Article Text

Abstract
Objective To determine whether the use of non-invasive respiratory support, such as continuous positive airway pressure and nasal high flow, to treat term infants in Australian and New Zealand tertiary neonatal intensive care units (NICUs) has changed over time, and if so, whether there are parallel changes in short-term respiratory morbidities.
Design Retrospective database review of patient-level data from the Australian and New Zealand Neonatal Network (ANZNN) from 2010 to 2018. Denominator data on the number of term inborn livebirths in each facility was only available as annual totals.
Patients and setting Term, inborn infants cared for in NICUs within the ANZNN.
Main outcome measures The primary outcome was the annual change in hospital-specific rates of non-invasive respiratory support per 1000 inborn livebirths, expressed as a percentage change. Secondary outcomes were the change in rates of mechanical ventilation, pneumothorax requiring drainage, exogenous surfactant treatment and death before hospital discharge.
Results A total of 14 656 term infants from 21 NICUs were included from 2010 to 2018, of whom 12 719 received non-invasive respiratory support. Non-invasive respiratory support use increased on average by 8.7% per year (95% CI: 7.9% to 9.4% per year); the number of term infants receiving non-invasive respiratory support almost doubled from 980 in 2010 (10.8/1000 livebirths) to 1913 in 2018 (20.8/1000). There was no change over time in rate of mechanical ventilation or death. The rate of pneumothorax requiring drainage increased over time, as did surfactant treatment.
Conclusions Non-invasive respiratory support use to treat term infants cared for in NICUs within the ANZNN is increasing over time. Clinicians should be diligent in selecting infants most likely to benefit from treatment with non-invasive respiratory support in this relatively low-risk population of term newborn infants. Analysis of patient-level data by individual NICUs is recommended to control for potential confounding due to changes in population over time.
- neonatology
- intensive care units, neonatal
- paediatrics
Data availability statement
Data may be obtained from a third party and are not publicly available.
Statistics from Altmetric.com
What is already known on this topic?
Modes of non-invasive respiratory support, such as continuous positive airway pressure and nasal high flow, are commonly used to treat newborn infants with respiratory distress.
Early non-invasive respiratory support benefits very preterm infants in whom the risk of respiratory distress syndrome and its associated mortality and morbidity is elevated.
Anecdotally, non-invasive respiratory support is increasingly used to treat newborn infants born at term who are more likely to have a less severe respiratory illness.
What this study adds?
In Australian and New Zealand neonatal intensive care units, non-invasive respiratory support use to treat term newborn infants has increased on average by almost 9% per year.
Rates of pneumothorax requiring drainage and surfactant treatment also increased over time.
How this study might affect research, practice or policy?
Unnecessary non-invasive respiratory support use should be avoided; a period of observation of newborn infants with mild respiratory distress prior to commencing non-invasive respiratory support may be prudent.
The rate of surfactant use has increased over time, which requires further exploration, especially given the uncertainty around surfactant treatment for term infants with respiratory distress.
We observed differences between individual hospitals in many outcomes, especially in the non-invasive respiratory support rate; local auditing of practice may be important.
Background
Modes of non-invasive respiratory support, such as continuous positive airway pressure (CPAP) and nasal high flow, are commonly used to treat newborn infants with respiratory distress.1–4 Most evidence for non-invasive respiratory support use comes from trials performed in tertiary neonatal intensive care units (NICUs). However, studies have also demonstrated the benefits of non-invasive respiratory support in non-tertiary special care nurseries.5 6
Early non-invasive respiratory support use has been shown to benefit very preterm infants in whom the risk of respiratory distress syndrome and its associated mortality and morbidity is elevated.7 Anecdotally, however, non-invasive respiratory support is increasingly being used to treat newborn infants born at term. These infants are more likely to have a self-limiting, short-term respiratory illness such as transient tachypnoea of the newborn, or mild respiratory distress syndrome, with low morbidity and mortality.8 Previously, term infants receiving non-invasive respiratory support may have been observed without intervention, or treated with supplemental oxygen alone.9
A lower threshold for treating term infants with non-invasive respiratory support might lead to earlier treatment with possible clinical benefits, such as a faster recovery, and reduced need for mechanical ventilation (MV) or exogenous surfactant therapy. In non-tertiary centres, these benefits may translate into reduced rates of transfer to a tertiary NICU. However, it is also possible that increased use of non-invasive respiratory support in low-risk infants might be detrimental by causing or prolonging separation of the infant from family or increasing the use of adjunctive medical treatments.
