Article Text

Abstract
Objective We aimed to describe long-term outcomes following hypoxic–ischaemic encephalopathy (HIE) treated with therapeutic hypothermia (TH).
Design Prospective, population-based observational study.
Setting Tertiary level neonatal intensive care units and neonatal outpatient clinic, Karolinska University Hospital, Stockholm, Sweden.
Patients Sixty-six infants treated with TH due to HIE between 2007 and 2009.
Interventions At 6–8 years and 10–12 years of age, children were assessed using a standardised neurological examination, the Movement Assessment Battery for Children, Second Edition (MABC-2) and the Wechsler Intelligence Scales for Children IV/V. Parents completed the Five-to-Fifteen (FTF) questionnaire.
Main outcome measures Adverse outcome among survivors was defined as cerebral palsy (CP), epilepsy, hearing or visual impairment, full-scale IQ (FSIQ) below 85, attention deficit disorder with/without hyperactivity, autism spectrum disorder or developmental coordination disorder.
Results Mortality was 12%. Seventeen per cent of survivors developed CP. Mean FSIQ was normal in children without major neuromotor impairment. Assessment in early adolescence revealed emerging deficits in 26% of children with a previously favourable outcome. The proportion of children exhibiting executive difficulties increased from 7% to 19%. This was reflected also by a significantly increased proportion of children with an FTF score >90th percentile compared with norms in early adolescence. The proportion of children with an MABC-2 score ≤5th percentile was also significantly increased compared with norms.
Conclusions Survivors without major neuromotor impairment have normal intelligence. The incidence of executive difficulties appears to be increased in this patient population. More subtle difficulties may go undetected at early school-age.
- child development
- neonatology
- neurology
- paediatrics
Data availability statement
Data are available on reasonable request. Deidentified participant data, data dictionary, study protocol, participant and parental letter of information and written consent form are available to investigators whose proposed use of the data has been approved by an independent ethics review committee for this purpose.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Therapeutic hypothermia reduces the risk of death or severe disability at 18–24 months of age in near-term/term infants with moderate to severe hypoxic–ischaemic encephalopathy (HIE).
From the pre-hypothermia era, it is known that a significant proportion of survivors free of major neuromotor disability suffers more subtle cognitive impairments and/or executive difficulties.
Among survivors free of cerebral palsy, a substantial proportion is at increased risk of general and/or specific cognitive impairment at early school-age despite therapeutic hypothermia.
WHAT THIS STUDY ADDS
Outcomes among children with a history of moderate HIE remain heterogeneous also in the era of therapeutic hypothermia.
Most survivors free of major neuromotor impairment have normal intelligence.
More subtle impairments may go undetected when assessments are done around early school-age, and the incidence of executive difficulties appears to be increased in this vulnerable patient population.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Further research is needed to elucidate the effects of therapeutic hypothermia on neurodevelopmental and cognitive outcomes in adolescence and adulthood.
Background
Therapeutic hypothermia (TH) is standard of care in near-term/term infants with moderate/severe hypoxic–ischaemic encephalopathy (HIE) in most high-resource settings. Contemporary studies have reported lower incidences of death or cerebral palsy (CP) compared with the major randomised controlled trials (RCTs) on TH.1 2 However, evidence suggests that a substantial proportion of survivors without major neurodisability still experiences impairments at early school-age.3–6 Attention and visuospatial function have been demonstrated to be poorer among survivors without CP compared with healthy peers.7 Neither motor difficulties4 8 nor attention, memory or behavioural problems4 9 are necessarily evident during early assessments in survivors of hypothermia-treated HIE without CP. MRI studies have demonstrated affected brain connectivity in children without CP following hypothermia-treated HIE.10 11 Around early adolescence, as academic and social load increases, children with previously apparent normal development following an early brain insult may present with emerging deficits or fail to make expected developmental gains.12 To date, no studies have investigated outcomes following hypothermia-treated HIE beyond early school-age.13
Here, we describe neurological, neuromotor, cognitive and developmental outcome at early school-age and in early adolescence in a regional, population-based clinical cohort of children with hypothermia-treated HIE.
