Article Text

Abstract
Objective The effect of prophylactic surfactant nebulisation (SN) is unclear. We aimed to determine whether prophylactic SN improves early lung aeration.
Design Parallel, randomised clinical trial, conducted between March 2021 and January 2022.
Setting Delivery room (DR) of a tertiary neonatal centre in Zurich, Switzerland.
Patients Preterm infants between 26 0/7 and 31 6/7 weeks gestation
Interventions Infants were randomised to receive positive distending pressure alone or positive distending pressure and additional SN (200 mg/kg; poractant alfa) using a customised vibrating membrane nebuliser. SN commenced with the first application of a face mask immediately after birth.
Main outcome measures Primary outcome was the difference in end-expiratory lung impedance from birth to 30 min after birth (∆EELI30min). EELI correlates well with functional residual capacity. Secondary outcomes included physiological and clinical outcomes.
Results Data from 35 infants were collected, and primary outcome data were analysed from 32 infants (n=16/group). Primary outcome was not different between intervention and control group (median (IQR): 25 (7–62) vs 10 (0–26) AU/kg, p=0.21). ∆EELI was slightly higher in the intervention group at 6 and 12 hours after birth, particularly in the central areas of the lung. There were no differences in cardiorespiratory and clinical parameters. Two adverse events were noted in the intervention group.
Conclusions Prophylactic SN in the DR did not significantly affect ∆EELI30min and showed only minimal effects on lung physiology. Prophylactic SN in the DR was feasible. There were no differences in clinical outcomes.
Trial registration number NCT04315636.
- intensive care units, neonatal
- neonatology
- resuscitation
Data availability statement
Data are available upon reasonable request. Deidentified individual participant data will be made available from three months to three years following publication, in addition to study protocols, the statistical analysis plan, and the informed consent form to researchers who provide a methodologically sound proposal, with approval by an independent review committee (“learned intermediary”). Data requestors will need to sign a data access or material transfer agreement approved by USZ. Proposals should be submitted to vincent.gaertner@usz.ch to gain access.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Surfactant nebulisation (SN) is a promising non-invasive route of surfactant application in preterm infants.
SN may be effective in preventing intubation in preterm infants with established respiratory distress syndrome, but the effect of prophylactic SN immediately after birth is unclear.
WHAT THIS STUDY ADDS
Prophylactic SN did not improve aeration and ventilation homogeneity as well as clinical outcomes.
Lung aeration was slightly increased after prophylactic SN at 6 and 12 hours after birth, particularly in the central areas of the lung.
Performing SN as well as continuous lung volume monitoring using electrical impedance tomography was feasible in very preterm infants immediately after birth.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Prophylactic SN cannot be recommended for clinical practice.
Different interfaces, nebuliser types and surfactant concentrations should be researched in bench studies before implementation of SN in future clinical studies.
Introduction
Respiratory distress syndrome (RDS) is usually treated by respiratory support and exogenous surfactant application.1 2 Surfactant is commonly administered into the trachea, either by endotracheal intubation or by transiently inserting a thin catheter (MIST=minimally invasive surfactant therapy).2 Both methods require laryngoscopy which carries the risk of vasovagal reactions and may be associated with intraventricular haemorrhage.3 Thus, a truly non-invasive approach to surfactant application is still sought.4
Surfactant nebulisation (SN) may be a promising alternative.5–7 In a meta-analysis of preterm infants with RDS, SN was associated with a reduced need for intubation within 72 hours after birth when compared with standard care.8 To date, clinical studies on SN were restricted to infants on the neonatal intensive care unit (NICU).6 7 9 10 Even though delivery room (DR) management is essential for the prevention of long-term lung injury,11 12 the effect of early prophylactic SN has never been investigated so far.
