Article Text

Abstract
Background The feasibility and benefits of continuous sustained inflations (SIs) during chest compressions (CCs) during delayed cord clamping (physiological-based cord clamping; PBCC) are not known. We aimed to determine whether continuous SIs during CCs would reduce the time to return of spontaneous circulation (ROSC) and improve post-asphyxial blood pressures and flows in asystolic newborn lambs.
Methods Fetal sheep were surgically instrumented immediately prior to delivery at ~139 days’ gestation and asphyxia induced until lambs reached asystole. Lambs were randomised to either immediate cord clamping (ICC) or PBCC. Lambs then received a single SI (SIsing; 30 s at 30 cmH2O) followed by intermittent positive pressure ventilation, or continuous SIs (SIcont: 30 s duration with 1 s break). We thus examined 4 groups: ICC +SIsing, ICC +SIcont, PBCC +SIsing, and PBCC +SIcont. Chest compressions and epinephrine administration followed international guidelines. PBCC lambs underwent cord clamping 10 min after ROSC. Physiological and oxygenation variables were measured throughout.
Results The time taken to achieve ROSC was not different between groups (mean (SD) 4.3±2.9 min). Mean and diastolic blood pressure was higher during chest compressions in PBCC lambs compared with ICC lambs, but no effect of SIs was observed. SIcont significantly reduced pulmonary blood flow, diastolic blood pressure and oxygenation after ROSC compared with SIsing.
Conclusion We found no significant benefit of SIcont over SIsing during CPR on the time to ROSC or on post-ROSC haemodynamics, but did demonstrate the feasibility of continuous SIs during advanced CPR on an intact umbilical cord. Longer-term studies are recommended before this technique is used routinely in clinical practice.
- resuscitation
- physiology
- neonatology
Data availability statement
Data are available on reasonable request. All data are available upon request to Prof Graeme Polglase.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Return of spontaneous circulation is feasible during chest compressions on an intact umbilical cord.
Time to return of spontaneous circulation is similar during chest compressions on an intact umbilical cord versus after umbilical cord clamping.
Umbilical cord clamping after return of spontaneous circulation reduces rebound hypertension.
What this study adds?
Chest compressions on an intact umbilical cord resulted in higher mean and diastolic blood pressure compared with chest compressions after umbilical cord clamping.
The time to achieve return of spontaneous circulation was not altered by single or continuous sustained inflations.
Continuous sustained inflations may result in prolonged impairment of pulmonary blood flow and worse oxygenation.
Introduction
Birth asphyxia, defined by WHO as “the failure to initiate and sustain breathing at birth”, is responsible for a quarter of all neonatal deaths with the majority occurring on the first day of life. Although rare (~0.2% of all births in Australia),1 infants exposed to severe asphyxia require cardiopulmonary resuscitation (CPR) in the delivery room, which involves application of chest compressions and administration of epinephrine (adrenaline).
Current neonatal resuscitation guidelines recommend chest compressions (CCs) if the heart rate remains <60/min despite adequate ventilation for at least 30 s.2–4 CCs are provided using a rate of 90/min in sequences of 3 CC followed by a pause to deliver one inflation at a rate of 30/min, which corresponds to a 3:1 compression:ventilation (C:V) ratio.2 3 However, the most effective C:V ratio in newborn infants remains controversial. We have recently described an alternative CC technique, combining continuous sustained inflations during CC (CC +SIcont) which significantly improved time to return of spontaneous circulation (ROSC) and survival compared with 3:1 C:V in a post-transitional piglet model.5 However, a study in lambs showed similar time to ROSC with CC +SIcont and 3:1 C:V.6 A randomised feasibility trial in preterm infants <32 weeks’ gestation reported significantly shorter (fourfold) time to ROSC with CC +SIcont than with 3:1 C:V.7 Currently, the SURV1VE trial is comparing these two strategies in newborn infants born >28+0 weeks’ gestational age requiring CC in the delivery room.8 9
Current neonatal resuscitation guidelines recommend immediate cord clamping (ICC) for infants requiring CC.2–4 We have recently demonstrated that ventilation and CC while attached to the umbilical cord in newborn lambs, termed physiological-based cord clamping (PBCC), does not impede the ability or increase the time taken to achieve ROSC.10 However, it is unclear whether ICC or PBCC influences the outcomes following different respiratory support techniques during CCs.