The Australian and New Zealand Neonatal Network (ANZNN, www.ANZNN.net) is a collaborative clinical network that monitors the care of high-risk newborn infants. The network includes all tertiary NICUs across Australia and New Zealand. All infants who are admitted to a participating unit during the first 28 days of life and meet one or more of the following criteria are included in the ANZNN registry: born <32 weeks’ gestation; birth weight <1500 g; received MV or non-invasive respiratory support for ≥4 consecutive hours, or died while receiving MV prior to 4 hours of age; received major surgery or received therapeutic hypothermia.
Aims
To determine whether the use of non-invasive respiratory support to treat term infants in Australian and New Zealand NICUs has changed over time, and if so, whether there are parallel changes in short-term respiratory morbidities.
Methods
Data sources
The number of inborn term livebirths in each year from 2010 to 2018 was requested from each NICU participating in the ANZNN registry. Separately, the ANZNN registry provided a dataset for all term inborn infants born ≥37 weeks’ gestation who met ANZNN criteria during the same period. Each NICU has an audit officer who collects and checks the data before submission into a central ANZNN database; accuracy of the data collection is validated by data crosschecking by ANZNN data managers. Individual patient data are available for each ANZNN-registered infant; variables were defined according to the ANZNN data dictionary (anznn.net/dataresources/datadictionaries).
Data from NICUs without a maternity unit (eg, children’s hospitals), with no inborn registrants in 1 or more years, or with no inborn liveborn data available for 1 or more years were excluded.
Population of interest
Term inborn infants cared for in tertiary NICUs registered with ANZNN.
Outcomes
Five outcomes available from the ANZNN database for 2010–2018 were prespecified. The primary outcome was the annual change in hospital-specific rates of non-invasive respiratory support per 1000 inborn livebirths, expressed as a percentage change. The modes of non-invasive respiratory support recorded in the ANZNN database were CPAP and nasal high flow. Data on specific settings, devices or interfaces (eg, CPAP mask or prongs) were not available. Infants who had any exposure to either CPAP or nasal high flow (for any length of time) were included as having received non-invasive respiratory support; this comprises infants with 4 or more hours of non-invasive respiratory support if this is the only qualification for ANZNN registration, and infants with any duration of non-invasive respiratory support if they qualified for ANZNN registration for another reason (eg, mechanical ventilation, major surgery). Secondary outcomes were the change in rates of MV (4 or more hours, or <4 hours and died, of intermittent mandatory ventilation, intermittent positive pressure ventilation, high-frequency oscillatory ventilation or CPAP by endotracheal tube), pneumothorax requiring drainage, exogenous surfactant treatment and death before hospital discharge.
Statistical analysis
Data on the number of inborn livebirths and different subgroups of registrants are described. Linear regression was used to assess statistical significance of within-hospital change in number (eg, annual number of term births) and logistic regression to assess within-hospital change in rates (eg, change in non-invasive respiratory support rates over time). All analyses were performed with the use of SAS software, V.9.4 (SAS Institute, Cary, North Carolina, USA). Average change in the annual number of births was estimated using a linear mixed effects model (‘PROC MIXED’ in SAS), to control for repeated measures by hospital, time as a fixed effect and baseline as a random effect.10 Specifying hospital baseline as a random effect allows the model to treat each hospital as if it has its own baseline rate in 2010, rather than assuming that all hospitals have a common underlying baseline rate. For all annual rates, overall change over time was estimated as a fixed effect (‘PROC GLIMMIX’ in SAS, with a binomial distribution and logit link function) with repeated measures by hospital, and hospital baseline specified as a random effect. As the event rates are rare (all <5%), the estimated event rates are presented as rates/1000 term inborn livebirths and the estimated ORs are interpreted as risk ratios,11 and change in rates is presented as an annual percentage change, to simplify exposition. No formal adjustment was made for multiple statistical comparisons.