Electrical impedance tomography (EIT) allows non-invasive and radiation-free lung volume imaging,13 thus making it a valuable tool for monitoring preterm infants.14 15 Changes in end-expiratory lung impedance (∆EELI) are a good measure for changes in overall lung aeration in preterm infants and correlate with changes in functional residual capacity (FRC).16
The primary objective of this randomised controlled trial was to compare the effect of prophylactic SN immediately after birth on EELI changes with standard care (positive distending pressure alone) in preterm infants between 26 and 32 weeks’ gestation. Secondary outcomes included physiological and clinical outcomes.
Methods
Trial design
This is a masked (blinding of parents and healthcare providers), parallel, prospective, randomised controlled trial conducted at the University Hospital Zurich comparing SN immediately after birth to positive distending pressure alone. The trial was approved by the Cantonal Ethics Committee Zurich (KEK-2020-00890) and registered on clinicaltrials.gov on March 19, 2020 (NCT04315636). This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Participants
All infants born between 26 0/7 and 31 6/7 weeks’ gestation at the University Hospital Zurich were eligible to participate. Exclusion criteria were a severe congenital malformation adversely affecting lung aeration or life expectancy, a priori palliative care and a genetically defined syndrome. In case of multiple births, the infant with the lower predicted birth weight was chosen to be randomised. Antenatal written informed consent was obtained from the parents.
Intervention
All infants received delayed cord clamping for 60 s and, once they reached the resuscitaire, they were supported on continuous positive airway pressure support (CPAP) with a positive distending pressure of 8 mbar using the EVE NEO ventilator (Fritz Stephan GmbH, Gackenbach, Germany) and a facemask (ComfortStar, Dräger Medical System, Lübeck, Germany). The decision to escalate pressure levels, to initiate non-invasive intermittent positive pressure ventilation (NIPPV) or to switch the interface to a nasopharyngeal tube (Vygon, Ecouen, France) or nasal prongs (Heinen & Löwenstein GmbH, Bad Ems, Germany) was at the clinician’s discretion.
In the intervention group, 200 mg/kg surfactant (poractant alfa, Chiesi Farmaceutici SpA, Parma, Italy; based on the prenatal weight estimate) was nebulised via a customised vibrating-membrane nebuliser (eFlow Neonatal Nebulizer System, PARI Pharma, Starnberg, Germany) positioned between the facemask and the ventilator circuit (online supplemental figure 1). Nebulisation commenced simultaneously with the first application of a positive distending pressure after birth and continued until the entire surfactant was nebulised, irrespective of the mode of non-invasive respiratory support. Infants randomised to the control group had the same setup without the nebuliser and they received positive distending pressure alone (ie, CPAP or NIPPV).
Supplemental material
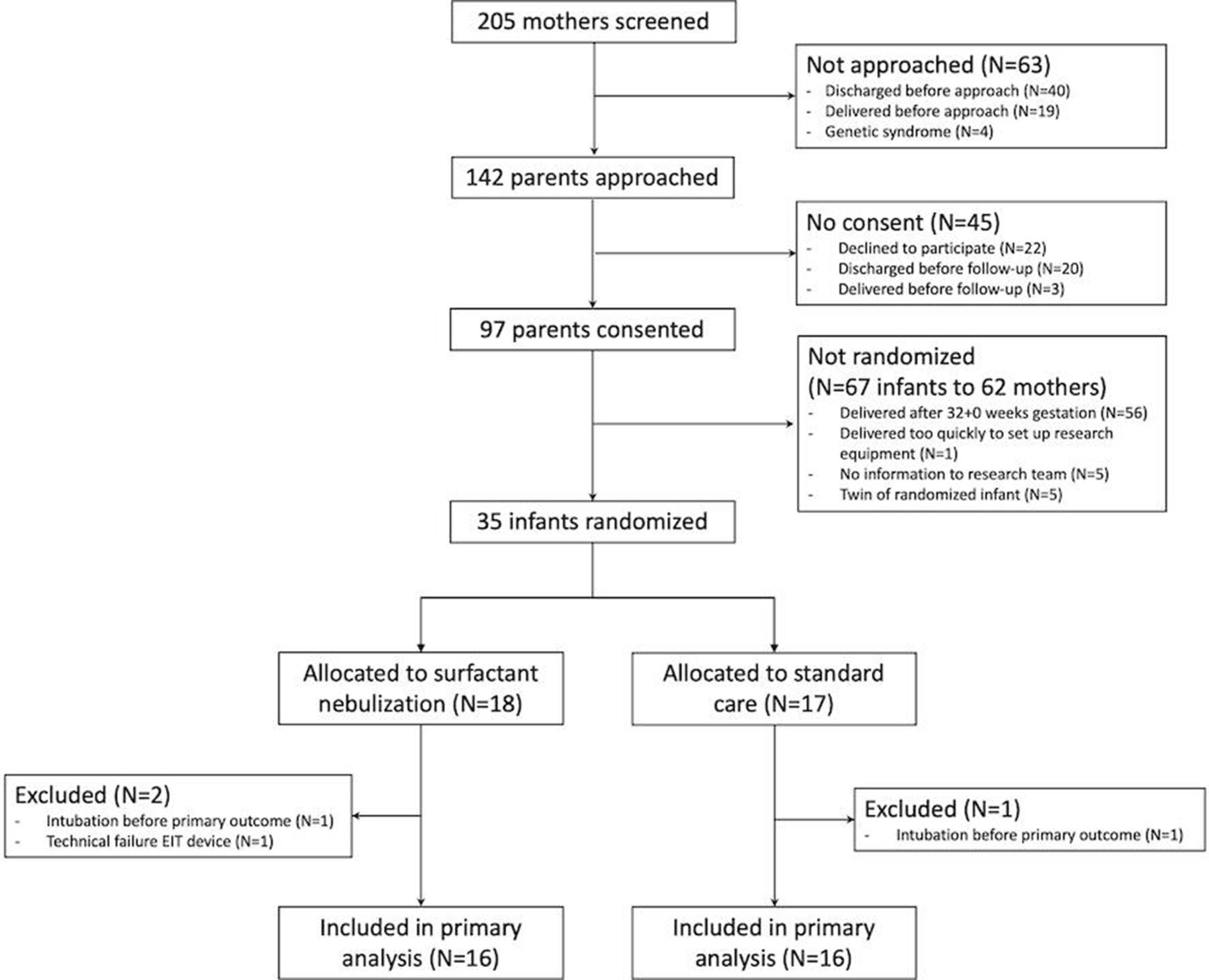
Flowchart of included infants. EIT, electrical impedance tomography.
Data collection
A researcher not otherwise involved in resuscitation was present for each delivery to set up data collection devices before birth: A textile EIT belt was fastened at nipple level as soon as the infant reached the resuscitaire. The LuMon device (SenTec AG, Landquart, Switzerland) was used to record EIT data at a frame rate of 51 Hz.14 EIT data analysis is described in the online supplemental file.
Supplemental material
Stabilisations were video recorded from above, providing a view of the infant’s body and the operator’s hands. Airway flow and pressure were measured continuously using a flow sensor with an accuracy of ±5% placed between the T-piece ventilation device and the facemask until the infant was switched to nasal prongs. Heart rate (HR) and preductal peripheral oxygen saturation (SpO2) were recorded using a Masimo Radical 7 pulse oximeter (Masimo Corporation, Irvine, California, USA). Fraction of inspired oxygen (FiO2) was measured using an oxygen analyzer (AX300, Teledyne Analytical Instruments, California) in the inspiratory limb of the ventilator. Respiratory function parameters were recorded at 200 Hz using the NewLifeBox recording system and breaths were extracted using Pulmochart software (Advanced Life Diagnostics, Weener, Germany).17 18
Outcomes
Primary outcome was the change in end-expiratory lung impedance (ΔEELI) between birth and 30 min (ΔEELI=EELI@30min − EELI@0min). Infants were excluded from primary outcome analysis if they received additional exogenous surfactant before 30 min after birth (via endotracheal tube or MIST) or if EIT data collection failed.
