Article Text

Abstract
BACKGROUND The physiological basis underlying the decline in the incidence of sudden infant death syndrome (SIDS) associated with changing the sleep position from prone to supine remains unknown.
AIMS To evaluate diaphragm thickness (tdi) and shortening in healthy term infants in the prone and supine positions in order to determine whether changes in body position would affect diaphragm resting length and the degree of diaphragm shortening during inspiration.
METHODS In 16 healthy term infants, diaphragm thickness at the level of the zone of apposition on the right side was measured using ultrasonography. Heart rate (HR), breathing frequency (f), and transcutaneous oxyhaemoglobin saturation (Sao 2) were recorded simultaneously during diaphragm imaging with the infants in the supine and prone positions during quiet sleep.
RESULTS At end expiratory (EEV) and at end inspiratory lung volumes (EIV), tdi increased significantly in the prone position. The change in tdiduring tidal breathing was also greater when the infant was prone. Sao 2, HR, and f were not significantly different at EEV and at EIV in both positions.
CONCLUSION In healthy term infants, placed in the prone position, the diaphragm is significantly thicker and, therefore, shorter, both at EEV and EIV. Diaphragm shortening during tidal breathing is greater when the infant is prone. In the prone position, the decreased diaphragm resting length would impair diaphragm strength, and the additional diaphragm shortening during tidal breathing represents added work performed by the diaphragm. This may compromise an infant's capacity to respond to stressful situations when placed in the prone position and may contribute to the association of SIDS with prone position.
- diaphragm
- infant
- sudden infant death syndrome
- sleep position
Statistics from Altmetric.com
There is a strong association between the prone sleep position and sudden infant death syndrome (SIDS).1-9 Proposed, but uncertain, mechanisms underlying this association include upper airway obstruction, rebreathing of expired air, thermal stress, reduced cerebral blood flow, and a higher arousal threshold.10-17However, no adverse effects of the prone position on respiratory mechanics have been found in term infants, and, to the contrary, studies of preterm infants suggest that the prone position is physiologically advantageous.18-24 Consequently, no specific posture induced compromise of respiratory mechanics has been linked with SIDS. Differences in diaphragm function between the prone and supine positions, however, have not been fully explored in infants.
The diaphragm is the primary respiratory muscle for the neonate and performs the majority of the work of breathing.25 In the prone position, alterations in respiratory system mechanics or changes in lung volume may affect the resting length of the diaphragm or the degree to which it shortens during inspiration. The effect of the prone position on diaphragm length, however, has not been studied in infants. We postulate that position induced alteration in diaphragm function may explain, in part, the association of the prone sleep position with SIDS. The purpose of this study was to evaluate position related alterations in diaphragm resting length and diaphragm shortening during tidal breathing in healthy term infants. Our premise was that diaphragm length and, therefore, diaphragm function, differs in the prone and supine sleep positions.
Methods
After written parental consent, 16 healthy term (eight boys and eight girls) appropriate for gestational age infants who had no clinical evidence of cardiorespiratory compromise or any other illness were studied within two days of delivery, except for one infant who was studied on day 17 of life (table 1). Birth and study weights were 3.3 (0.6) kg (mean (SD)) and mean head circumference and body length were 33.5 (2) cm and 50 (3) cm, respectively. Mean gestational age was 39 (0.9) weeks, and postnatal age was 3 (4) days. Twelve infants were delivered vaginally and four by Caesarean section. Their mean Apgar scores were 9 (1) and 9 (0) at one and five minutes, respectively.
Patient characteristics
All infants were studied in a nursery while sleeping comfortably under a radiant warmer. Studies were performed about one hour postprandially during quiet sleep. If the infant became agitated, he or she was calmed with a pacifier. All studies were completed within 30 minutes. The infants were randomly assigned to either the supine or prone position. After obtaining data in the initial position, the infants were repositioned and allowed to settle down in the other position before being restudied. In both positions, the head was placed sideways. When prone, the infant's abdominal wall was resting against the mattress.
Infant sleep states were characterised as active or quiet according to behavioural criteria.26 Active sleep was defined by rapid eye movements, frequent body and facial movements, and irregular breathing with paradoxical movements of the rib cage and abdomen. Quiet sleep was defined as no eye movements, rare body or facial movements with occasional startles, and regular breathing with synchronised movements of the rib cage and abdomen.
