Article Text

Abstract
Objective To evaluate clinical, audiological and neuroimaging findings in a cohort of infants diagnosed with congenital cytomegalovirus (cCMV) infection after failure at newborn hearing screening.
Methods A prospective observational study in the Netherlands, using the existing newborn hearing screening infrastructure for well babies. Between July 2012 and November 2016, cytomegalovirus (CMV) PCR testing of neonatally obtained dried blood spots (DBS) was offered to all infants who failed newborn hearing screening. Clinical, neuroimaging and audiological data were collected.
Results DBS of 1374 infants were successfully tested and 59 were positive for CMV (4.3%). Data of 54 infants were retrieved. Three were small for gestational age and six had microcephaly. Forty-eight (89%) had sensorineural hearing loss (SNHL), of whom half had unilateral SNHL. In both unilaterally and bilaterally affected children, the majority of the impaired ears had severe or profound hearing loss. Neuroimaging abnormalities were found in 40 of 48 (83%) children who had evaluable cranial ultrasound and/or cerebral MRI. The abnormalities were mild in 34, moderate in 3 and severe in 3 infants. The degree of SNHL and the severity of neuroimaging abnormalities were found to be correlated (p=0.002).
Conclusions The yield of targeted cCMV screening following newborn hearing screening failure was eight times higher than the estimated national birth prevalence of cCMV. The majority of this cohort of infants with clinically unsuspected cCMV disease had confirmed SNHL, neuroimaging abnormalities and lower than average birth weights and head circumferences. Newborns who fail newborn hearing screening should be tested for CMV to ensure appropriate clinical, neurodevelopmental and audiological follow-up.
- Virology
- Neuropathology
- Magnetic Resonance Imaging
- Paediatrics
- Audiology
Data availability statement
Data are available upon reasonable request. A dataset was generated and analysed and would be available upon reasonable request directly to the authors.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Congenital cytomegalovirus (cCMV) infection is the leading non-genetic cause of hearing loss. Targeted salivary cCMV screening within the newborn hearing screening programme is recognised as feasible and is implemented in some US states and trialled in other regions. Neuroimaging and clinical data of these limited cohorts are scarce.
WHAT THIS STUDY ADDS
Targeted dried blot spot screening for cCMV of infants who failed newborn hearing screening yields an eightfold increase of diagnoses (4.3%) compared with the general newborn population (0.54%). The majority (83%) of these infants with cCMV and sensorineural hearing loss show abnormalities on neuroimaging that are mostly mild. The severity of neuroimaging abnormalities and degree of hearing loss were found to be associated.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study shows that targeted dried blood spot screening following newborn hearing screening failure has a high yield. The results give insight in neuropathogenesis, support clinical care and will help guide decisions on implementation of cCMV screening.
Introduction
Congenital cytomegalovirus (cCMV) infection is the most common congenital infection worldwide and the leading cause of non-genetic hearing loss (HL).1 The birth prevalence in the developed countries is approximately 0.7%.2 The majority (90%) are born without clinically apparent disease, but approximately 13.5% of these ‘asymptomatic’ infants develop permanent sequelae such as sensorineural HL (SNHL) and developmental delay.2 3 One of the approaches to identify at-risk babies is targeted cytomegalovirus (CMV) screening after newborn hearing screening failure. Expedited cCMV diagnosis allows for possible antiviral treatment, as well as early assessment of potential neurological, developmental and ophthalmological sequelae. Previous studies exploring incorporated targeted CMV screening into newborn hearing screening programmes suggest favourable cost-effectiveness.4–8 While several reports of ongoing screening programmes offer insight into the feasibility of targeted screening, details on clinical, audiological and neuroimaging findings are scarce.9–14 In case of future implementation, clinicians could increasingly encounter infants with cCMV and seemingly isolated HL. More data on this patient population are needed to provide appropriate parental guidance on treatment and prognosis.