Results
The annual number of term inborn livebirths in the 21 hospitals ranged from 1618 to 7369, with a total of 754 054 over 9 years. The number was estimated to be increasing significantly over time in seven hospitals, unchanged in seven and decreasing significantly in seven. Overall, the estimated average change in term inborn livebirths was +9.4 births/year (p=0.12; 95% CI: −3.1 to 21.9).
There were 30 NICUs with a total of 28 110 ANZNN term registrants in the period 2010–2018. We excluded 13 454 infants who were either not clearly inborn or had been born in an ineligible NICU (figure 1), leaving 14 656 eligible registrants from 21 NICUs.

Selection of study population. NICU, neonatal intensive care unit. ANZNN, Australian and New Zealand Neonatal Network.
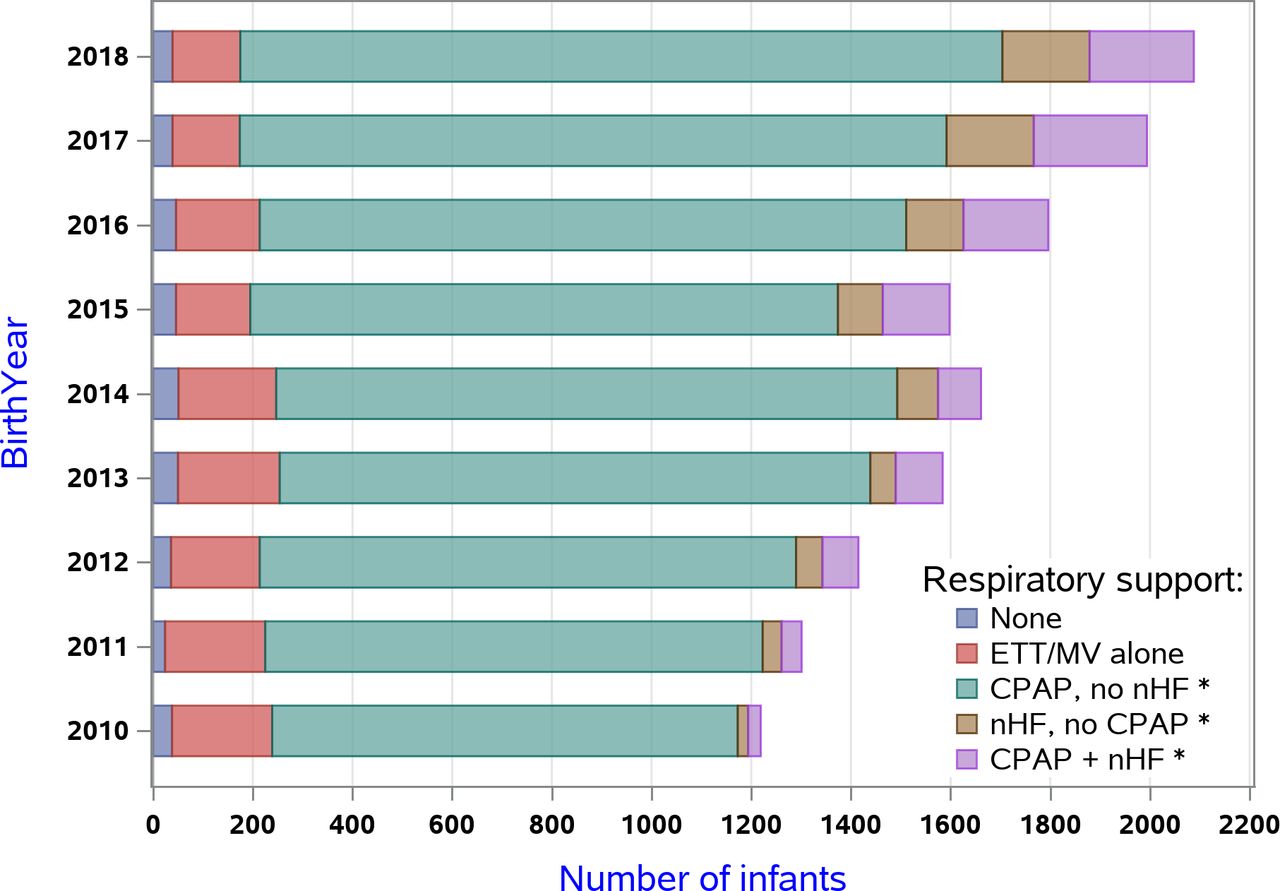
During 2010–2018, 14 656 (1.9%) of the term inborn livebirths were registered with ANZNN. Of these ANZNN registrants, 2.3% were from a multiple birth, 48% were born by caesarean section, the mean (SD) gestational age was 38.9 (1.4) weeks and birth weight was 3406 (578) g, 62.0% were males and 15.1% had a congenital anomaly (table 1). A total of 12 719 infants received non-invasive respiratory support across the period 2010–2018; this included a small number of infants (332, 2.6%) who received <4 hours of non-invasive respiratory support (ie, infants who were eligible for registration with ANZNN for a reason other than non-invasive respiratory support) or in whom the duration of non-invasive respiratory support was not recorded. The number of infants receiving non-invasive respiratory support almost doubled from 980 in 2010 to 1913 in 2018 (figure 2).

Type of respiratory support each year from 2010 to 2018. CPAP, continuous positive airway pressure; ETT, endotracheal tube; MV, mechanical ventilation; nHF, nasal high flow. *Includes some infants that also receive ETT/MV.
Characteristics of 14 656 eligible registrants
Primary outcome: rate receiving non-invasive respiratory support
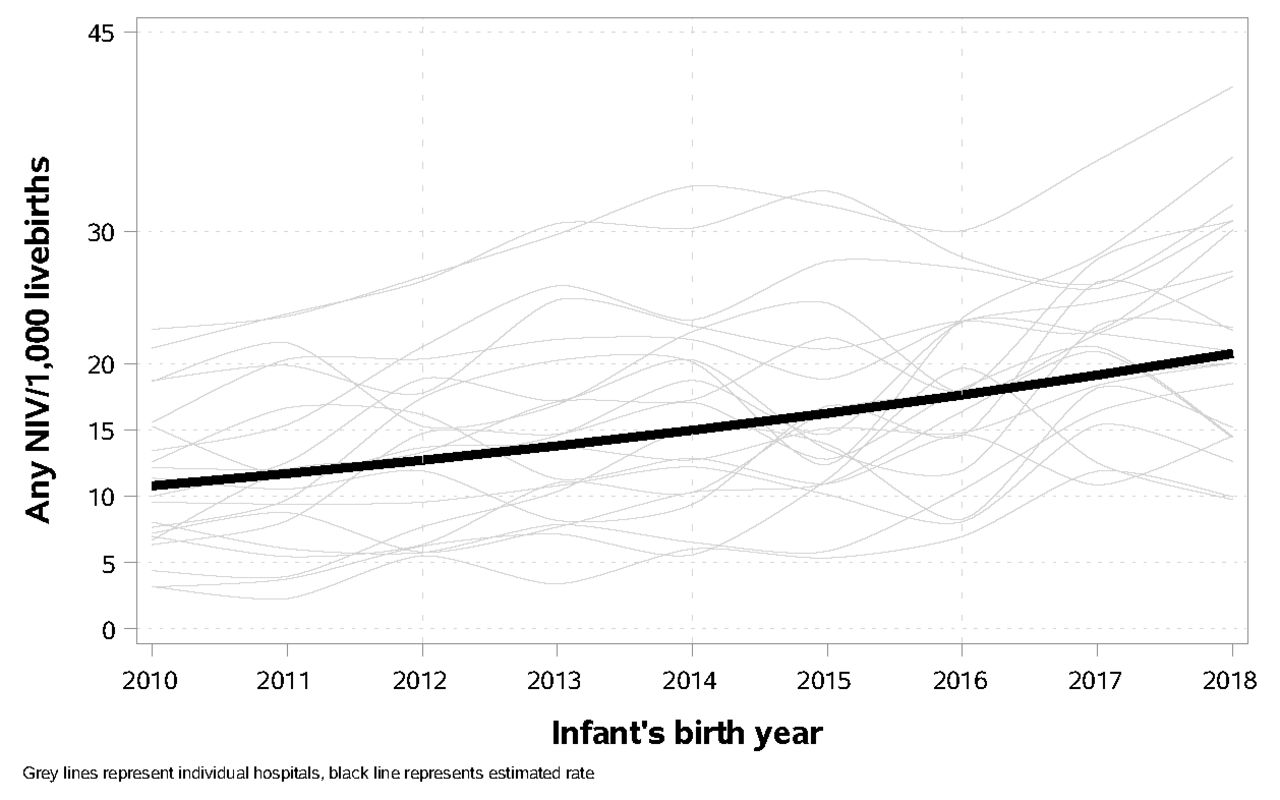