A 7.5 MHz ultrasound transducer was used to obtain two dimensional images of the diaphragm at the level of the zone of apposition of the right hemithorax. The diaphragm was visualised in the right mid-axillary line at the level of the eighth or ninth intercostal space. Using the B mode, two dimensional coronal images of the diaphragm were generated and selected for clarity and parallelism of the three reflective layers of diaphragm structure (the muscle, pleural, and peritoneal membranes). At least five respiratory cycles were recorded and then replayed. We used the freeze frame control during the replay to precisely determine the end inspiration and end expiration. Diaphragm thickness (tdi) was measured as the distance between the midpoints of the peritoneal and pleural layers at end inspiratory volume (EIV) and end expiratory volume (EEV). The diaphragm thickness was measured to the nearest 0.1 mm, which is within the range of the accuracy of the transducer. All scans were performed by a single investigator (FDM). When repeated measurements were obtained for each infant at a given lung volume, the coefficients of variation for tdi were less than 10%. The reproducibility of tdi can be in part be attributed to studying the infants during quiet sleep where the breathing pattern is regular and the ultrasound images can be reviewed and recorded. Heart rate (HR), respiratory rate (f), and oxyhaemoglobin saturation (Sao 2) were measured continuously by a cardiorespiratory monitor (Datascope) and were recorded simultaneously during diaphragm imaging.
Diaphragm thickness and all physiological variables were recorded at end EEV and EIV in both positions. The change in tdi(Δtdi) during inspiration was calculated as the difference between tdi at EEV and at EIV. A pairedt test was used to determine the significance of differences in tdi and Δtdibetween the two positions. A p value of less than 0.05 was considered significant. All studies were approved by the Institutional Review Board of the Memorial Hospital of Rhode Island.
Results
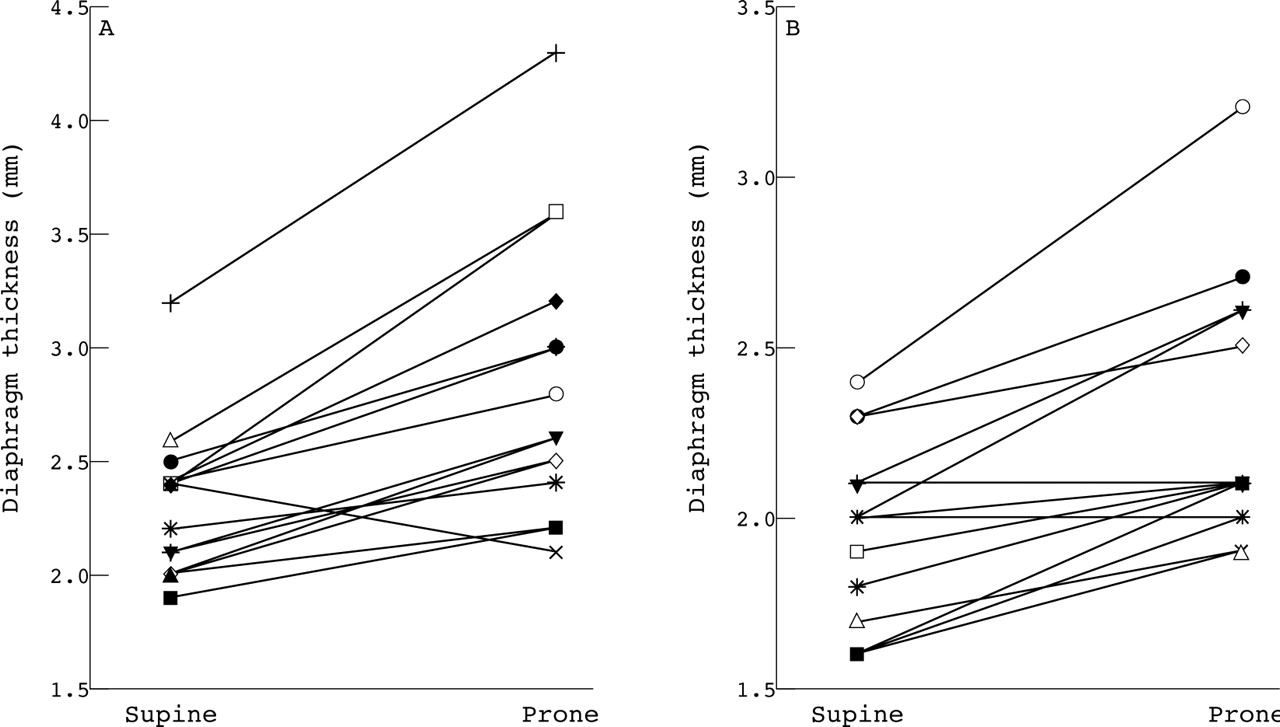
Table 2 presents the group mean values of tdi, Δtdi during inspiration, Sao 2, HR, and f for the supine and prone positions at EEV and at EIV. No differences in Sao 2, HR, and f were noted at either position or lung volume. The zone of apposition of the diaphragm to the rib cage was easily visualised and tdi measured in all infants (fig 1). Figure 2 shows individual values of tdi. In both positions, tdi is significantly greater at EIV than at EEV. This is not surprising as a normally functioning diaphragm thickens as it shortens during inspiration. However, the values of tdi were significantly greater in the prone position, both at EEV and at EIV (p < 0.01). When compared to the supine position, the diaphragm was 14% thicker at EEV and 23% thicker at EIV when the infants were prone. In addition, the change in tdi between EEV and EIV was greater in the prone position (30 (7)% v 20 (3)% for the prone and supine positions, respectively, p < 0.05). There were no differences in tdi or Δtdi between male and female infants in both sleep positions at either lung volume studied.