Material and methods
Patients and setting
This study included all infants (gestational age (GA) ≥34+0 weeks) treated with TH due to HIE in the greater Stockholm catchment area from January 2007 to December 2009. The two tertiary-level neonatal intensive care units (NICUs) at Karolinska University Hospital serve as regional TH centres where all infants meeting treatment criteria for TH are funnelled.
Hypothermia treatment
Amplitude-integrated EEG (aEEG) was not mandatory to commence TH (online supplemental table 1). Systemic hypothermia of 33.5°C for 72 hours followed by slow rewarming was achieved using a Thecoterm® mattress (TecCom, Halle, Germany) or a CritiCool® suit (Mennen Medical, Rehevot, Israel). HIE severity was assessed throughout TH with the Sarnat and Sarnat staging and the Thompson score.14–16
Supplemental material
Procedure for follow-up
After obtaining written parental consent, assessments were performed in our outpatient clinic. If a child had undergone psychometric testing at 6–8 and 10–12 years of age elsewhere, we did not readminister the test but reviewed the results after obtaining parental permission. A questionnaire response was requested from the parents.
Neurological and neuromotor assessment
A paediatric neurologist took a detailed medical history, including information on any formal diagnosis of visual/hearing impairment, autism spectrum disorder (ASD),17 attention deficit disorder with/without hyperactivity (ADD/ADHD),17 developmental coordination disorder (DCD),17 18 epilepsy or CP and performed a structured neurological examination. A physiotherapist assessed motor functions using the Movement Assessment Battery for Children, Second Edition (MABC-2)19 which consists of three subscales: Manual dexterity, Aiming and catching and Balance. Each domain gets a standard score and percentile equivalents and is compared with normative data. A total test score ≤5th percentile indicates significant motor difficulty, whereas a total test score between the 6th and 15th percentile indicates a child at risk of motor difficulty. A total test score >15th percentile is considered normal.19 Assessors were not blinded to the neonatal course.
Psychometric assessment
A psychologist blinded to previous medical history assessed cognitive abilities using the Swedish versions of the Wechsler Intelligence Scales for Children, Fourth Edition (WISC-IV, Wechsler, 2003, 2007) at age 6–8 years and the Wechsler Scales of Intelligence for Children, Fifth Edition (WISC-V, Wechsler, 2014) at age 10–12 years. Both versions yield a full-scale IQ (FSIQ). Results are expressed as an age-standardised score, with a population mean of 100 and a SD of 15. An FSIQ<70 constitutes one of the diagnostic criteria for intellectual disability.17 An FSIQ between 70 and 84/85 is considered borderline intellectual functioning (BIF).17 For children unable to complete sections of the WISC-IV/V due to physical impairments, results are reported separately.
Other assessments
Parents completed the Five-to-Fifteen questionnaire (FTF/FTF revised form)20 to screen for developmental and behavioural disorders. It comprises 181 items divided into eight domains: Motor skills, Executive functions, Perception, Memory, Language, Learning, Social skills and Emotional/behavioural problems. The FTF has been normed for Swedish children aged 5–15 years and has good reliability and validity.21–24 It has been used in a stratified sample of Swedish children from the general population, and medians, means, 75th, 90th and 98th percentiles for domain scores have been published for boys and girls.21 25 The 90th and 98th percentile are used as a cut-off for obvious difficulties and severe/major difficulties, respectively.
Ethics considerations
This study has been approved by the appropriate Ethics Review Board in Sweden (2009/735-31/4, 2016/1921-32, 2019-01447).
Data collection
Demographic and perinatal data were retrieved from the electronic obstetric medical records. Neonatal data were retrieved from the patients’ electronic medical records. After approval from the Ethics Review Board, the children in our cohort were invited for assessment at ages 6–8 and 10–12 years.
Study outcomes
The primary outcome in our study was survival without neurological abnormalities (defined as an FSIQ score ≥85, a normal neurological examination, normal hearing, normal vision, no ASD/ADD/ADHD/,17 no DCD17 18 and no epilepsy). We also investigated the incidence of CP, ADD/ADHD, ASD and DCD.