Physiological secondary outcomes were changes in EELI and cardiorespiratory parameters (mean airway pressures (MAPs), expired tidal volume (VT), inspiratory time (Ti), ratio of inspiratory and expiratory time (Ti/Te-ratio), respiratory rate (RR), SpO2, FiO2, SpO2/FiO2ratio and HR) at 10-min intervals for the first 90 min after birth and at 6, 12 and 24 hours after birth. Averages were computed during each selected timeframe for subsequent analyses.
Clinical secondary outcomes were episodes of desaturation and bradycardia, number of events with hypothermia (<36.5°C) or hyperthermia (>37.5°C), respiratory failure (defined as endotracheal application of surfactant, via endotracheal tube or via MIST; failure criteria are described in the online supplemental file) during hospitalisation, age at first intubation, moderate or severe bronchopulmonary dysplasia (defined as oxygen need at 36 weeks postmenstrual age),19 intraventricular haemorrhage (IVH) ≥grade 2,20 any grade retinopathy of prematurity (ROP), surgically treated necrotising enterocolitis (NEC), blood culture-positive sepsis, mortality, any air leak (ie, pneumothorax, pneumomediastinum or pulmonary interstitial emphysema), pulmonary haemorrhage, time on different modes of respiratory support in days (ie, CPAP, NIPPV and mechanical ventilation), length of hospital stay and postmenstrual age at discharge. Mortality, air leak and pulmonary haemorrhage within the first 24 hours after birth were pre-specified safety outcomes. Clinical outcome data were analysed in all enrolled patients including those excluded from primary outcome analysis.
Sample size
In pilot measurements, EELI increased by a mean 11 AU/kg (SD 11 AU/kg) over the first 30 min after birth. To detect an additional increase of 11 AU/kg in the SN group (corresponding to one-third the effectiveness of MIST15) with a power of 80% and an alpha error of 5%, a sample size of 32 infants (16 per group) was required.
Randomisation and masking
The random allocation sequence was generated by a member of the research team who was subsequently not involved in randomisation or patient recruitment (JT). Using the online randomisation option in RedCap,21 another researcher (VDG or CMR) randomised infants immediately before birth in a 1:1 ratio to either standard care (positive distending pressure alone) or additional SN using random block sizes of two and four. Parents and healthcare providers on the NICU were blinded to the intervention but due to the nature of the intervention, the clinical team in the DR was unblinded. The outcome assessor was unblinded.
Statistical analysis
Normally distributed data are presented as mean with SD or 95% CI. Non-parametric data are presented as median and IQR. Differences between SN and standard care were evaluated using a t-test or Wilcoxon test, depending on data distribution. Dichotomous outcomes were compared using Fisher’s exact test. In case of significant differences, comparisons of secondary outcomes were corrected for multiple testing using the Bonferroni-Holm method. Adjusted p values<0.05 were considered statistically significant. Statistical analyses were performed using R statistics (version 3.6.2).22
Results
Population
Data of 35 infants were collected between 19 March 2021 and 14 January 2022. All infants received the allocated treatment and primary outcome data were analysed from 32 infants (figure 1). Baseline characteristics are provided in table 1.
Baseline patient characteristics (N=32)
Primary outcome
Thirty minutes after birth, ∆EELI was not significantly higher in the intervention group (median (IQR) ∆EELI30min: 25 (7–62) AU/kg vs 10 (0–26) AU/kg, p=0.21, figure 2).