Physiological parameters, tdi, and Δtdi in supine and prone positions

Representative ultrasound image of the zone of apposition depicting the pleural, peritoneal, and muscular layers of the diaphragm at EEV.

{kind=link}
{kind=link}
Diaphragm thickness in individual patients in the supine and prone positions at end inspiratory lung volume (A) and at end expiratory lung volume (B). Data from each patient are paired.
From measurements of tdi in both positions, we calculated the difference in diaphragm muscle length at EEV between the prone and supine positions (see ). The ratio of diaphragm lengths in the prone and supine positions at EEV (ldiprone:ldi supine) is equal to the ratio of diaphragm thickness in the supine and prone positions (tdisupine:tdi prone). Thus, the 14% increase in tdi at EEV when the infant is prone represents a 13% shortening of the diaphragm. From measurements of Δtdi, we also calculated the relative difference in the change in diaphragm length during inspiration—that is, diaphragm shortening (Δldi prone:Δldi supine) during inspiration, between the prone and supine positions. Diaphragm shortening was, on average, 33% greater when the infant was prone.
Discussion
Sudden infant death syndrome continues to be the leading cause of infant mortality in developed countries.1 ,27 Recently, there has been considerable emphasis on infant sleep position as a predisposing factor for SIDS.1-9 Retrospective studies examining the link between sleep position and SIDS show that the prone sleep position has a consistent and strong association with SIDS. The likelihood ratios (relative risks or odds ratios) for SIDS with the prone sleep position compared to any other position have ranged from 1.3 to 11.3.2 The association between the prone sleep position and SIDS is further supported by the observation that the incidence of SIDS has been significantly reduced in countries that have instituted programmes aimed at reducing sleep time in the prone position (42% reduction in SIDS in the USA).1-4 7-9 ,27
Despite intense research, the aetiology of SIDS and the explanation of its association with the prone sleep position remain unknown. As the diaphragm is the major muscle of breathing in the neonate, we postulated that position induced alteration in diaphragm function may, in part, explain this association. We found that, in healthy term infants: (1) the zone of apposition of the diaphragm to the rib cage is readily visualised; (2) the diaphragm is significantly thicker at EEV when the infant is placed in the prone position; and (3) diaphragm thickening is greater during inspiration when the infant is prone. The latter two findings indicate that: (1) the resting length of the diaphragm is shorter in the prone position; and (2) during tidal breathing, the shortening of the diaphragm is greater in that position.
Differences in diaphragm configuration and rib cage anatomy between the newborn and adult have led investigators to postulate that the zone of apposition is minimal or even absent in the neonate.28However, we had no difficulty visualising the zone of apposition in these infants and found that on average it spanned two to three interspaces when measured at EEV. This finding indicates that the diaphragm is coupled to the chest wall, in healthy term infants, in a more advantageous way than previously thought. As the diaphragm descends, it raises gastric pressure in the area of apposition, which, in turn, is inflationary to the lower rib cage. Thus, the disordered chest wall motion noted in neonates may be owing to weakness of the intercostal muscles or to greater rib flexibility, rather than to the lack of a zone of apposition.
The greater tdi noted in the prone position cannot be accounted for by sampling error by the ultrasonographer. Firstly, the large width of the transducer head (5 cm) relative to the small infant chest wall allowed us to image the diaphragm over several interspaces. Over the range of interspaces sampled, there was uniformity of tdi in a given position. Secondly, we marked the external chest wall such that all measurements of tdi were made at the same external locations of the rib cage in the prone and supine positions. However, despite having the transducer at the same external location, it is possible that a different segment of the diaphragm was displaced under the transducer head when body position was changed.