Statistical analysis
Normality was tested with Kolmogorov-Smirnoff’s test. Normally distributed variables are presented as mean with SD, and variables with skewed distributions are presented as median with IQR. When comparing the proportion of children with an MABC-2 score ≤15th or ≤5th percentile or an FTF score >90th percentile to norms, we used a binomial test. McNemar test was used to investigate if the proportion of children with an abnormal MABC-2 score differed significantly between the two assessment occasions. A two-sided p-value <0.05 was considered statistically significant for all analyses. Analyses were done using GraphPad Prism V.9.3.1 for macOS (GraphPad Software, San Diego, California, USA; www.graphpad.com) or SPSS V.27.0 for Windows (IBM, Armonk, New York, USA).
Results
Neonatal outcome
Between January 2007 and December 2009, 66 infants with HIE underwent TH at Karolinska University Hospital. Baseline patient characteristics are summarised in table 1. Two infants had suffered a postnatal collapse shortly after delivery. Four infants were born late preterm (at 34+0, 35+1, 35+3 and 35+6 weeks’ GA, respectively). Four infants with Sarnat stage 1 HIE had been treated with TH. Active TH was initiated after 6 hours of age in three infants passively cooled following fulfilled A-criteria due to the onset of seizures. Seven infants died after discontinuation of intensive care due to the estimated poor prognosis, bringing the neonatal mortality to 10.6%. Fifty-nine infants survived to discharge from the NICU. One child was excluded from further analyses due to a genetic syndrome.
Patient demographic characteristics (N=65)
Long-term outcome assessments
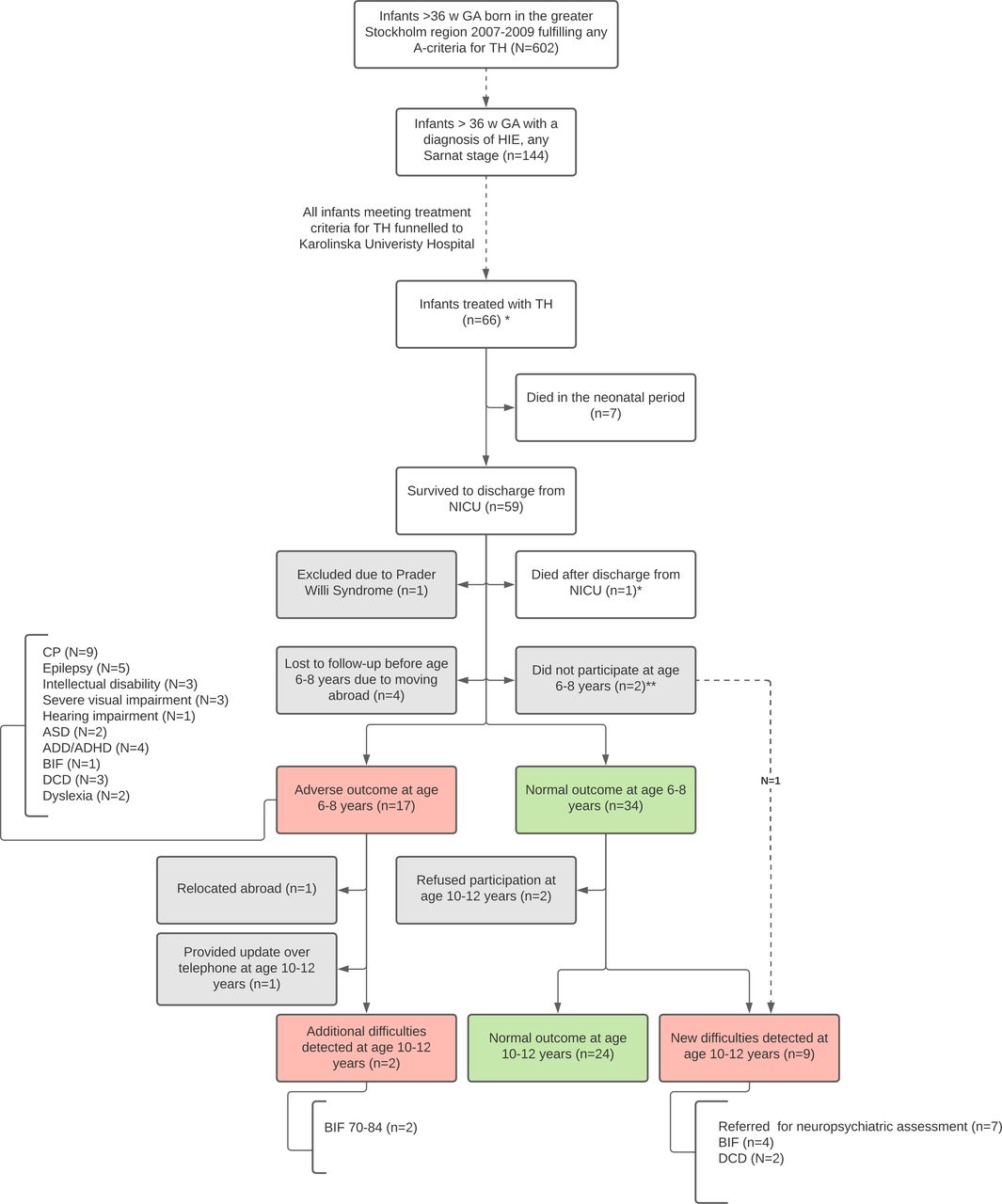
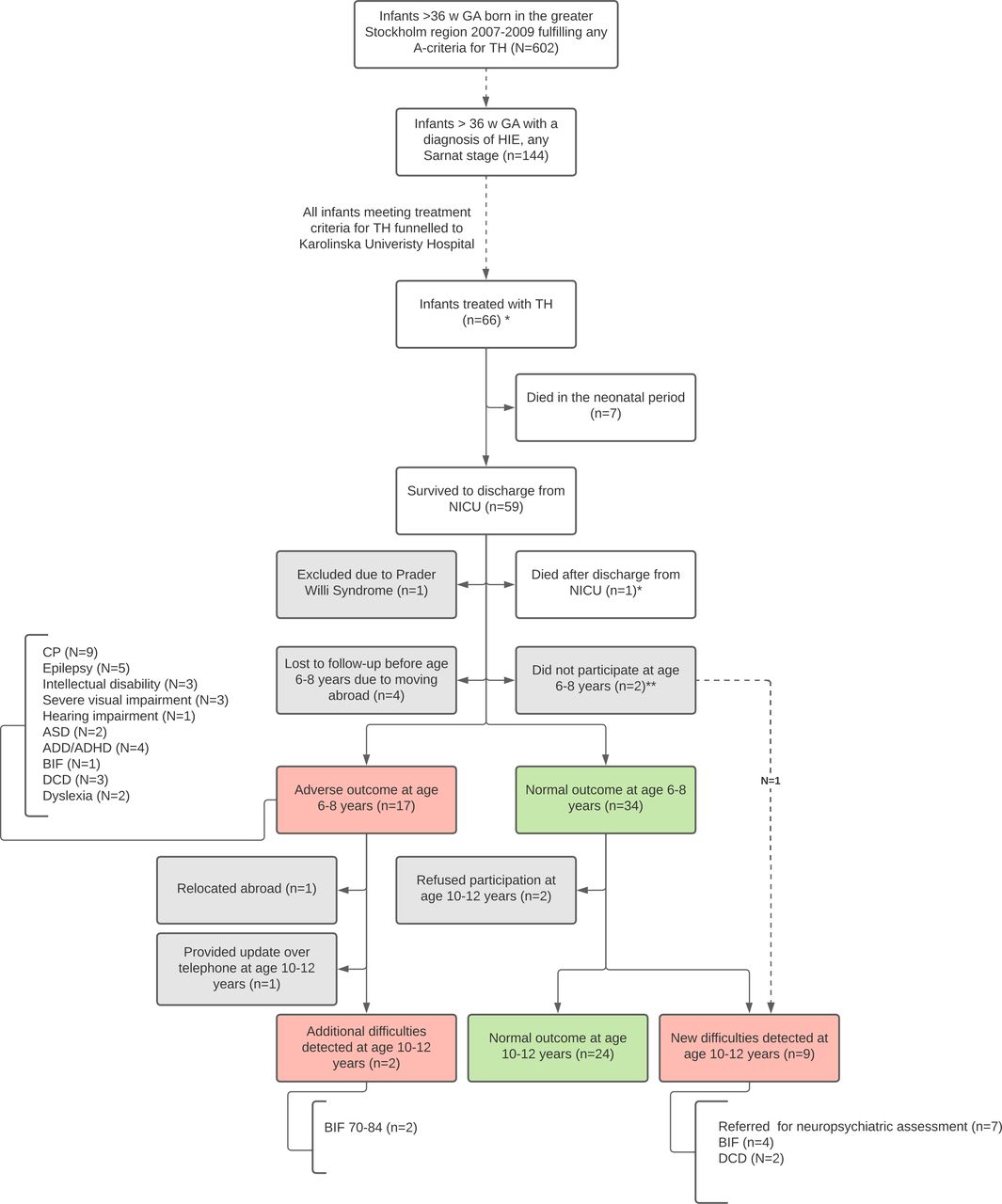
Mean age at the first and second assessment was 7.4 years (SD=0.7 years) and 11.2 years (SD=0.7 years), respectively. Outcome was known for 59 children (91%) at early school age, and for 57 children (88%) in early adolescence. Figure 1 provides an overview of outcomes. Table 2 summarises outcomes in relation to worst Sarnat stage of HIE on day 1 of life.
{kind=link}
Flow chart outlining long-term outcomes among children included in the study. *The cohort described in the present study includes all infants treated with TH due to HIE in the greater Stockholm region between 2007 and 2009. A joint protocol for TH was accepted in the region prior to implementation of TH in regular clinical practice. The level III NICUs at Karolinska University Hospital serve as regional TH centres where all infants meeting criteria for TH treatment are funnelled. * Child with severe CP, ad mortem at 1 year of age. ** Two survivors still residing in Sweden did not participate in the assessment at 6-8 years of age. One of them had been assessed at 5.5 years of age in accordance with new national Swedish guidelines and had normal outcome at that time, but exibited emerging deficits when assessed at 10-12 years of age. Our cohort also includes four infants with Sarnat stage I HIE and four infants born late preterm who received TH. ADD, attention