Article Text

Abstract
Aims: To determine whether current and postpartum maternal depression and low maternal intelligence are risk factors for malnutrition in children.
Methods: In rural South India 72 children with malnutrition were identified from a central register; 72 controls were matched for age, gender, and residence.
Results: Major depression in the postpartum period (OR 5.0, 95% CI 1.0 to 24.0), current major depression (OR 3.2, 95% CI 1.1 to 9.5), and low maternal intelligence (OR 3.8, 95% CI 1.3 to 11.1) were associated with malnutrition in the child. Low birth weight (OR 2.9, 95% CI 1.2 to 6.8) was also significantly associated with infant malnutrition. Conditional logistic regression adjusting for all other determinants yielded the following results: major depression during the postpartum period (OR 7.8; 95% CI 1.6 to 38.51), current major depression (OR 3.1; 95% CI 0.9 to 9.7), low maternal intelligence (OR 4.6; 95% CI 1.5 to 14.1), and low birth weight (OR 2.7; 95% CI 2.5 to 6.8). The interactions between current maternal depression and low birth weight and between postpartum depression and low maternal intelligence were statistically significant. The level of maternal intelligence was associated with nutritional status. The severity of malnutrition was also significantly associated with major depression during the postpartum period and low maternal intelligence.
Conclusion: There is evidence for an association between postpartum maternal depression, low maternal intelligence, and low birth weight with malnutrition in children aged 6–12 months.
Statistics from Altmetric.com
Malnutrition is a major public health problem in the developing world; national surveys have documented mild to moderate malnutrition among over a third of all children in the State of Tamil Nadu, South India.1 Many factors have been shown to be associated with malnutrition, including (1) nutritional factors (for example, breast feeding, weaning, and nutritional supplementation);2–5 (2) socioeconomic factors;6,7 and (3) health status of mother (for example, maternal malnutrition, teenage pregnancy, and antenatal care).1 In addition to these, there is evidence that depression in the postnatal period8–10 and low maternal intelligence11,12 and are also associated with malnutrition in children. We are not aware of studies which have simultaneously examined all these factors. We attempted to examine the association between low maternal intelligence and current and postpartum maternal depression with malnutrition in children after adjusting for the other known causes of malnutrition.
METHODS
The setting
The Department of Community Health, Christian Medical College, Vellore, India has been working in Kaniyambadi Block for the past 40 years.13 This region is a geographically defined area of 127.4 km2 with a population of 109 872. The community programme operates in all 85 villages in the area. The majority of the population follow the Hindu religion. The language spoken is Tamil. A significant proportion of the population is from the lower socioeconomic strata. Agriculture and animal husbandry are the major occupations.
The Community Health and Development (CHAD) programme is run by the Department. The programme has four major components: health care, animal husbandry and agriculture, adult and non-formal education, and community development. The front line of CHAD’s health care structure is the community health worker. They are traditional midwifes who live in the village who have been trained by the programme. The community health worker is supported by the community health team (including a doctor, nurse, community extension worker, health aide), which visits each village every two weeks. Cases requiring greater medical input are referred to the base hospital. The base hospital has 80 beds. The hospital treats a wide variety of patients including those with tuberculosis, leprosy, rheumatic heart disease, and AIDS. Normal delivery, sterilisation, and child health clinics form the major component of the health care provided.
The database
Each child has a record of all immunisation received. The child’s height, weight, head circumference, and motor milestones are also recorded (at birth, 6, 10, and 14 weeks, and then at 9 and 18 months) by the CHAD programme. The government also monitors the health of all children through its Integrated Nutrition Programme. This scheme also records weights of children at monthly interval from birth to 36 months. This information is transferred to the CHAD database. The health aide calculates the nutritional status based on the child’s weight and the expected weight for age. The classification of malnutrition, recommended by the Indian Academy of Paediatrics, which employs the expected weight for age as the norm, is used to grade malnutrition (normal weight, 80% and above; grade I, 70–79%; grade II, 60–69%; grade III, 50–59%; grade IV, <50% of expected weight for age).14 This measure is recommended for routine assessment of nutritional status in the community because it is inexpensive and easy to apply. This data are stored on the CHAD surveillance system central computer. The children who are diagnosed to have malnutrition are monitored every month. The central database is updated every month with information from the village community health workers and the government nutrition programme. Details of the surveillance system have been described elsewhere.15
Cases and controls
We defined as cases those children with weights between 50% and 80% of their expected weight for age while controls were those with more than 80% of their expected weight for age. We excluded children (from both case and control groups) according to the following criteria:
-
If the mother was not the primary care giver.