Changes in diaphragm length can be inferred from measurements of changes in diaphragm thickness in the zone of apposition.29 The volume of the diaphragm muscle is the product of its length, perimeter, and thickness. As the volume of the diaphragm muscle remains constant during diaphragm shortening, length will vary inversely with thickness (see ). The group mean 14% increase in diaphragm thickness at EEV between the prone and supine positions (tdi prone:tdi supine × 100) indicates that the resting length of the diaphragm is 13% shorter when the infant is prone (ldi prone:ldi supine × 100). A similar degree of diaphragm shortening has been measured in canine diaphragm at EEV when the animal is prone.30 ,31This degree of diaphragm shortening is similar to that seen with an increase in lung volume of 15–30% of vital capacity.29Such increases in EEV can impair diaphragm performance. In adults, diaphragm strength and endurance as well as the efficiency of breathing are reduced by 40–50% with this magnitude of increase in lung volume.32
The mechanism for the increase in tdi in the prone position is not obvious. Differences in chest wall configuration, in the control of breathing between the two positions, and an increase in EEV could account for the thicker diaphragm when the infants were prone. An increase in EEV would shorten and thicken the diaphragm. However, the effects of the prone position on EEV are controversial. Large increases in EEV have been measured in anaesthetised adults,33whereas no change in EEV was measured in ventilated infants and children.34 Alternatively, a change in chest wall configuration, without a change in EEV, may account for this increase in tdi between the two positions. In support of this assertion, Sprung et al found that the diaphragm shortened in dogs placed in the prone position despite no change in EEV.31
In addition to being thicker at EEV, the diaphragm thickened more and, therefore, shortened more during inspiration (33% greater shortening during inspiration) when the infant was prone. This increased shortening may be owing to greater tidal volumes or to more chest wall distortion during inspiration. In support of the former mechanism, previous studies have shown that tidal volume increases and thoracoabdominal synchrony improves when healthy preterm and term infants are placed prone.35 ,36 Our study does not distinguish between these mechanisms. Others, however, have noted no change in tidal volume between the prone and supine positions in healthy preterm infants.19 ,37
The greater diaphragm shortening during inspiration when the infant was prone suggests that the work performed by the diaphragm was greater when the infants were in this position. The work accomplished when a muscle contracts is the integral of its tension over the distance it shortens, or, analogously for the diaphragm, the integral of transdiaphragmatic pressure over the volume displaced. In infants, the high chest wall compliance unopposed by inspiratory rib cage muscle activity often leads to paradoxical inward movement of chest wall during inspiration. Because of this disordered motion, there is less inhaled volume for a given degree of diaphragm shortening. In this instance, the diaphragm is performing more work than calculated from the measurement of tidal volume.38 ,39 Our method of measuring Δtdi during inspiration circumvents this limitation and provides an alternate means of assessing the work of breathing in infants. Assuming that transdiaphragmatic pressure was similar in both positions, we reasoned that diaphragm work per breath is increased when infants are prone. As the work of breathing increases, the oxygen cost of breathing increases and inspiratory muscle endurance decreases.32 We acknowledge that measurements of tidal volume or transdiaphragmatic pressure in these infants would have strengthened this conclusion.
In summary, we have established normal values for diaphragm thickness in healthy term infants and have shown significant differences in diaphragm thickness and the change in diaphragm thickness during inspiration between the supine and prone positions. Contrary to other physiological variables that have been measured, we found that the prone position in term infants is mechanically potentially disadvantageous to the diaphragm. We speculate that reduced mean operating length of the diaphragm in the prone position results in a less efficient and weaker diaphragm. A disadvantaged diaphragm combined with increased work of breathing in the prone position may impair an infant's response to respiratory stresses. In addition to previously proposed factors, our observations suggest the position induced diaphragm dysfunction may be another factor that may underlie the association between the prone sleep position and SIDS.1-3 9-17 ,27 How the diaphragm responds when challenged with respiratory stresses such as upper airway obstruction, hypoxia, or hypercarbia, and how the prone position alters diaphragm function in premature infants remain unknown and need further exploration.
Acknowledgments
This work was presented at the meeting of the American Thoracic Society, 23–28 April 1999, San Diego, California, USA.
Appendix
1) Comparison of diaphragm length (ldi) at EEV between the prone and supine positions.
mdisupine = tdisupine × pdisupine × ldisupine (Eq. 1)
mdiprone = tdiprone × pdiprone × ldiprone (Eq. 2)
where m, t, p, and l represent diaphragm mass, thickness, perimeter, and length. There was no change in chest perimeter between the supine and prone positions in these 16 infants. Assuming mass is constant.
ldi prone/ldisupine = tdisupine/tdiprone (Eq. 3)
2) Comparison of the change in diaphragm length during inspiration (Δldi) between the prone and supine positions. Taking derivatives of Equations 1 and 2, we obtain
Δldiprone = (−Δtdiprone/tdiprone)ldiprone (Eq. 4)
and
Δldisupine = (−Δtdisupine/tdisupine)ldisupine (Eq. 5)
The ratio of Δldiprone/Δldisupine is then
Δldiprone/Δldisupine = [(−Δtdiprone/tdiprone)ldiprone] / [(−Δtdisupine/tdisupine)ldisupine] (Eq. 6)
Since ldiprone/ldisupine = tdisupine/tdiprone (Eq. 3), substituting for ldiprone/ldisupine, we obtain Δldiprone/Δldisupine = Δtdiprone/tdisupine (tdisupine/tdiprone).2