Our aim was to determine whether PBCC combined with SIcont during CCs provides physiological benefit over ICC and a single SI (SIsing) followed by standard 3:1 C:V. We hypothesised that continuous SIs during CCs in both ICC and PBCC groups would reduce the time to ROSC in asystolic near-term lambs, and provide a physiological benefit after ROSC compared with standard resuscitation.
Materials and methods
The experimental procedures were approved by Monash Medical Centre Animal Ethics Committee A, Monash University, and were conducted in accordance with the National Health and Medical Research Council of Australia’s guidelines and the ARRIVE guidelines.11
Instrumentation and delivery
Pregnant Border-Leicester ewes (Ovis aries) at 139±2 days’ gestation (term ~148 days) were anaesthetised by intravenous injection of thiopentone sodium (20 mg/kg; Jurox, NSW, Australia), followed by tracheal intubation and delivery of inhaled anaesthesia (isofluorane 1.5%–2.5% in oxygenated air; Bomac Animal Health, NSW, Australia). Fetal surgery and instrumentation have been described in detail previously.10 12 Briefly, ultrasonic flow transducers (Transonic Systems, Ithaca, NY, USA) were placed around the left main pulmonary artery and left carotid artery, and catheters were inserted into a carotid artery and jugular vein.10 12 13 Arterial pressures and blood flows were digitally recorded in real time (1 kHz, Powerlab; ADInstruments, NSW, Australia).10 The fetal trachea was intubated with a 4.5 mm cuffed endotracheal tube and lung liquid was drained passively. A transcutaneous arterial oxygen saturation (SpO2) probe (Masimo, Radical 4, CA, USA) was placed around the right forelimb of the lamb and a Near Infrared Spectroscopy optode (Casmed Foresight; CAS Medical Systems Inc, Branford, CT, USA) was placed over the left frontal cortex and used to continuously measure cerebral tissue oxygen saturation (SctO2).10 On completion of surgery, the fetus was removed from the uterus, dried and placed on the ewes’ abdomen on a hot water bottle to maintain core body temperature.
Once physiological parameters were stable, asphyxia was induced by clamping the umbilical cord (ICC groups) or occlusion of the maternal common internal iliac artery (PBCC groups) as described previously.10 The common internal iliac artery remained occluded throughout the experiment (including during CPR). Hypoxia was allowed to progress until lambs became asystolic, defined as mean arterial blood pressure of ~0 mmHg and absence of carotid and pulmonary arterial blood flow traces. Respiratory support was then provided using a T-piece device (Neopuff; Fisher and Paykel Healthcare, Auckland, New Zealand) using one of two strategies:
A single 30 s SI (SIsing) to 30 cmH2O using 100% oxygen, followed by positive pressure ventilation with a peak inflation pressure of 30 cmH2O, end-expiratory pressure of 5 cmH2O targeting 60 breaths per minute; or
Continuous 30 s SIs (SIcont), with a 1 s break between SIs, from initiation of respiratory support until ROSC.
Overall, this resulted in four groups being studied: ICC+SIsing (n=12), ICC+SIcont (n=7), PBCC+SIsing (n=9) and PBCC+SIcont (n=7).
One minute after ventilation onset, CCs were initiated using an asynchronous technique at a 3:1 ratio in the SISING groups, with continuous CCs used in the SICONT groups. However, all groups received 90 compressions per minute. Epinephrine (10 µg/kg estimated body weight) was given intravenously 1 min after CCs were initiated, and every 3 min thereafter for a maximum of four doses. On ROSC, defined as end-diastolic blood pressure >20 mm Hg and spontaneous unassisted heart contractions,14 lambs were transferred to volume guaranteed ventilation targeting 7 mL/kg with warm humidified air (Dräeger Babylog 8000+ ventilator; Dräeger, Lübeck, Germany). The fraction of inspired oxygen was adjusted to maintain arterial oxygen saturation between 90% and 95% and ventilation parameters adjusted to maintain PaCO2 between 45 and 55 mm Hg. Lambs in the PBCC groups underwent umbilical cord clamping 10 min after ROSC.