Across the 21 NICUs, hospital-specific rates of non-invasive respiratory support increased by 8.7% per year (p<0.0001; 95% CI: 7.9% to 9.4% per year), from an estimated 10.8/1000 livebirths in 2010 to 20.8/1000 livebirths in 2018 (figure 3).
{kind=link}
{kind=link}
{kind=link}
Non-invasive respiratory support rate and average in 21 neonatal intensive care units; 2010–2018.
Nineteen of the 21 NICUs had a statistically significant increase in non-invasive respiratory support rates over time; no NICU had a statistically significant decrease in non-invasive respiratory support rates over time. The annual rate of non-invasive respiratory support at individual NICUs ranged from 3.1 to 22.6/1000 livebirths in 2010 and from 9.7 to 40.9/1000 livebirths in 2018 (figure 3).
Secondary outcomes
Table 2 shows the results of change over time for the secondary outcomes. There was no change over time in the MV rate (p=0.66) or in death (p=0.39). Of the 397 deaths, 198 (49.9%) were secondary to a congenital anomaly. There was some evidence of increasing pneumothorax requiring drainage (4.0% per year; 95% CI: 0.3% to 7.7% per year; p=0.03; increasing from an estimated 0.49/1000 livebirths in 2010 to 0.66/1000 livebirths in 2018) and increasing surfactant use (7.8% per year; 95% CI: 4.8% to 10.9% per year; p<0.0001; increasing from an estimated 0.66/1000 in 2010 to 1.21/1000 in 2018).
Secondary outcomes
Discussion
For inborn term infants cared for in Australian and New Zealand NICUs, non-invasive respiratory support use is increasing. The number of infants receiving non-invasive respiratory support in 21 NICUs increased from 980 in 2010 to 1913 in 2018, an increase of >100 treated infants each year. Most received CPAP.
The drivers for clinicians to increasingly treat term newborn infants with non-invasive respiratory support are unclear and plausibly multifactorial. While we could not find any published studies exploring this question, we hypothesise that the drivers may broadly include: (1) the increased availability of