deficit disorder; ADHD, attention deficit hyperactivity disorder; ASD, autism spectrum disorder; BIF, borderline intellectual function; CP, cerebral palsy; DCD, developmental coordination disorder; GA, gestational age; HIE, hypoxic–ischaemic encephalopathy; NICU, neonatal intensive care unit; TH, therapeutic hypothermia.
Overview of long-term outcome in relation to Sarnat stage of HIE in all children for whom outcome was known (overlap between diagnoses is possible)
Neurological outcome
Among participants surviving to discharge from the NICU, 10 (17%) developed CP. One child with CP and epilepsy died at age 1, bringing the total all-cause mortality to 12%. HIE severity, subtypes of CP, Gross Motor Function Classification System (GMFCS) level, neuroimaging findings, Bayley Scales of Infant and Toddler Development, Third Edition motor score percentiles and neurological comorbidities are described in table 3.
Subtype, severity and age at formal diagnosis in children with cerebral palsy
Among survivors without CP, three children (6%) had a diagnosis of DCD at early school age. By early adolescence, two more children were diagnosed with DCD, bringing the incidence to 10%. The proportion of children scoring ≤5th percentile on MABC-2 was significantly increased compared with norms at both assessments. At early school age, 11 (25%) of the 44 children had an MABC-2 score ≤15th percentile. In early adolescence, this increased to 13 (30%) which is significantly higher compared with norms (p<0.006) (online supplemental table 2).