Lambs were sedated throughout the study (ethical requirement) which prevented spontaneous breathing (Alfaxan intravenous 5–15 mg/kg/h in 5% dextrose; Jurox, NSW, Australia). Carotid arterial blood samples were collected regularly to measure blood gas parameters using a blood gas analyser (ABL90; Radiometer, Brønshøj, Denmark) in order to monitor the lamb’s well-being and guide respiratory support.
Calculations
Cerebral oxygen delivery (DO2, mL/kg/min)=(CBF·CaO2)/brain weight (kg).
Arterial oxygen content (CaO2)=([1.39·Hb·SaO2/100]+[0.003·PaO2]), where Hb is the haemoglobin concentration (g/dL). Alveolar-arterial difference in oxygen was calculated as (713*FiO2)−(PaCO2/0.8)−PaO2.
Statistical analysis
All baseline fetal and physiological data were compared using a two-way ANOVA (GraphPad Prism V.9.0.0; GraphPad Software, CA, USA). Two-way repeated measures ANOVA with Holm-Sidak post hoc comparison was used to compare serial physiological data. Statistical significance was accepted at p<0.05.
Results
Fetal characteristics
Fetal characteristics are outlined in table 1. Body weight of ICC lambs was significantly lower than PBCC lambs (p=0.007), but no other differences were observed. pH was not different between groups. PaO2 was significantly higher in ICC +SIcont compared with ICC lambs (p=0.02) while PaCO2 was significantly lower in ICC +SIcont lambs compared with PBCC lambs (p<0.05). Fetal lactate levels were similar in all groups.
Fetal characteristics
At the end of the asphyxia period when asystole was reached and immediately prior to initiation of resuscitation, blood-gas variables were not different between groups (overall mean±SD: pH: 6.892±0.04; PaCO2: 112.4±18.3 mm Hg; PaO2: 7.4±4.7 mm Hg; lactate 11.8±2.5 mmol/L).
Return of spontaneous circulation
Two lambs in the ICC group, and one lamb in each of the PBCC and ICC +SIcont groups failed to reach ROSC and were excluded from the analysis. There were no differences in the time taken to achieve ROSC between groups (figure 1). There was no difference in the number of doses of epinephrine required to achieve ROSC between the groups (mean (SD) ICC +SISING: 1.7±0.9; PBCC +SISING: 1.7±1.0; ICC +SIcont: 1.9±1.1; PBCC +SIcont: 1.7±1.0 doses).

Time to return of spontaneous circulation in ICC+SIsing (blue), PBCC+SIsing (red), ICC+SIcont (green) and PBCC+SIcont (purple) lambs. Individual animals are shown with mean (95% CI) included. Black dots indicate lambs which failed to achieve ROSC. This image was created by GRP.
Physiological parameters
Physiology during chest compressions
During the first minute of CC (prior to epinephrine), mean and diastolic blood pressures were significantly higher in PBCC +SIsing and PBCC +SIcont lambs compared with ICC +SIsing and ICC +SIcont lambs (figure 2). Following epinephrine, mean and diastolic blood pressures during CC remained higher in PBCC +SIsing and PBCC +SIcont groups compared with ICC +SIcont, but not ICC +SIsing lambs. No differences in other physiological variables were observed between groups during CC. Furthermore, within ICC and PBCC groups, SIs did not alter any physiological variables during CC.

Mean (A–B), systolic (C–D) and diastolic (E–F) carotid arterial blood pressures (CAP) averaged over the first minute of chest compressions (CCs) (prior to epinephrine) or averaged during the remaining duration of CCs (after epinephrine) in ICC+SIsing (blue), PBCC+SIsing (red), ICC+SIcont (green) and PBCC+SIcont (purple) lambs. Individual animals are shown with mean (95% CI) included. Letters that are different indicates statistical difference (p<0.05). This image was created by GRP.