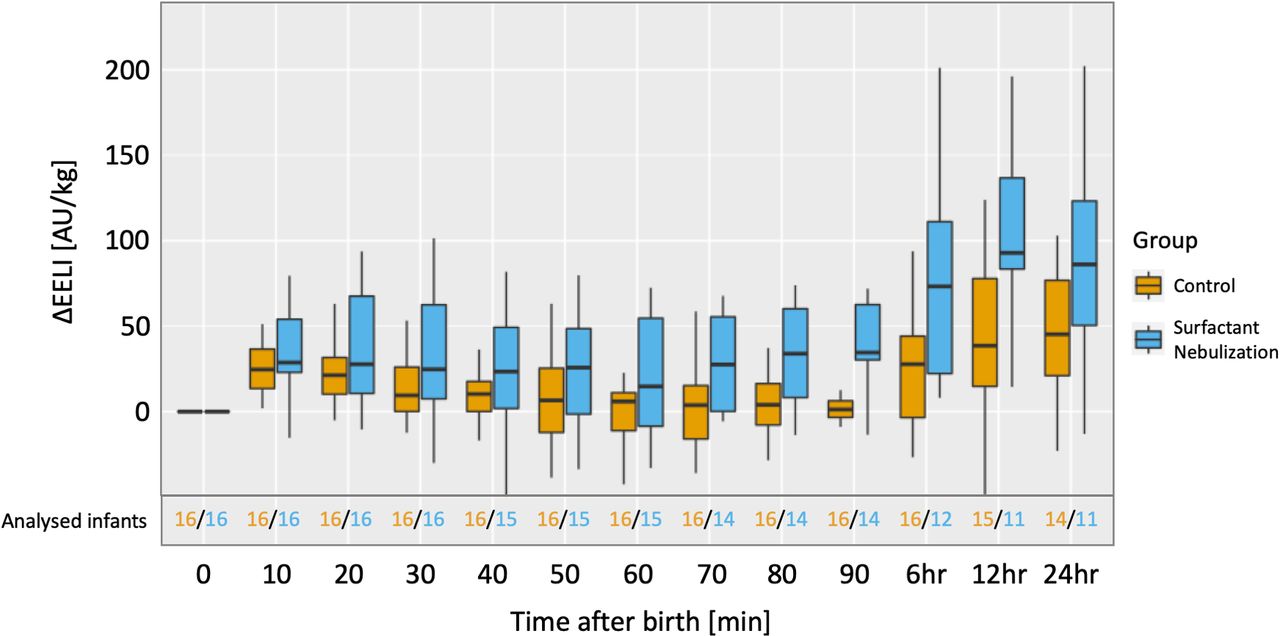
Development of end-expiratory lung impedance (EELI) over the first 24 hours after birth (N=32). The corresponding exact values can be found in online supplemental figure 1. Of note, the decrease in the number of analysed infants is due to infants with respiratory failure (ie, receiving endotracheal surfactant). Inclusion of these infants would systematically skew the data. AU/kg, arbitrary units per kilogram body weight; ∆EELI, changes in end-expiratory lung impedance.
Secondary outcomes
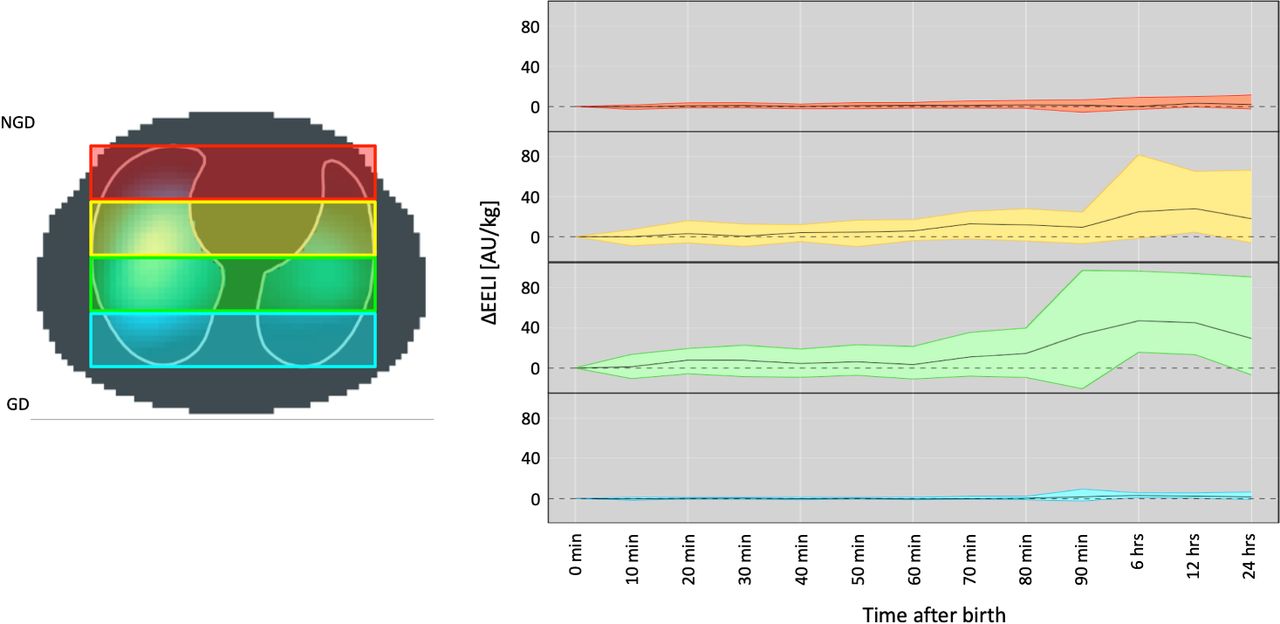
∆EELI was slightly higher in the intervention group at 6 and 12 hours after birth (figure 2), which was mainly attributable to central lung areas (figure 3). After correction for multiple testing, there were no changes in ventilation distribution, MAP, SpO2/FiO2 ratio, HR as well as detailed respiratory function data between the groups (online supplemental figure 2 and online supplemental tables S1-S4).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Changes in end-expiratory lung impedance (EELI) in four horizontal slices over the first 24 hours after birth. Analysis for each timepoint is based only on infants who are non-invasively ventilated at the respective timepoint (see figure 2 for exact numbers). Colours in the graph on the right correspond to colours of the functional EIT image on the left: most non-gravity-dependent in red, central non-gravity-dependent in yellow, central gravity-dependent in green and most