Supplemental material
Developmental outcome and FTF questionnaire findings
At early school age, six children without CP had other difficulties affecting everyday life. Three children had a diagnosis of ADHD, one of them also had dyslexia and one also had DCD. One child had ASD. One child had profound bilateral hearing loss. One child had unilateral blindness. On repeated assessment in early adolescence, executive difficulties were evident in seven more children. At early school age, the results of the FTF questionnaire were unremarkable compared with norms. In early adolescence, the proportion of children with a score >90th percentile was significantly increased compared with norms within the Motor skills, Executive functions, Perception, Memory and Language domains (online supplemental table 3).
Supplemental material
Cognitive outcome
At early school age, 46 children completed WISC-IV. Mean FSIQ was 104 (SD 10.8, 95% CI 100.8 to 107.2). Mean index scores were all within normal range (table 4). One child with ADHD and dyslexia had BIF. In early adolescence, 45 children completed WISC-V. Mean FSIQ was 100.9 (SD 16.3, 95% CI 96 to 105.8). Mean index scores were all within normal range (table 5). Online supplemental figure 1 illustrates distribution of FSIQ scores.
Supplemental material
WISC-IV results on a group level
WISC-V results on a group level
In early adolescence, two children with previous diagnoses (ADHD and DCD in the case of one child, and CP, cortical visual impairment and epilepsy in the case of the second child) were found to have BIF. Furthermore, four children with favourable outcome at early school age now had BIF. The number of children with BIF thus increased from 1 (2%) to 7 (12%) by early adolescence.
One child with CP (GMFCS 5) and cortical visual impairment took the tests with the aid of an assistant, revealing a cognitive ability equivalent to 2–3 years below the chronological age. Another child with CP (GMFCS 3) was not able to complete all included tests, but those that could be completed indicated normal intelligence. Three children with CP (GMFCS 1) had results within normal range on both occasions.
Discussion
In this study, a considerable proportion of children with a history of hypothermia-treated HIE and seemingly favourable outcome at early school age exhibited emerging deficits by early adolescence. We found a high incidence of executive difficulties. Overlap of multiple diagnoses was common also among children with impairments other than moderate/severe CP. Our incidence of CP was lower than the TOBY trial (21%)26 but similar to the NICHD trial (17%).27 The lower mortality rate in our cohort compared with these RCTs (29% and 26%, respectively)26 27 may possibly be explained by the smaller proportion of infants with Sarnat stage III HIE. Compared with more contemporary clinical HIE cohorts, mortality rate1 2 and incidence of CP2 were similar. Surprisingly, 40% of children with CP in our cohort had unilateral spastic CP, raising suspicion of an aetiology other than HIE. However, they had all met treatment criteria for TH with clinical and biochemical findings consistent with perinatal asphyxia. One of these children had suffered a neonatal stroke in addition to asphyxia. The proportion of children with an MABC-2 score ≤5th percentile was significantly increased compared with norms both at early school age and in early adolescence. However, the proportion of children scoring ≤15th percentile was significantly increased compared with norms only in early adolescence. A recent study reported similar findings of MABC-2 scores ≤15th percentile in 38% of school-age children without CP following hypothermia-treated HIE.8 Mean FSIQ and all mean index scores were normal among survivors without major neurodisability. We chose to use the most recent WISC version (WISC-V) at the assessment in early adolescence with the Flynn effect in mind.28 In a Swedish sample of children assessed with both the WISC-V and WISC-IV, the adjusted correlation for the primary index scores and FSIQ was high between the two instruments (WISC-V; Wechsler, 2014). It is important to note that in WISC-V, the influence of the Processing speed index and Working memory index on FSIQ is smaller compared with WISC-IV. While WISC mean index scores were within normal range, we observed relatively lower scores within Working memory and Processing speed. Interestingly, the healthy peers recruited in the Swedish ExPRESS study exhibited a similar pattern at 6.5 years of age.29 Results of the FTF were unremarkable at early school age. By early adolescence, however, the proportion of children with an FTF score indicating obvious difficulties was significantly increased compared with norms within several domains that may impact educational outcomes. This finding aligns with the number of children exhibiting executive difficulties increasing from 4 (7%) to 11 (19%) between assessments, which appears to be higher compared with the general population. Most