-
Children from single parent homes. (Infants being looked after by single parents are uncommon in the region. The socioeconomic and emotional burden in such families is very significant as there is no welfare system or social services in the country. It was felt that we would not be able to recruit matched controls living on the same street and hence children from single parent homes were excluded from among both case and control groups.)
-
Children whose birth weights were less than 2 kg.
-
Children who were preterm babies.
-
Children with any obvious co-morbid physical illness.
The database was used to identify cases of malnutrition aged 6–12 months, from among the resident population of programme area from July 2000 to February 2001. These children were re-examined by the health aide and the current weights recorded. Only children who were reconfirmed to have malnutrition were included in the study. Using the same database, controls matched with a case for age, sex, and locality were randomly selected. These children were also re-examined by the health aide to reconfirm their status as normal weight controls.
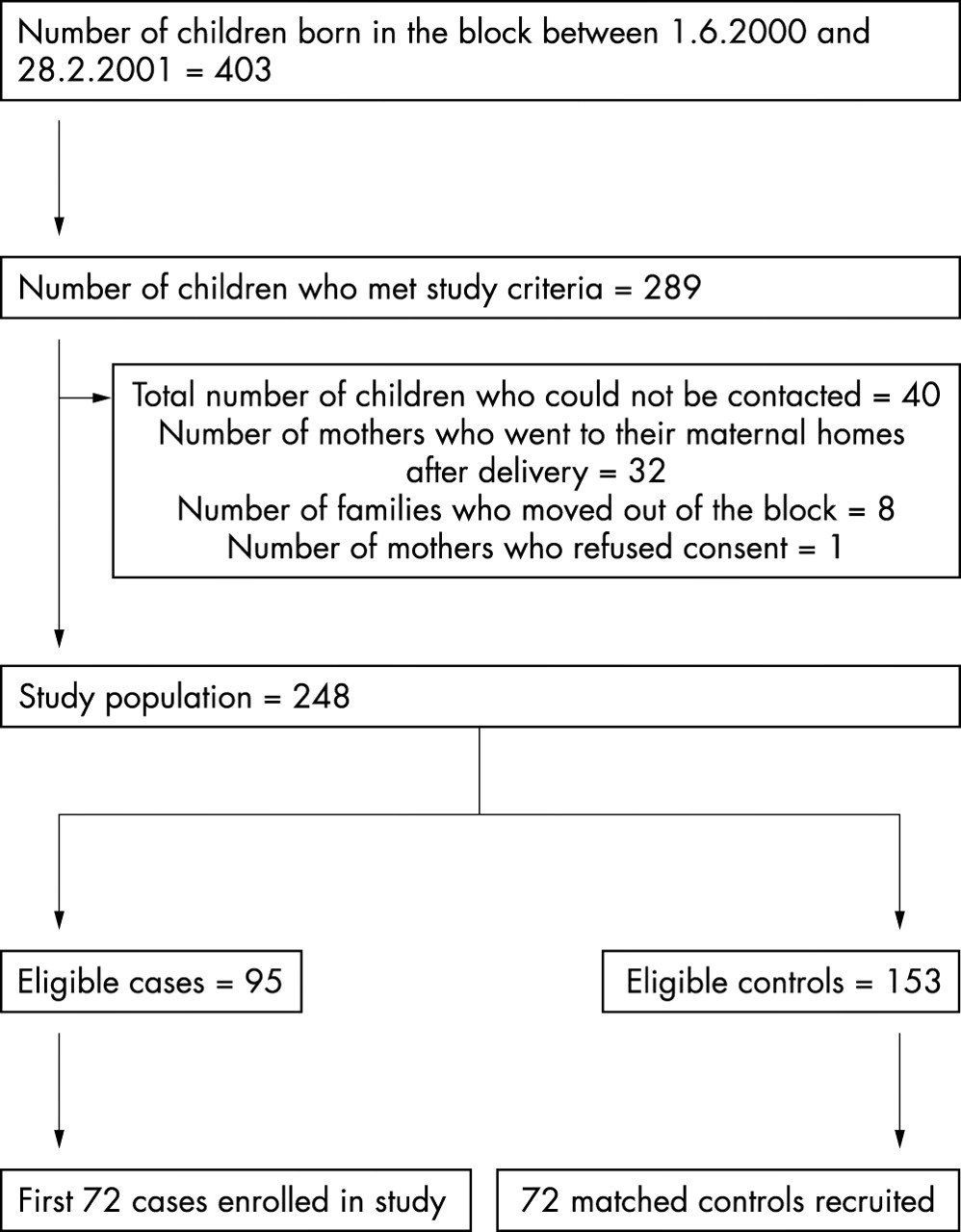
Figure 1 shows the details of recruitment. The first 72 children with malnutrition who were contacted were recruited; 72 controls were also selected, matched for age, gender, and residence (living in the same street). A total of 144 records were copied from the archives and given code numbers to conceal case or control status. The records were randomly assembled and given in batches to the primary investigator (SA), who extracted data according to a protocol devised by the research group. The investigator (BS) who prepared the list of all children was not involved in the assessment of mothers. The investigator (SA) who interviewed the mothers was not aware of the nutritional status of the child.

{kind=link}
Flow chart of recruitment of cases and controls.
Assessments
Mothers of the cases and controls were interviewed to assess psychiatric morbidity, intelligence, sociodemographic, and other factors associated with malnutrition. The Structured Clinical Interview for DSM III R (SCID, patient edition)16 was used to assess psychiatric morbidity. Standard procedures, including translation-back translation, were employed to obtain equivalence.17 Two bilingual health professionals who were proficient in English and Tamil initially translated the schedule into Tamil. Two other health professionals then back translated the vernacular version obtained into English. The final Tamil version was arrived at by a consensus by all four translators, with attention being paid to content, semantic, technical, and conceptual equivalence. The following definitions of depression were employed: Diagnostic and Statistical Manual III Revised (DSM III R) major depression during the month after childbirth was considered as postpartum depression; DSM III R major depression during the past one month was considered as current depression.
The Revised Bhatia’s Short Battery of performance tests to assess intelligence in adults,18 a measure standardised for the India population,19 was used to assess the intelligence quotient. It has been validated against three standard intelligence scales (Raven’s Standard Progressive Matrices, Wechsler’s Adult Performance Intelligence Scale, and Wechsler’s Adult Verbal Intelligence Scale) and the scores have been shown to have a high correlation. Normative tables are provided for age, sex, and education groups. It takes 20–30 minutes to administer. An intelligence quotient of 70 or less was considered as low intelligence.
A specially designed proforma was used to assess the sociodemographic characteristics, health status of parents, details of the pregnancy and delivery, antenatal care, details of breast feeding, medical illnesses, and immunisation status. Inability to buy food in the past month, type of house, and number of square meals per day were used as proxy indicators of socioeconomic status, as a direct assessment of such status is difficult in developing countries. The assessments were done at home.
Statistical methods
Our outcome variable was infant malnutrition (grades 1–3). Student’s t test or the χ2 test was used to assess the potential association between the determinants of interest and malnutrition. The determinants of interest were current maternal depression (DSM III-R major depression), postpartum maternal depression (DSM III-R major depression), and low maternal intelligence (IQ of 70 or less). The magnitude of the association between these potential determinants and malnutrition was first expressed using crude odds ratios with 95% confidence intervals. Conditional logistic regression analysis was done using the following variables:
-
Variables of interest: current maternal depression, postpartum maternal depression, and low maternal intelligence.