devices that can provide positive end expiratory pressure (PEEP) in both the delivery room and neonatal unit. Once PEEP is being provided in the delivery room, this may lead to a desire to continue its provision into the neonatal unit. The abundance of devices, relative ease of use and perhaps a lack of written indications for use in this population may also play a role; (2) unjustified generalisation of data across populations: it is possible that the known benefits of non-invasive respiratory support for very preterm infants, resulting in increased use, are being inappropriately applied to the term infant population. There may be a fear that not commencing non-invasive respiratory support early for an infant with undifferentiated respiratory distress could result in more severe disease; (3) individual unit practices and the distribution of medical and nursing resources: infants with respiratory distress require close observation whether they are treated with non-invasive respiratory support or not. Some postnatal wards may not have the capacity to undertake frequent observations and this may lead to admission to the neonatal unit (potentially de-skilling of maternity unit staff and entrenching this practice), where there is an assumption that infants are sick, and thus a lower threshold for use of non-invasive respiratory support. There is also pressure on units to discharge infants as soon as possible, so non-invasive respiratory support may be initiated in the belief that this will lead to quicker resolution of symptoms and faster discharge without causing harm; (4) medical staff experience and tolerance of signs of respiratory distress: although we do not have data to support this, it is possible that there is an acute increase in non-invasive respiratory support every time there is a change in junior medical staff. It is also possible that there are fewer senior medical staff who have had experience caring for infants with respiratory distress in an era when non-invasive respiratory support was not available.