Therefore, the aim of this study is to describe the clinical, audiological and neuroimaging characteristics of a cohort of infants diagnosed with cCMV after failing newborn hearing screening. This targeted screening approach, in which CMV testing was performed on neonatally obtained dried blood spots (DBS), was carried out as part of the CONCERT Study, a non-randomised trial in which the effect of 6-week valganciclovir was compared with no treatment.
Methods
Study design and population
This observational study used the existing newborn hearing screening infrastructure for well babies in the Netherlands. Screening takes place in a maximum of three rounds: the first and second rounds using oto-acoustic emissions, the third round using automated auditory brainstem response (ABR) technology. After failing the third round, infants are referred to a regional audiology centre (AC). During the CONCERT trial, CMV testing was offered to all referred infants. The current study describes all cCMV-positive infants for whom written informed consent was obtained to retrieve baseline clinical data. The subgroup of infants eligible for inclusion in the trial had cCMV and SNHL, was aged <13 weeks, born at ≥37 weeks’ gestational age and had a birth weight >−2 SD.
CMV testing
Following informed consent, DBS were retrieved from the National Institute of Health and Environment. CMV PCR was performed on DBS sampled in the first week of life through routine heel prick screening. Using a whole blood spot (50 µL input volume), DNA was extracted using the Qiagen mini kit (from July 2012) or the Magna Pure 96 System (from July 2016). Next, a real-time CMV PCR assay with a detection limit of <500 IU/mL was performed in triplicate on each DBS as previously described.15 16 If at least one in three replicates was positive in the initial DBS, a confirmatory PCR was performed and similarly interpreted in a newly requested DBS sample.
Clinical, audiological and neuroimaging assessments
Following cCMV diagnosis, parents were informed of the possibility to participate in the CONCERT trial and advised to seek paediatric consultation regardless of participation. Trial subjects underwent screening, consisting of medical history taking, physical examination and laboratory assessments (complete blood count, liver and kidney function tests). Decisions on referral for neuroimaging and ophthalmological examination were left to the paediatrician. Audiological, ophthalmological, neuroimaging data and, if subjects were excluded from the CONCERT trial, clinical data, were retrieved from consulted specialists. Audiological assessments by regional ACs consisted of routinely performed click and/or tone burst ABR and tympanometry. Raw baseline data were reviewed by two experienced audiologists. The hearing threshold was determined as the lowest level with a peak V response. SNHL was defined as >20 dB perceptive unilateral or bilateral HL and categorised as follows: mild 21–40 dB, moderate 41–70 dB, severe 71–90 dB, profound >90 dB.17 Thresholds of ears with mixed perceptive and conductive HL were analysed as observed. Neuroimaging data were classified in blinded fashion according to the previously published Alarcon criteria18 by LSdV. All clinical centres used high-resolution cranial ultrasound (cUS) and MRI (1.5 or 3 Tesla) including sagittal and axial T1-weighted and T2-weighted images.
Statistical analysis
Birth weight and head circumference SD were derived using Growth Analyzer Research Calculation Tools (V.4.1, Growth Analyzer, Rotterdam, the Netherlands). Ordinal logistic regression analysis was used to examine the association between the degree of SNHL and neuroimaging abnormalities, as well as the relation between head circumference and neuroimaging abnormalities. In these analyses, mean hearing thresholds per ear for each patient were calculated. In case of normal hearing or conductive HL, the threshold was set at 10 dB. In case of profound HL without any measured responses, 110 dB was noted. Statistical analyses were performed with IBM SPSS software V.25.