gravity-dependent in blue. The corresponding exact values can be found in online supplemental figure 2. As infants were nursed in a supine position throughout the EIT recordings, functional electrical impedance tomography images are shown in a ventral–dorsal orientation. Thus, dorsal lung regions (ie, those closest to the mattress depicted as a grey line) were considered gravity-dependent. AU/kg, arbitrary units per kilogram body weight; ∆EELI, changes in end-expiratory lung impedance;EIT, electrical impedance tomography; GD, gravity-dependent; NGD, non-gravity-dependent.
Besides an increased number of overall doses of surfactant in the intervention group, there were no significant differences in clinical secondary outcomes (table 2).
Intention to treat analysis for clinical outcomes (N=35)
Safety
We noted two serious adverse events in the intervention group: one infant developed a pneumothorax requiring drainage 3 hours after birth. Another infant had an airway obstruction with persistent bradycardia during SN requiring endotracheal suctioning and subsequent intubation.
Discussion
In this randomised controlled trial, we found no significant effect of prophylactic SN in the DR on end-expiratory lung impedance 30 min after birth when compared with standard care. ∆EELI was slightly increased in the intervention group at 6 and 12 hours after birth, which was mainly attributable to an increase in the central lung areas. There were no meaningful differences in further physiological or clinical outcomes.