-
Birth weight: low birth weight was entered in the model as there was a significant difference between cases and controls. Indicator variables were created for birth weight categories as the relation between malnutrition and birth weight was non-linear.
-
Other known risk factors for malnutrition: socioeconomic status, maternal literacy, immunisation status, duration of exclusive breast feeding, and duration of supplemental breast feeding.
Statistical significance in the logistic regression models was assessed using the Wald statistic. Both backward and forward inclusion of variables were used in the logistic regression model building procedure in order to identify the final model. We also constructed additional models to assess interaction effects between the main variables of interest. The association between infant malnutrition and levels of maternal intelligence was tested for trend. The significance of the association between the severity of malnutrition and other variables was also assessed. SPSS for Windows 6.0 was used to analyse the data.
Sample size
A survey of postnatal depression in the region had documented a prevalence of 19.8%.20 Assuming depression in mothers with normal weight children to be 20% and an odds ratio of 3 for depression in mothers with a malnourished child we needed 72 case-control sets (one case to one control) with an 80% power and 5% significance. Epi Info (version 6.04b) was used to calculate sample size.
RESULTS
Table 1 presents the characteristics of cases and controls. The differences in birth weight (p<0.01, 95% CI −0.04 to −0.1) and current weight (p<0.001, 95% CI −1.7 to −1.2) between cases and controls were statistically significant. The cases and controls were matched for age, gender, and street of residence. The matching for place of residence resulted in socioeconomic status similarities between cases and controls. Other factors (past medical illnesses, immunisation, maternal body mass index and weight, access to medical care, type of family, and total number of children were not significantly associated with case status). There were 47 (65.3%) cases with grade I malnutrition, 18 (25.0%) cases with grade II, and 7 (9.7%) with grade III malnutrition.
Baseline characteristics of cases and controls
Table 2 shows the unadjusted and adjusted odds ratios for postpartum and current maternal depression, low maternal intelligence, and low birth weight. Low maternal intelligence, postpartum depression, and low birth weight were independent risk factors for infant malnutrition even after adjustment for other determinants. The interactions between current major depression, postpartum depression, low maternal intelligence, and low birth weight were tested using conditional logistic regression. The interactions between current maternal depression and low birth weight (OR 1.8; 95% CI 1.2 to 2.8; p = 0.003) and between postpartum depression and low maternal intelligence (OR 3.3; 95% CI 1.6 to 6.8; p = 0.001) were significant. This implies that that the odds ratio for malnutrition among children whose mothers had major depression (current) and who were born low birth weight was 15.1 (OR = 2.7×3.1×1.8), compared with children whose mothers did not have major depression currently and who were not born low birth weight. Similarly, the odds ratio for malnutrition among children whose mothers were of low intelligence and who had major depression (postpartum) was 112.3 (OR = 7.4×4.6×3.3), compared with children whose mothers did not have major depression (postpartum) and whose intelligence quotient was over 70. The other interactions were not statistically significant.
Association between determinants (current maternal depression, postpartum maternal depression, low maternal intelligence, and low birth weight) and infant malnutrition
Table 3 shows the association between levels of maternal intelligence and malnutrition. The lower the intelligence level the greater the risk of malnutrition in the child. The effect was greatest for mothers’ with IQ less than 70 compared with IQ greater than 111, suggesting a negative association between maternal intelligence and malnutrition.
The relationship between level of mother’s IQ and malnutrition in the child
Table 4 shows the association between grades of malnutrition and the other variables. There was a significant association between the presence of postpartum depression, low maternal intelligence, birth weight, and duration of supplemental breast feeding with the severity of malnutrition. The other socioeconomic and clinical variables were not associated with severity of malnutrition.
The association between grades of malnutrition and other variables
DISCUSSION
We used a case-control study design in order to assess the many factors associated with malnutrition in a rural South Indian population.