Results
Study participants
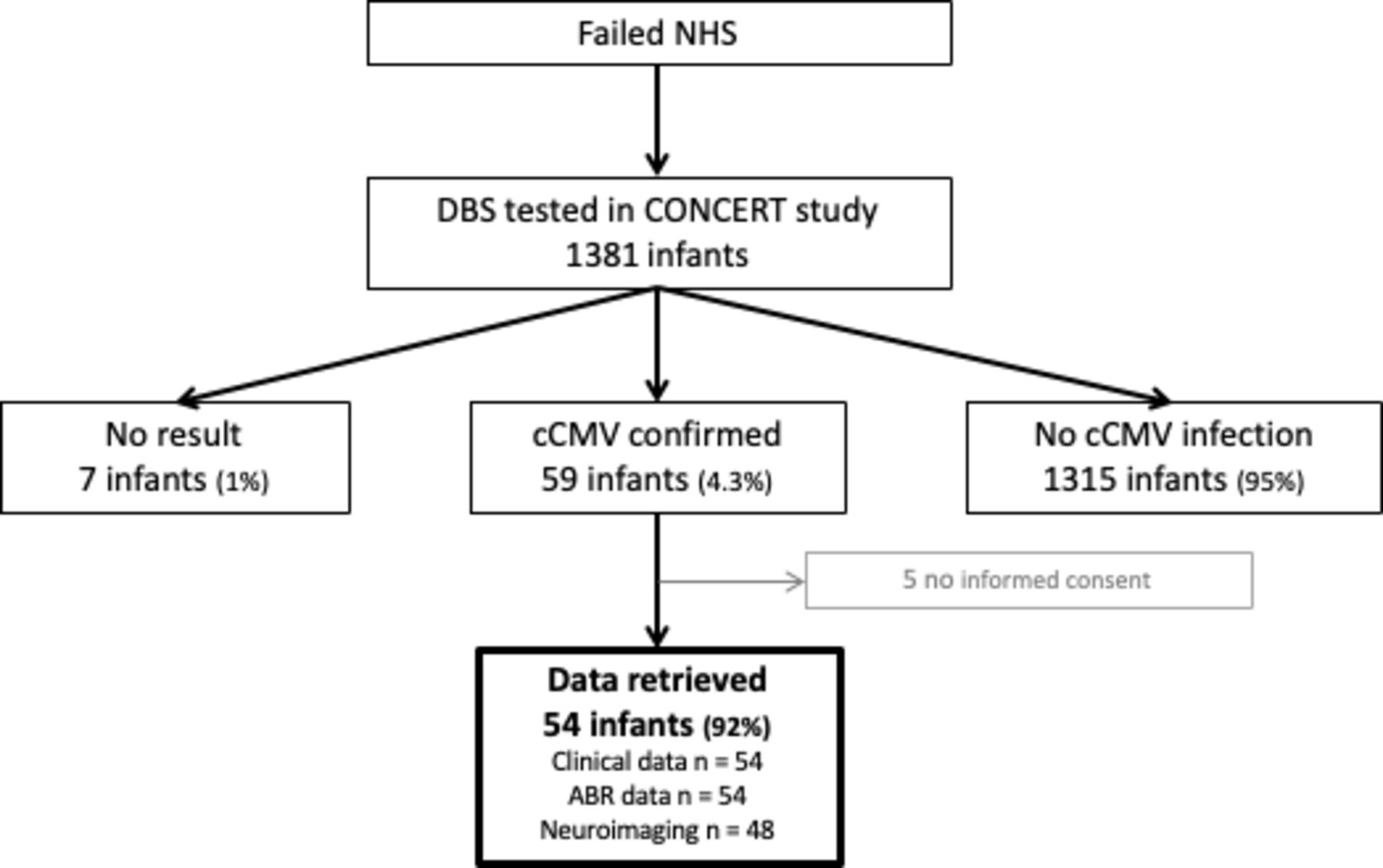
Between July 2012 and November 2016, 1381 children were enrolled for cCMV testing. PCR results of seven samples were not available: three due to insufficient blood, three due to internal PCR control failure and one due to sample loss. Of the 1374 DBS analysed, 59 were positive for CMV, yielding a cCMV prevalence of 4.3%. Informed consent for data retrieval was obtained for 54 of 59 infants (figure 1).