Electrical impedance tomography is a novel technology which allows non-invasive and radiation-free imaging of the lung.13 Over the recent years, a number of observational studies have provided additional insight into pulmonary pathophysiology,14 23 24 but to our knowledge, no randomised controlled trial with an EIT variable as primary endpoint has been published so far. Changes in end-expiratory lung impedance (∆EELI) are a good correlate of ∆FRC.16 In this study, ∆EELI 30 min after birth was higher after SN compared with standard care but this did not reach statistical significance. The median difference was as large as hypothesised but the confidence intervals were wider than expected which may be due to the highly adaptive situation in the DR with irregular breathing patterns and rapid changes in aeration.25 26 Also, lung deposition of vibrating membrane nebulisers is estimated to be only 5%–20% under ideal situations.27 With longer expiration times during the transitional period in the DR,28 the deposition rate of SN may be further hampered. Still, FRC was increased after SN at certain timepoints, possibly corresponding to a reduced alveolar surface tension and consequently, to a reduced end-expiratory alveolar collapse.29 Unsurprisingly, this effect was strongest in the central lung areas where the majority of air flow is directed. Compared with the immediate effect of instilled surfactant, the effect of nebulised surfactant on FRC was delayed,15 likely due to a deferred formation of an active surfactant layer during the gradual lung fluid absorption in the distal airways after birth. However, there are other factors possibly contributing to this finding: (1) Infants receiving endotracheal surfactant were excluded from EIT data analysis, which may have contributed to increasing differences over time. However, inclusion of ventilated infants would have skewed the data even stronger. (2) There was a non-significantly increased rate of antenatal steroids and preterm premature rupture of membranes in the intervention group and both factors are known to reduce RDS.30 31 Considering these confounding factors, there may well be no clinically meaningful effect of prophylactic SN on lung aeration. A potential improvement for future studies could be the timing of the intervention. It was argued previously that the transitional period consists of three phases where the lung is still liquid-filled in the first phase after birth.26 A fluid-filled lung would preclude surfactant reaching the distal airways at this stage. However, analogous to previous data,32 most infants in our study were breathing spontaneously when reaching the resuscitaire more than a minute after birth, suggesting at least a partial lung aeration at this timepoint, particularly as the first few breaths after birth already contribute largely to generating FRC.33 Still, future studies may need to incorporate an individualised approach by first measuring lung aeration using EIT and starting prophylactic SN only when a certain increase in ∆EELI is noted.
While intratracheal surfactant application improves lung aeration as well as ventilation homogeneity,34 35 we did not see a meaningful effect of prophylactic SN on physiological outcomes. Any effects towards a different ventilation distribution were marginal and vanished after correction for multiple testing. Most importantly, neither ventilation nor aeration homogeneity was improved after SN. The deposition rate during SN, particularly in the DR with longer expiration times, may be too small to achieve even a physiological effect.27 28 A higher surfactant concentration per millilitre increases the surface activity of pulmonary surfactant36 and may possibly yield a measurable and relevant effect despite low deposition rates. However, detailed bench studies evaluating different interfaces, nebulisers and concentrations of surfactant are needed before further clinical studies are warranted.
Cardiorespiratory parameters were largely comparable over time between the two groups. Importantly, leak and frequency of facemask repositionings during DR stabilisation were not increased after SN. During nebulisation, however, infants in the intervention group required slightly higher MAP and increased FiO2 to keep SpO2 within target limits. SN is associated with temporary desaturations,37 38 which may have resulted in an increase of MAP and FiO2 in our setting. We speculate that the increased dead space introduced by the nebuliser and the additional fluid in the inspiratory air may have further contributed to this adverse finding. Also, there were two serious adverse events (airway obstruction and pneumothorax, each occurring in 1 of 18 infants) in the intervention group. These side effects warrant further investigation and caution should be exercised during prophylactic SN.
Previous studies evaluating safety and efficacy of SN were limited to the NICU.6–9 We demonstrated that SN is feasible in the DR, providing a basis for future trials evaluating clinical outcomes of prophylactic SN. A recent meta-analysis comparing SN with standard care in preterm infants with RDS revealed a small reduction in intubation rate after SN, particularly in infants >28 weeks’ gestation.8 In our trial, intubation rate was slightly higher after SN but the current study was not powered to detect clinical differences. Considering that we did not see a physiological impact of prophylactic SN in this small trial, clinical effects seem unlikely. Thus, further bench studies are needed to re-evaluate the ideal combination of device, surfactant concentration and interface used for prophylactic SN before further clinical studies are warranted.
This study has various limitations: First, it was a single-centre study and results may not be generalisable to different units with differing approaches to neonatal stabilisation. Second, we only investigated a small sample of 32 infants which limits clinical validity of the data. Our study was not powered to detect clinically meaningful differences. Third, we only included infants between 26 and 32 weeks’ gestation. While the necessity of preventing respiratory failure is largest among infants <26 weeks,39 we used a limited age range to show feasibility of performing SN in the DR despite the rapidly adapting situation. Fourth, we only investigated a specific combination of nebuliser, dose and concentration of surfactant. Fifth, the neonatal team in the DR and the outcome assessor were unblinded which introduces potential bias. Finally, infants were initially stabilised using a facemask. There is less lung deposition with facemasks compared with interfaces positioned closer to the glottis.7 40 While facemasks are widely accepted as primary interface in the DR, the ideal interface for SN still needs to be evaluated.
Conclusion
In this randomised controlled trial, we found no significant effect of prophylactic SN in the DR on ∆EELI when compared with standard care. Apart from a slightly increased EELI in the intervention group at 6 and 12 hours after birth, mostly due to an improved aeration in central lung areas, we found no further physiological benefits after prophylactic SN. There were no clinically important differences in outcomes between the groups. Collecting EIT data and performing SN during DR stabilisation were feasible. Different interfaces, nebuliser types and most importantly, surfactant concentrations should be researched before implementation in future clinical studies.
Data availability statement
Data are available upon reasonable request. Deidentified individual participant data will be made available from three months to three years following publication, in addition to study protocols, the statistical analysis plan, and the informed consent form to researchers who provide a methodologically sound proposal, with approval by an independent review committee (“learned intermediary”). Data requestors will need to sign a data access or material transfer agreement approved by USZ. Proposals should be submitted to vincent.gaertner@usz.ch to gain access.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Cantonal Ethics Committee of Zurich (approval number KEK-2020-00890). Written informed consent was provided by the parents or guardians of the participants before the study.
Acknowledgments
We thank Prof Jan Vermant and Maria Novaes from the Eidgenössische Technische Hochschule Zürich for scientific input regarding properties of aerosolised surfactant. Finally, we thank all parents and infants who participated in the study and the staff at the neonatal intensive care unit of the Department of Neonatology of the University Hospital Zurich, Switzerland.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators SUNSET study group: David Glauser, Marianne Hauff, Leonie Plastina, Tanja Restin, Janine Thomann and Sandra Ziller (all Newborn Research Zurich, Department of Neonatology, University Hospital Zurich, Switzerland).
Contributors VDG conceptualised and designed the study, recruited patients, collected data, analysed the data, wrote the initial draft of the manuscript and reviewed and revised the manuscript. SM helped to conceptualise and design the study, and critically reviewed the manuscript for important intellectual content. TM recruited patients, collected data and critically reviewed the manuscript for important intellectual content. DB helped to conceptualise and design the study, and critically reviewed the manuscript for important intellectual content. CMR conceptualised and designed the study, recruited patients, collected data, coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content. David Glauser, Marianne Hauff, Leonie Plastina, Tanja Restin, Janine Thomann and Sandra Ziller assisted in data collection and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. VDG acts as the guarantor of the work.
Funding VDG was supported by the European Society for Pediatric Research, the Heuberg-Foundation and the SwissLife Foundation. TM was supported by the Anna-Müller-Grocholski Foundation. JT was supported by a Filling The Gap Grant of the University of Zurich. CMR was supported by the EMDO foundation.
Competing interests The nebulisers were provided free of charge by PARI Pharma and the EIT monitor and belts were provided by SenTec AG.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Highlights from this issue