Attempts to overcome limitations of case-control designs
The study has the limitations of case-control designs. However, these were minimised using the following strategies: cases and controls were selected using the same reference framework with similar exclusion criteria for unbiased referral; the assessor who evaluated the mother was blind to the nutritional status of the child to prevent bias; standard interview schedules were employed to reduce recall bias; exposures (DSM III R major depression and IQ <70) were defined prior to the commencement of the study; and multivariate analysis was used to exclude confounders. The refusal of consent for the study was low and excludes participation bias. The interview schedule to assess depression is a standard instrument, which is routinely employed in research. It is a valid measure of both current and lifetime depression. The measure to evaluate the intelligence quotient used is performance scale and was chosen because of its ease of administration in the field. It has been evaluated against more detailed methods of assessment and found to be a valid a measure of intelligence. This study is limited to very young children (6–12 months). Consequently, generalisation of these results to children of other age groups requires caution.
Risk factors for malnutrition
We found that malnutrition in children was associated with mothers with postpartum depression, current major depression, low maternal intelligence, and low birth weight. The association remained statistically significant after other confounding factors had been taken into account. The presence of postpartum and current maternal depression, low intelligence, and low birth weight greatly increased the risk of malnutrition in the child. However, the evidence for current maternal depression as a risk factor for infant malnutrition was weaker than for postpartum depression, low maternal intelligence, and low birth weight. In addition, current maternal depression can be a consequence of infant malnutrition rather than cause of malnutrition. The risk of malnutrition was higher with lower levels of maternal intelligence.
Many of the traditional factors associated with malnutrition, being related to socioeconomic status, were not significantly associated with malnutrition in this study. The matching of cases with controls living on the same street resulted in similar profiles for both groups on socioeconomic factors and related variables. The similar prevalence of these variables in both groups resulted in other clinical variables (current and postpartum maternal depression, low maternal intelligence, low birth weight) being significantly associated with the nutritional status of the child.
While postpartum depression precedes the development of malnutrition in the child, the current depression may be a consequence of the nutritional status. However, depression in mothers, due to any cause, can have a major impact on the nutrition of the child. Depression is known to reduce maternal interest in child rearing.21,22 The disability due to depression can result in reduced nutrition for the child. The emotional distress associated with depression may impair the woman’s ability to cope with motherhood and lead to a vicious cycle of despair. In addition, the lack of initiative can result in the failure to supplement nutrition during the weaning period. The recognition and management of depression in mothers may help prevent malnutrition in children. This needs to be confirmed using randomised trials.
Lower maternal intelligence can also impact on the child’s nutrition. The lower ability to grasp the need to supplement nutritious food during the weaning period can result in malnutrition. Low maternal intelligence may also affect prenatal maternal nutrition and consequently birth weight of the child. Although mothers are taught about nutrition and supplementary feeding, mothers with lower intelligence will need simple instruction and greater supervision (from relatives and community health workers) to prevent malnutrition in their children. There is a need to focus on mothers with lower intelligence in addition to providing general education.
Low birth weight was a risk factor in the development of infant malnutrition. Infants of mothers with poor nutrition or diseases during pregnancy, which result in low birth weight, are at increased risk to develop malnutrition. Preterm or small for gestational age babies will be at increased risk for malnutrition. Consequently, increased vigilance in children born with lower birth weights is necessary. In addition, monitoring fetal growth during pregnancy and managing problems can also prevent the development of malnutrition by increasing birth weight.
Implications of the study
The results of this study suggest the possibility of interventions to prevent malnutrition in children by recognising and managing depression and lower intelligence in mothers. The identification of socioeconomic factors by the primary health care team, which are associated with malnutrition, did not allow them to intervene as they are not empowered to change the socioeconomic status. The recognition and management of these medical conditions (current and postpartum maternal depression and lower intelligence) will allow health teams to focus their interventions. Randomised controlled trials assessing the efficacy of recognition and management of maternal depression and lower maternal intelligence in preventing malnutrition in infants need to be carried out to confirm the efficacy of such interventions.
Acknowledgments
We thank the mothers and children who took part in the study and the community health workers and health aides for their cooperation and help in recruitment. We thank Dr KS Joseph for statistical advice.
REFERENCES
Footnotes
-
Funding: Research Grant No. 22F744 from the Christian Medical College, Vellore, India.