In secondary analyses of a randomised trial of non-invasive respiratory support modes conducted by our group in Australian non-tertiary special care nurseries,6 we found that non-invasive respiratory support treatment success (in this case nasal high flow) was predicted by lower supplemental oxygen requirements prior to randomisation,12 and that the subgroup of infants born ≥36 weeks’ gestation who were not receiving supplemental oxygen at the time of randomisation (to either nasal high flow or CPAP) had less severe illness than those receiving supplemental oxygen, with low rates of treatment failure, MV and need for transfer to a tertiary NICU.13 Potential risks and downstream effects of non-invasive respiratory support use include admission to a neonatal unit, separation of the infant from family and the frequent use of concomitant intravenous fluids and antibiotics13; thus, unnecessary non-invasive respiratory support use should be avoided. A period of observation of newborn infants with respiratory distress prior to a decision to commencing non-invasive respiratory support may be prudent, especially in those who do not have a supplemental oxygen requirement.
If clinicians are commencing non-invasive respiratory support earlier and more frequently with the intention to avoid surfactant and/or MV, our results indicate that this has not been achieved. The rate of MV did not change, and there was strong evidence that the rate of surfactant use increased over time, which requires further exploration, especially in light of the uncertainty around surfactant treatment for term infants with respiratory distress.14 Of concern, the rate of pneumothorax requiring drainage appears to have also increased over time; the fact that these pneumothoraces were drained indicates they were considered clinically significant. The overall rate of pneumothorax requiring drainage was 3.2% among eligible registrants across the 9 years of study (table 2). Given the plausible association between early non-invasive respiratory support use and pneumothorax in newborn infants,5 6 this is an important safety issue that must be considered by clinicians when deciding whether to commence non-invasive respiratory support in this population.
Although not a prespecified aim of our study, we observed differences between individual hospitals in many outcomes, especially in the non-invasive respiratory support rate. In 2018, there was a more than fourfold range in non-invasive respiratory support rates per 1000 inborn livebirths in the 21 NICUs that were examined, from 9.7/1000 to 40.9/1000. The presence of substantial variation in practice raises questions as to whether these can be attributable to differences in patient profile, clinical or operational circumstances or reflects unjustified interhospital variation in health system performance.15 Individual hospitals can explore their detailed datasets to explore patient-level factors that were not available to the current study, as they have access to individual data on each inborn infant, not just those registered with ANZNN. Alternatively, groups of hospitals can cooperatively audit performance.
There are several limitations of our study. The estimated change in non-invasive respiratory support use over time does not include an unknown number of newborn infants who receive <4 hours of continuous non-invasive respiratory support; ANZNN registrants must receive at least 4 hours of non-invasive respiratory support or meet another ANZNN registration criterion. Our lack of individual patient data for infants not registered with NICUs means we were unable to determine if the increase in the proportion of infants being treated with non-invasive respiratory support reflected changes in the underlying population at risk over time. For example, there may have been differences in maternal characteristics such as the incidence of gestational diabetes, or there may have been a higher proportion of inborn term infants that were ‘sicker’ (smaller, more immature, lower Apgar scores) due to improved antenatal referral to tertiary centres, or other changes in practice such as the mode of delivery. We were also unable to assess other potential benefits or harms of non-invasive respiratory support use, as the data were not part of the ANZNN database. For example, we could not examine the effects of increasing non-invasive respiratory support use on the use of intravenous fluids, antibiotics or effects on breastfeeding rates.