Physiology after ROSC
Blood-gas measurements and oxygenation
Blood-gas and oxygenation data throughout the study are shown in figure 3. After ROSC, pH was significantly higher in ICC +SIsing and PBCC+SIsing lambs compared with ICC +SIcont and PBCC+SIcont lambs. PaCO2 was significantly higher in ICC +SIcont lambs compared with ICC +SIsing from 9 min, but no other differences in PaCO2 were observed. PaO2 was significantly lower in ICC +SIcont lambs compared with ICC +SIsing from 12 min. Lactate was significantly lower in ICC +SI lambs compared with all other groups. SaO2 was not different between groups at any time. SctO2 was significantly higher in ICC lambs compared with PBCC lambs with no effect of SIs observed. Cerebral oxygen delivery was not different between groups (p=0.11). Alveolar arterial difference in oxygen was significantly lower (better) in PBCC+SIsing lambs compared with ICC +SIsing and PBCC+SIcont lambs for the first 6 min after ROSC. However, from 20 min after ROSC, ICC +SIsing lambs had lower AaDO2 compared with ICC +SIcont and PBCC+SIcont lambs.
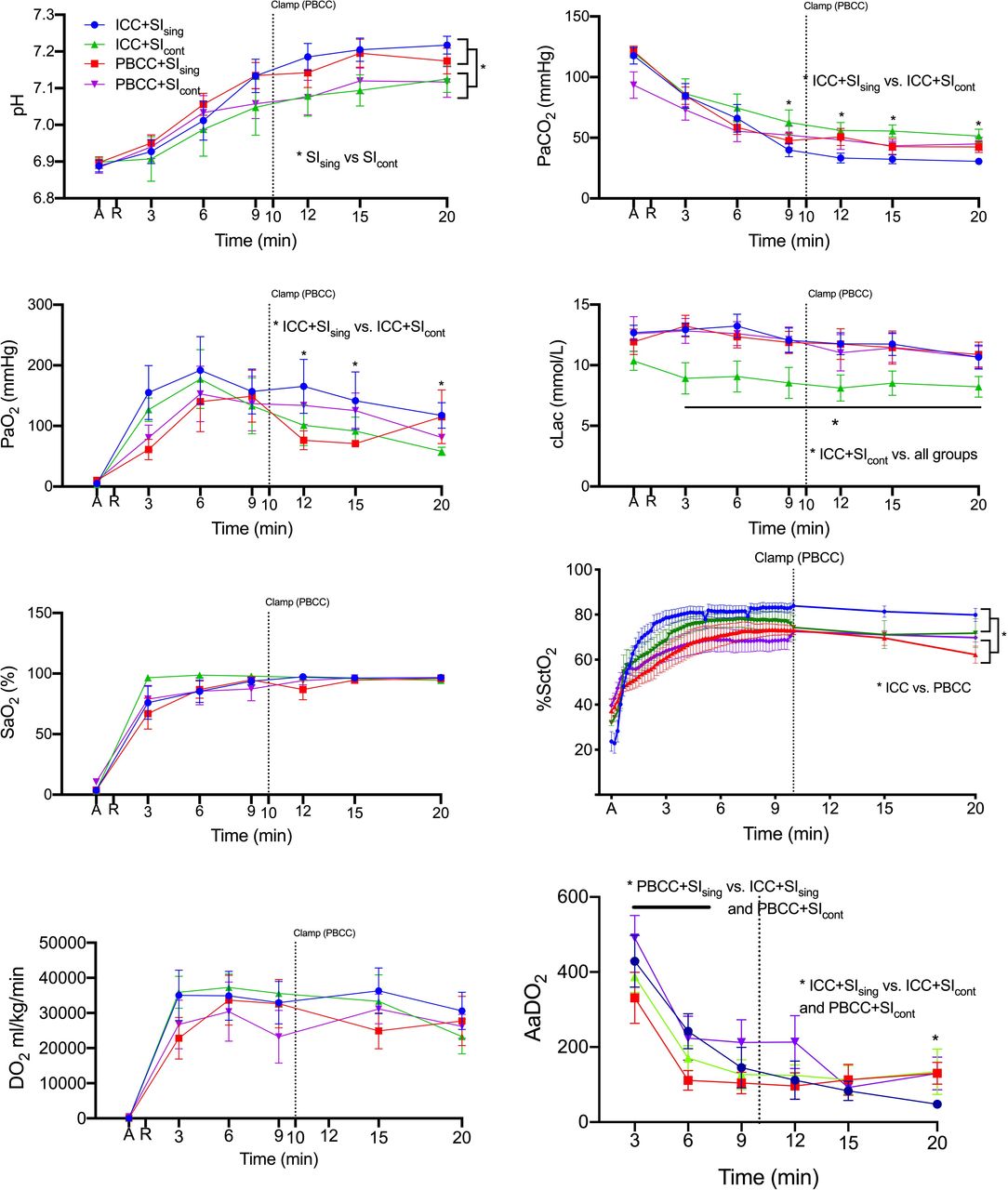
(A) pH, (B) partial arterial pressures (Pa) of carbon dioxide (CO2), (C) Pa of oxygen (O2), (D) lactate, (E) arterial saturations SaO2, (F) cerebral oxygenation (SctO2), (G) cerebral oxygen delivery (DO2) and (H) alveolar-arterial difference in oxygen (AaDO2) measured at the end of the asphyxia period (A) and on return of spontaneous circulation (R) in ICC+SIsing (blue), PBCC+SIsing (red), ICC+SIcont (green) and PBCC+SIcont (purple) lambs. Data are mean±SEM. * indicates significant difference with comparisons detailed on the graphs. This image was created by GRP.
Heart rate and blood pressure
Heart rates in ICC+SIcont lambs were significantly higher than ICC+SIsing lambs within the first 30 s after ROSC, while ICC+SIsing lambs had lower HR between 240 and 330 s after ROSC compared with all other groups (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Mean heart rates, (B) mean carotid arterial blood pressures (CAP), (C) mean pulmonary blood flows (PBF) and (D) mean carotid arterial blood flows (CaBF) measured at control, fetal (F), at the end of the asphyxia period (A) and on return of spontaneous circulation (ROSC) in ICC+SIsing (blue), PBCC+SIsing (red), ICC+SIcont (green) and PBCC+SIcont (purple) lambs. Data are mean±SEM. * indicates significant difference p<0.05. This image was created by GRP.
Mean blood pressure is detailed in figure 4 while systolic and diastolic blood pressures are included in online supplemental figure 1. Mean and systolic blood pressures were significantly higher in ICC groups compared with the PBCC groups (figure 4 and online supplemental file 1). SIs did not alter the response. Diastolic blood pressure was significantly higher in ICC lambs 2–3 min after ROSC compared with PBCC groups. Overall, SIcont caused a significantly lower diastolic blood pressure than SIsing (online supplemental figure 1) irrespective of cord clamping time.
Supplemental material
Supplemental material
Pulmonary blood flow
Mean and end-diastolic PBF +SIsing in ICC+SIsing lambs were significantly higher during the first 5 min after ROSC compared with all SIcont groups, while mean and end-diastolic PBF were significantly higher in ICC+SIcont lambs between 110 and 210 s after ROSC compared with PBCC+SIsing and PBCC+SIcont lambs (figure 4C and online supplemental figure 1). However, beyond 10 min, SIcont lambs had significantly lower mean, end-diastolic and peak-systolic PBF compared with SIsing lambs.
Carotid blood flow
Mean and end-diastolic carotid blood flows were significantly higher in ICC groups compared with PBCC groups during the first 5 min and 10 min, respectively, after ROSC, with no effect of SIs observed (figure 4D and online supplemental figure 1). Peak-systolic carotid blood flows were significantly higher in PBF groups compared with ICC groups at 15 and 20 min. No effect of sustained inflations was observed.
Discussion
Current neonatal resuscitation guidelines recommend ICC and a 3:1 C:V in newborn infants requiring CC.2–4 It is not known whether this is the optimal way to provide CPR to asystolic newborns. We compared the use of single versus continuous SIs during both ICC and PBCC in asphyxiated near-term lambs. We found that (1) CC during PBCC and ICC resulted in similar time to ROSC and survival; (2) CC during PBCC generated higher mean and diastolic blood pressures than in ICC; (3) after ROSC, lambs who had ICC displayed rapid overshoot in blood carotid blood flow, and PBF for ~5 min; (4) PBCC reduced the rapid overshoot in blood pressure; and (5) continuous SIs had little effect on the cardiopulmonary transition, but reduced PBF and diastolic arterial pressure 10 min after ROSC.