children with executive difficulties that became apparent only in early adolescence did not exhibit hyperactivity, which may partially explain why these difficulties had previously remained undetected. Also, we speculate that cognitive abilities within normal range may further contribute to masking of executive difficulties. With increasing academic and social demands, however, these deficits may become increasingly apparent.12 Tonks et al have demonstrated affected dorsal stream functions including attention difficulties and reduced visuospatial processing among school-age survivors of hypothermia-treated HIE without CP.7 Furthermore, school-age children without CP following treatment with TH due to HIE were demonstrated to have disrupted brain connectivity on diffusion-weighted MRI.10 Previous studies have shown that less overt motor and cognitive deficits at school age are not predicted by developmental scores at 18 months.8 30 Our findings suggest that more subtle deficits may go undetected also at early school-age. Failing to make age-appropriate developmental gains as environmental demands increase, despite exhibiting apparent normal functioning earlier post-insult, has been described also in other cohorts of children with acquired brain injury.31
Limitations of our study include small sample size, and our results may therefore not be fully generalisable. However, our cohort includes all infants treated with TH due to HIE in Stockholm during 2007–2009. HIE severity staging might have been more robust if aEEG had been mandatory for initiation of TH. Our cohort also includes infants treated with TH outside of the protocol; four infants with Sarnat stage I HIE, four late-preterm infants and three infants for whom active TH was initiated at >6 hours of age. Further limitations include the lack of a control group and incomplete blinding of all assessors. Outcomes were, however, contrasted with the normative samples of the respective test. We could not adjust for the parental level of education or diagnosis of ASD/ADD/ADHD due to lack of information.
Strengths of the current study include its population-based, prospective design. Standardised assessments using validated instruments were performed by the same experienced team on both occasions. The participation rate among survivors residing in Sweden was very high.
In summary, we found a similar mortality rate and incidence of CP compared with other contemporary HIE cohorts. Mean FSIQ was normal among survivors without major neurodisability. A considerable proportion of children apparently unaffected at early school age subsequently exhibited emerging deficits in early adolescence. Outcomes after moderate HIE remain heterogeneous also in the era of TH.
To the best of our knowledge, this is the first study to report outcomes in early adolescence following HIE treated with TH. Further long-term outcome studies are needed in this vulnerable patient population. We advocate for extended follow-up, also in the absence of major sequelae, to enable the identification of children who may benefit from intervention.
Data availability statement
Data are available on reasonable request. Deidentified participant data, data dictionary, study protocol, participant and parental letter of information and written consent form are available to investigators whose proposed use of the data has been approved by an independent ethics review committee for this purpose.
Ethics approval
This study involves human participants and was approved by the Stockholm Ethics Review Board and the Swedish Ethical Review Authority (2009/735-31/4, 2016/1921-32, 2019-01447). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors wish to thank all the children and families who participated in the study, as well as research nurses Michaela Melakari and Camilla Halzius for their assistance. We also wish to thank Dr Ingrid Ekström and Professor Mikael Norman for their valuable contributions.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Correction notice This article has been corrected since it was first published. The open access licence has been updated to CC BY.
Contributors KRG, MEW, MB and KL conceptualised and designed the study. KRG, MEW and MB acquired funding for the study. All authors performed repeated literature searches and agreed on methodology. KRG was responsible for the administration of the project. KRG, MEW and KL conducted the investigations. MB and KL supervised the project. KRG, MEW and KL performed data curation, verified the collected data and performed the formal statistical analyses. KRG wrote the original draft and revised the manuscript after review by MEW, KL and MB. KRG is guarantor.
Funding This work was supported by H.K.H. Kronprinsessan Lovisas Förening för Barnasjukvård/Axel Tielmans Minnesfond (grant no 2020-00587) and grants provided by Region Stockholm: ALF project (grant no 510097) and Centre for Innovative Medicine (project no H9641193).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.