Enrolment of study participants. ABR, auditory brainstem response; cCMV, congenital cytomegalovirus; DBS, dried blood spot; NHS, newborn hearing screening.
Clinical and audiological characteristics
Gestational ages ranged from 32 to 42 weeks with two infants born preterm (32 and 36 weeks’ gestation) both with birth weights >−1 SD. Six infants had microcephaly (head circumference <−2 SD), with birth weights ranging from −2.19 to −0.17 SD (table 1). Our study population had significantly lower birth weights and smaller head circumferences compared with the general population (online supplemental figure 1). No ophthalmological abnormalities were found in the 33 infants examined. One infant had jaundice with elevated bilirubin levels (total bilirubin 212 µmol/L, direct bilirubin 185 µmol/L) and liver enzymes (aspartate aminotransferase 228 U/L; alanine aminotransferase 188 U/L) at the age of 15 days.
Supplemental material
Clinical and audiological characteristics of 54 infants with cCMV infection and failed newborn hearing screening
ABR results were evaluable in 54 infants at a median age of 37 days (IQR 27–51 days). Forty-eight (89%) were diagnosed with SNHL or mixed HL. Of these, 24 (50%) infants had bilateral HL. In the infants with bilateral HL, 34 ears (71%) were found to have severe or profound HL, and 20 (83%) infants with unilateral HL were diagnosed with severe or profound HL (table 1).
Neuroimaging
Neuroimaging was evaluable in 48 of 54 infants: cUS in 24, MRI in 6 and both in 18 infants. cUS was performed at a median age of 67.5 days (IQR 52–79 days), whereas the median age at MRI was 219 days (IQR 93–308 days) (figure 2). cUS was usually performed by radiologists and MRIs were performed in case of cUS abnormalities or cochlear implant (CI) indication.
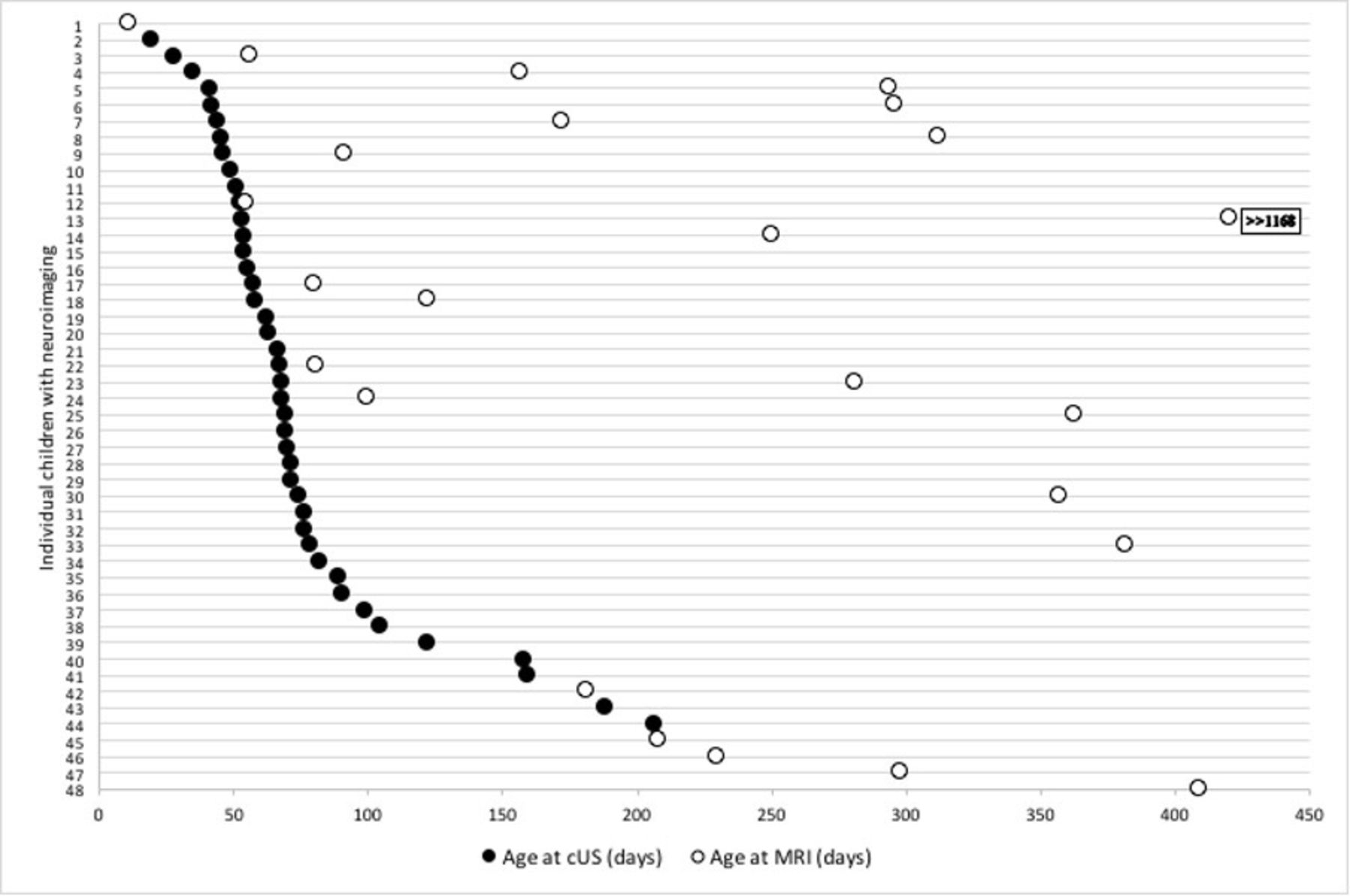
Age distribution at cUS and MRI investigations (n=48). cUS, cranial ultrasound.
Abnormalities were found in 40 of 48 children (83%); 34 (71%) had mild abnormalities (score 1), 3 (6%) had moderate (score 2) and 3 (6%) had severe abnormalities (score 3) (table 2). Moderate abnormalities included severe ventriculomegaly, temporal lobe involvement and diffuse white matter signal abnormalities. The severe abnormalities found were polymicrogyria in all three patients; one patient additionally showed extensive calcifications, atrophy and dysgenesis of corpus callosum.
Alarcon scoring and hearing data of 48 children with cCMV and evaluable neuroimaging