In conclusion, the use of non-invasive respiratory support to treat term infants in NICUs in Australian and New Zealand has increased over time, without any reduction in MV, and a concomitant increase in pneumothorax requiring drainage and surfactant use. Clinicians should be diligent in selecting newborn infants most likely to benefit from treatment with non-invasive respiratory support in this relatively low-risk population. Interunit variation warrants further exploration.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study did not require ethical approval as data from the ANZNN is approved for use for research purposes.
Acknowledgments
Thanks to all Advisory Council Members of the ANZNN: Advisory Council Members of ANZNN (*denotes ANZNN Executive). Australia: Scott Morris (Flinders Medical Centre, South Australia), Peter Schmidt (Gold Coast University Hospital, Queensland), Larissa Korostenski (John Hunter Children’s Hospital, New South Wales), Mary Sharp, Steven Resnick, Rebecca Thomas, Andy Gill*, Jane Pillow* (King Edward Memorial and Perth Children’s Hospitals, Western Australia), Jacqueline Stack (Liverpool Hospital, New South Wales), Pita Birch, Karen Nothdurft* (Mater Mother’s Hospital, Queensland), Dan Casalaz, Jim Holberton* (Mercy Hospital for Women, Victoria), Alice Stewart, Rod Hunt* (Monash Medical Centre, Victoria), Lucy Cooke* (Neonatal Retrieval Emergency Service Southern Queensland, Queensland), Lyn Downe (Nepean Hospital, New South Wales), Michael Stewart (Paediatric Infant Perinatal Emergency Retrieval, Victoria), Andrew Berry (NSW Newborn & Paediatric Emergency Transport Service), Leah Hickey (Royal Children’s Hospital, Victoria), Peter Morris (Royal Darwin Hospital, Northern Territory), Tony De Paoli, Naomi Spotswood* (Royal Hobart Hospital, Tasmania), Srinivas Bolisetty, Kei Lui* (Royal Hospital for Women, New South Wales), Mary Paradisis (Royal North Shore Hospital, New South Wales), Mark Greenhalgh (Royal Prince Alfred Hospital, New South Wales), Pieter Koorts (Royal Brisbane and Women’s Hospital, Queensland), Carl Kuschel, Lex Doyle (Royal Women’s Hospital, Victoria), John Craven (SAAS MedSTAR Kids, South Australia), Clare Collins (Sunshine Hospital, Victoria), Andrew Numa (Sydney Children’s Hospital, New South Wales), Hazel Carlisle (The Canberra Hospital, Australian Capital Territory), Nadia Badawi, Himanshu Popat (The Children’s Hospital at Westmead, New South Wales), Guan Koh (The Townsville Hospital, Queensland), Jonathan Davis (Western Australia Neonatal Transport Service), Melissa Luig* (Westmead Hospital, New South Wales), Bevan Headley, Chad Andersen* (Women’s & Children’s Hospital, South Australia). New Zealand: Nicola Austin (Christchurch Women’s Hospital), Brian Darlow (Christchurch School of Medicine), Liza Edmonds (Dunedin Hospital), Guy Bloomfield (Middlemore Hospital), Mariam Buksh, Malcolm Battin* (Auckland City Hospital), Jutta van den Boom (Waikato Hospital), Callum Gately (Wellington Women’s Hospital). We also wish to acknowledge ANZNN Executive that are not members of hospitals' contributing data: Georgina Chambers* (National Perinatal Epidemiology and Statistics Unit, University of New South Wales); Victor Samuel Rajadurai* (KK Women’s and Children’s Hospital, Singapore); David Barker* (Whangarei Hospital, New Zealand), Anjali Dhawan* (Blacktown Hospital, New South Wales), Barbara Hammond* (Whanganui Hospital, New Zealand), Natalie Merida* (consumer), Linda Ng* (ACNN).
References
Footnotes
Twitter @calumtheroberts
Contributors BJM, AB and GA led the project, all authors conceived and planned the manuscript and analysis. GA performed all of the data analysis. BJM wrote the first draft of the manuscript. AB, GA and PGD revised the manuscript. BJM is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests BJM, LSO, CTR and PGD and their research activities are supported by Medical Research Future Fund (MRFF, Australia) or National Health and Medical Research Council (NHMRC, Australia) fellowships and grants.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue