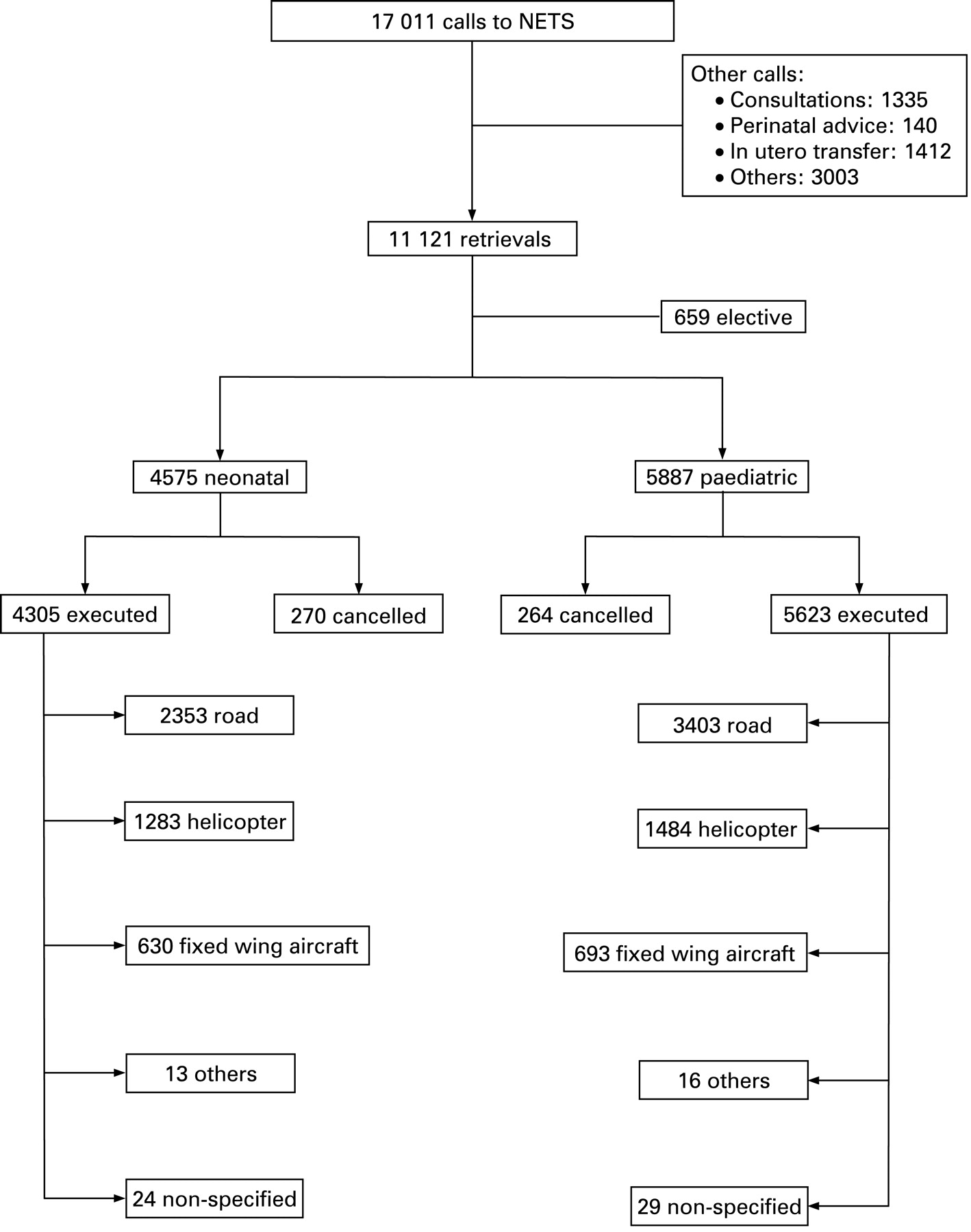
Flow chart of the calls handled by the NETS Clinical Coordination Centre over the study period. NETS, New South Wales Newborn and Paediatric Emergency Transport Service.
There were 5887 (56.3%) immediate and emergency paediatric retrievals compared to 4575 (43.7%) neonatal retrievals. A total of 264 (4.5%) paediatric retrievals were cancelled compared to 270 (5.9%) neonatal retrievals. The reasons and time from call to cancellation of these requests are shown in table 1.
Neonatal retrievals
Of the 4575 neonates, 3213 (70.2%) were less than 24 h old and 553 (12.1%) less than 7 days of age at the time of the call. The median gestational age was 37 (range 23–44) weeks and median birth weight was 2800 (range 400–6100) g. There were 2528 (55.2%) male neonates and eight (0.2%) with ambiguous genitalia.
The clinical reasons for neonatal retrieval included prematurity, respiratory distress syndrome, meconium aspiration, sepsis, surgical abnormality, and congenital and genetic abnormalities.
The medians (IQR) of the components of neonatal retrieval time are shown in table 2. The median (IQR) discussion time (the time from the start to the end of the first NETS call) was 10 (7–15) min. Team tasking and mobilisation took 11 (6–15) and 3 (0–10) min, respectively. The median (IQR) stabilisation time (from first look at the patient until the team was ready to depart from the referring hospital) was 97 (56–153) min. The median (IQR) time for the mission (from departure until return back to the NETS base after completing the transfer) was 350 (265–480) min; a median (IQR) of 139 (5–253) min of this time was spent on travel.
Paediatric retrievals
A total of 5887 paediatric retrievals were executed. These included 1240 (21.1%) patients aged ⩽6 months, 555 (9.4%) aged 6–12 months and the rest aged over 1 year. Males constituted 3335 (56.6%) of this sample.
The main clinical reasons for paediatric retrieval included asthma/bronchiolitis, sepsis and surgical abnormality.
The medians (IQR) of the components of paediatric retrieval time are shown in table 2. The median (IQR) discussion time was 15 (11–20) min. Team tasking and mobilisation took 13 (8–20) and 4 (0–11) min, respectively. The median (IQR) stabilisation time was 50 (33–80) min. The median (IQR) time for the mission was 260 (197–371) min, of which a median (IQR) of 117 (78–194) min was spent on travel.
Neonatal versus paediatric retrievals
Compared with paediatric transfers, neonatal transfers had significantly longer stabilisation time (p<0.001), handover time (p<0.001) and mission time (p<0.001). In contrast, paediatric retrievals had significantly longer discussion time (p<0.001) (fig 2).

{kind=link}
{kind=link}
Box-and-whisker plot comparing the main components of the retrieval times for neonatal and paediatric transfers (*p<0.05).
The number and type of procedures undertaken by the retrieval team for both paediatric and neonatal retrievals are shown in table 3. These included respiratory (eg, endotracheal intubation), ventilatory and circulatory (eg, inotropes) interventions.
DISCUSSION
No benchmarks currently exist for establishing the appropriate lengths of the various components of the transport process. Furthermore, interpretation of any published “standard times”, when available, should be viewed in the context of the catchment area covered by the transport service, the experience and staffing of the transport service, the facilities at the referring hospital and the experience/expertise of local doctors (eg, prior resuscitation and stabilisation before the arrival of the transport team) and the severity of the patient’s condition.
Minimising the time taken from the first contact with the health service to patient arrival at an appropriate destination hospital is a prime goal of any transfer service. Various strategies aim to reduce the time of each component without compromising patient care.
Our data showed a median (IQR) discussion time of 10 (7–15) and 15 (11–20) min for neonatal and paediatric transfers, respectively. Maintaining short discussion times is achieved by bringing multiple parties involved in the care of the patient (transport, referring, receiving teams and any other specialised service deemed necessary) together by using a virtual conference room to involve all relevant parties in one conversation rather than several separate conversations. The discussion should focus on the key clinical management issues and sorting out the logistics (eg, bed availability) after the referring hospital has left the call and a NETS team is activated.10
The team and vehicle activation and mobilisation times are components which should be minimised. In our setting, the teams and vehicles (with the exception of the fixed wing aircraft) are stationed at the headquarters and are easily activated upon receiving a request for retrieval.
The travel time depends on multiple factors including geographical distance, mode of transport (surface or air) and functional distance (team and vehicle availability, launch, loading and taxiing times, and number of vehicle changes).11 The choice of vehicle depends on the distance and the total time involved in the outward and return journeys and the requirements of the patient’s condition. Other considerations may include the availability and/or proximity of airports or helipads and weather conditions. The advantages and disadvantages of each vehicle are discussed elsewhere.3 11 12 Our relatively longer travel time (table 2) and the variety of modes of transfer (fig 1) reflect our sparsely populated state and the long distances needed to travel combined with unpredictable weather conditions.
The response time is an important quality indicator reflecting and affected by many factors including clinical urgency, time to tasking, mobilisation and geographical and functional distances. The median (IQR) response time of 75 (51–140) and 65 (47–115) min for neonatal and paediatric transfer, respectively, is less than that of Holt et al who described a response time of 120 (100–145) min for newborn infants transferred in a sparsely populated area in Norway.13 Kempley et al described a median response time of 87 min for a centralised transfer unit in a geographically defined area in London and southeast England.14 Longer response times place sick patients at risk and it is important that the transport service/receiving team advises the local team at the referring hospital on continuing management at the time of the original call, particularly when distance increases the overall process and the time taken to reach definitive care.11 Broughton et al found that the greatest improvement in the clinical condition of sick infants, measured by a modified Clinical Risk Index for Babies, occurred between the initial phone call and the arrival of the transfer team.5
Our median (IQR) neonatal (97, 56–153 min) and paediatric (50, 33–80 min) stabilisation times are longer than those described by Holt et al (neonatal: 60, 40–70),13 Moss et al (neonatal: 60, range: 5–840)15 and Whitfield et al (neonatal: 80, range 15–590 and paediatric: 45, range 10–419).1 These differences are likely to reflect differences in the study populations and illness severity. Ideally, the process of stabilisation should begin at the time of the original call to the transfer unit when advice is given by the transport, receiving and other specialised teams. It is important that following the initial multi-party conference call, basic stabilisation manoeuvres should start promptly and discussion with the parents should not await the arrival of a transport team, particularly when distance increases the overall process and time taken to reach definitive care.11 A balance should be achieved between these interventions and the urgency of the transfer as rushed stabilisation and “wrap and run” or “swoop and scoop”, while achieving the goal of transferring the patient more quickly, may have disastrous consequences.1 9 11 Exceptions include certain surgical conditions, for instance requiring the evacuation of a patient with an intracranial haematoma.12
What is already known on this topic
There are few data regarding response, stabilisation and retrieval times in large centralised retrieval services.
Such data would be valuable for quality assurance, staff and budgeting purposes and for evaluating new interventions to reduce retrieval times.
What this study adds
Detailed reference times for the various components of the transport process in a large centralised service have been established.
These data can be used for benchmarking and quality improvement in similar settings.
Our data showed that paediatric transfers had a longer discussion time (approx ×1.5) compared with neonatal transfers (fig 2). In contrast, neonatal transfers had a significantly longer stabilisation time (approx ×2), handover time (approx ×1.2) and mission time (approx ×1.3). The longer handover time might reflect the fact that neonatal transfer involves the maternal history in addition to the infant’s history. The stabilisation of these infants, especially newborns, often involves multiple procedures unique to this age group, such as umbilical line insertion in addition to intubations, etc, depending on the clinical status of the infant. These factors might lead to a longer stabilisation and mission time for neonatal transfer.
CONCLUSION
Our findings provide reference times for the duration of the transport process in a centralised paediatric and neonatal transport system. These results can be used for quality assurance, staff and budgeting purposes. Furthermore, new interventions that reduce retrieval times can be evaluated using these times as a reference.
Acknowledgments
We thank the NETS doctors, nurses and clerical staff. We also thank the nursery, obstetric and medical records staff members of the obstetric and children’s hospitals in NSW and the ACT.
Footnotes
Funding: None.
Competing interests: None.