Four of the six infants with microcephaly (−3.88 to −2.02 SD) had Alarcon score 1 and two with head circumferences of −4.14 and −2.83 SD had polymicrogyria, resulting in Alarcon scores of 3. An association between head circumference and Alarcon score was found (figure 3A, p=0.002).

{kind=link}
{kind=link}
{kind=link}
Relationship between Alarcon score and (A) head circumference (n=46), and (B) sensorineural hearing loss (n=48).
SNHL was diagnosed in 44 of 48 children with evaluable neuroimaging and audiological data (table 2). An association was found between the severity of neuroimaging abnormalities and of SNHL (figure 3B, p=0.002). Correcting for mixed HL had no effect on the found correlation.
Discussion
To our knowledge, this is the first study to describe detailed data of a significant cohort of infants with cCMV detected through targeted screening. Furthermore, while targeted saliva screening is implemented and trialled in some regions, this is the first report of a nationwide targeted screening study using DBS. The prevalence of cCMV (4.3%) in our study population was eight times higher than the national birth prevalence of 0.54%,19 and the majority of infants were diagnosed with SNHL (87%). Previous newborn hearing screening-based screening studies report a cCMV prevalence between 0.6% and 4.7%, of whom 50%–83% had HL at the time of diagnosis.9 11 12 20 Our relatively high yield of both cCMV and confirmed HL cases may be explained by our sensitive three-round newborn hearing screening. In the Netherlands, 99.6% of all well babies are screened, of which 0.3% fail the newborn hearing screening. Of these, 35%–40% are diagnosed with unilateral or bilateral HL.21 Most European countries, the UK and USA report an newborn hearing screening fail rate between 1.5% and 2%, with confirmed HL in 5%–10%.22 A higher proportion of confirmed HL in a targeted screening population is likely to result in a higher detection rate of cCMV. Indeed, Rawlinson et al, who only included infants with confirmed HL in their targeted screening study, detected probable and definite cCMV in 5.6% of infants.23 The high percentage of children with confirmed HL could also in part be due to selection bias. Although we offered testing to all infants following newborn hearing screening failure and tested the majority of all referrals (60%), parents could have been more inclined to consent for CMV testing after HL confirmation at the AC. Unfortunately, audiological data from CMV-negative or CMV-untested newborn hearing screening fails were unavailable.
Eighty-three per cent of infants were found to have neuroimaging abnormalities on cUS and/or MRI, in most cases these were mild. Recent studies report imaging abnormalities of 0%–33% in ‘asymptomatic’ and 64%–76% in ‘symptomatic’ cCMV.24 25 Blazquez-Gamero et al found 69% cUS and/or MRI abnormalities in a cohort of 107 mostly ‘symptomatic’ (72%) subjects, while Lucignani et al reported 79.5% MRI abnormalities in a smaller cohort with 27 of 44 (61.3%) ‘symptomatic’ subjects.26 27 However, data on neuroimaging findings in infants with isolated HL are scarce. Hranilovich et al reviewed MRIs of a retrospective cohort diagnosed by targeted newborn hearing screening failure-based screening, describing one or more abnormalities in 10 of 17 patients (59%).28 Another study described 11 of 15 (73%) children as having abnormal MRI findings.23 The added assessments of cUS could explain our higher proportion of abnormal neuroimaging.
The use of the Alarcon score enabled us to examine the relation between the degree of neuroimaging abnormalities and SNHL at birth. The correlation found indicates that while infants with severe HL may also have mild imaging abnormalities, children with severe neuroimaging abnormalities are most likely to also have severe bilateral HL. Biologically, it makes sense that neuropathology following an intrauterine infection would lead to both more neuroimaging abnormalities and SNHL. Still, the majority of our considerable cohort with mostly severe SNHL have only mild neuroimaging abnormalities. Apart from microcephaly in six infants, none showed neurological abnormalities at birth. Thus, severe HL does not necessarily imply severe neuroimaging abnormalities and a subsequent adverse neurodevelopmental prognosis. This is noteworthy, since the presence of SNHL could be expected to result from vertical CMV transmission during the first trimester of pregnancy.29–33 Our findings suggest that early vertical transmission more often leads to isolated inner ear disease than widespread central nervous system (CNS) pathology. Preclinical pathogenesis studies are needed to explore this research gap.
Our study has limitations. First, because CMV testing was part of a trial, our study population does not reflect a hypothetical nationwide targeted screening cohort. Our population may be skewed towards term babies of normal birth weight, due to the inclusion criteria of the CONCERT trial, although the current study does include subjects excluded from the trial. Second, we performed CMV testing on DBS, rather than urine or saliva, the gold standard used in earlier targeted screening studies. Although PCR on DBS is less sensitive than on urine or saliva, we estimate that our DBS procedure has a sensitivity of at least 84% and a specificity of 99.9%.34 With a prevalence of around 5% in this cohort, the positive and negative predictive values are 98% and 99%, respectively. Moreover, using DBS has obvious advantages in our unique local setting. In the Netherlands, there is a high homebirth rate and an infrastructure for maternity care at home for well babies. As a result, both hearing screening and heel prick testing are routinely performed at home, making saliva or urine collection impractical and DBS a convenient alternative for incorporating targeted screening into existing programmes. In addition, since we chose to enrol after third round failure, which increases yield and reduces cost, many infants would have been missed if testing was due within 21 days. Indeed, in our cohort, informed consent for CMV testing was obtained within 21 days in only 35% of infants.
Finally, the main limitation of our study is the fact that infants were not subjected to a standardised neuroimaging protocol, resulting in lack of MRI data and different timing of imaging if both modalities were performed, MRI having been performed at a much later age. White matter signal intensity abnormalities have been reported to become less apparent over time,35 36 although the prognostic value of isolated white matter abnormalities for long-term sequelae is still debated.37 In the 24 infants who only underwent cUS, abnormalities such as migrational disorders and white matter abnormalities may have been missed. This may have led to an underestimation of CNS abnormalities in our study. A recent study found 93 of 480 (19%) children with cCMV with normal cUS to have abnormal findings on MRI.38 Conversely, the lack of an imaging protocol may have also led to selection bias towards a more severely affected group as the subgroup of patients with an MRI had abnormalities on cUS or an indication for CI placement. More data are needed in similar cohorts of isolated SNHL, in which both cUS and MRI are performed in a standardised protocol, preferably shortly after birth.
Conclusions
This is the largest and most clinically detailed account of a targeted screening cohort of infants with cCMV. The majority in our cohort had confirmed SNHL, neuroimaging abnormalities and lower than average birth weights and head circumferences. A high prevalence of neuroimaging abnormalities in infants with CMV and HL could have therapeutic consequences as the current consensus is to start antiviral treatment in case of CNS involvement, although the definition of CNS involvement regarding mild abnormalities is still under debate.39 Long-term studies using both cUS and MRI are needed to determine the clinical consequences of these imaging abnormalities and treatment benefits in this subpopulation. In the meantime, these findings underscore the need for appropriate follow-up in infants with cCMV and seemingly isolated HL.
An early diagnosis of cCMV as the cause of HL will improve parental counselling, while raising awareness of possible neurodevelopmental sequelae and facilitating timely hearing and language rehabilitation. Consequently, newborns who fail newborn hearing screening should be tested for CMV.
Data availability statement
Data are available upon reasonable request. A dataset was generated and analysed and would be available upon reasonable request directly to the authors.
Ethics statements
Patient consent for publication
Ethics approval
The CONCERT trial (ClinicalTrials.gov: NCT02005822) was approved by the Medical Ethical Committee of the Leiden University Medical Center (Study P13.168, File nr: NL45593.058.13). Informed consent was requested for CMV diagnostics after newborn hearing screening failure and before clinical trial participation. In addition, written informed consent for data retrieval for the current study was requested from parents or legal guardians of all cCMV-positive infants.
Acknowledgments
We are grateful to all parents who gave consent for CMV diagnostics in the CONCERT Study. We thank all cooperating region coordinators of the newborn hearing screening programme, for informing parents of newborn hearing screening-referred infants about the availability of CMV diagnostics; the Department for Vaccine Supply and Prevention Programs at the National Institute for Public Health and the Environment for providing the DBS cards; and Dick Biesheuvel for his advice and contribution in extracting audiological data. Finally, we acknowledge the hard work of Lisette Rusman and Caroline de Brouwer in testing the dried blood spots.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
PKC and FS contributed equally.
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors PKC and FS contributed equally to this work. PKC carried out the analyses and drafted the manuscript. FS conceptualised and designed the study, collected data, carried out the analyses, reviewed and revised the manuscript. AV acted as guarantor, conceptualised and designed the study, supervised data collection, reviewed and revised the manuscript. AMO-M conceptualised and designed the study and reviewed and revised the manuscript. LSdV assessed neuroimaging data and reviewed and revised the manuscript. WS assessed audiological data and reviewed and revised the manuscript for audiological content. EvZ provided statistical support and revised the manuscript for statistical content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This study was Supported by Fonds NutsOhra (project number 0901-054).
Competing interests The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper. The authors declare the following non-financial interests/personal relationships which may be considered as potential competing interests: AMO-M is a member of the national advisory board on newborn hearing screening, which is an unpaid function.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.