We aimed to determine whether SIcont resulted in a more rapid time to ROSC compared with a SIsing. Contrary to our hypothesis, we found no difference in the time taken to achieve ROSC between SIcont and SIsing groups with either ICC or PBCC. A study using post-transitional asphyxiated piglets5 15 and a pilot study in preterm infants7 reported faster times to ROSC with SIcont compared with 3:1 C:V. Conversely, Vali et al used a transitional cardiac arrest lamb model and reported similar median (IQR) times to ROSC with 390 (225–405) and 345 (204–465) s.6 The reasons for the differences in outcomes are not clear and may represent species differences given the similar outcomes in transitional lamb studies.
An interesting finding from our study was that mean and diastolic blood pressure was higher during CCs in lambs undergoing PBCC compared with ICC. We have previously considered that CCs with an intact placental circulation may not be feasible due to an inability to increase diastolic blood pressure >~20 mmHg as a result of the low resistance placental vascular bed. However, our study confirms the findings of our previous study10 and demonstrates that this is not the case, and in fact that the opposite may be true. The potential reason for the higher blood pressure during CCs is unclear, but it is possible that the umbilical arteries passively collapse (thereby increasing afterload) in response to the absence of an internal distending pressure whereas the umbilical veins continue to provide venous return. Further, it is also likely that the ability to increase filling (preload) due to the presence of the umbilical circulation has a greater effect in maintaining blood pressure during resuscitation. Despite the higher mean and diastolic blood pressures during CCs, the time to ROSC was not faster in PBCC groups compared with ICC groups.
A further aim of this study was to determine whether SIcont improved the haemodynamic transition after ROSC in both ICC and PBCC groups compared with CV. However, we found continuous SIs resulted in a similar physiological response immediately after ROSC compared with conventional ventilation. We have previously demonstrated that a single SI during the initial ventilation of severely asphyxiated lambs, with reduced but ongoing cardiac output, reduced the time taken to restore heart rate and blood pressure16 and cerebral blood flow,17 compared with CV. While we did find that SIcont lambs had a higher heart rate within the first 30 s after ROSC, we did not observe any other effect on blood pressure or cerebral blood flow. This indicates that the benefit of a SI is restricted to the period of lung aeration and, as we would expect the lung to fully have aerated prior to ROSC (ie, during the CCs) in both the CV and SI groups, it is not surprising that we saw no difference between the two groups.
We did find that lambs that received SIcont irrespective of ICC of PBCC had lower diastolic blood pressure after 10 min, which was also observed by Vali et al.6 It is not known why SIcont would reduce diastolic blood pressure ROSC, but it may be due to reduced or impaired venous return. It is not known whether the consequences are beneficial or adverse, and this warrants further study. We also showed that SIcont resulted in lower mean, diastolic and systolic PBF in both ICC and PBCC lambs. Right-to-left shunting across the ductus arteriosus, as evidenced by a negative end-diastolic PBF, is a key feature during PBCC because the placenta continues to act as a low resistance pathway for blood and competes with the lung for right ventricular output. However, a high proportion of PBCC +SIcont lambs had negative end-diastolic PBF at the end of the study period (ie, at 20 min), which is indicative of a higher pulmonary vascular resistance. Further, pH, PaO2 and PaCO2 were worse in SIcont lambs post-ROSC, which may be a consequence of the reduced pulmonary perfusion. This observation has not previously been made in other studies using large animals as they were conducted largely in non-transitional models without a patent ductus arteriosus, highlighting the importance of conducting these studies immediately at birth.
We previously reported that PBCC reduced the post-asphyxial overshoot in blood pressure and cerebral blood flow, resulting in reduced protein extravasation—an early indicator of cerebrovascular haemorrhage.10 12 In the current study, we again observed that PBCC reduced the overshoot in carotid blood pressure and blood flow compared with ICC. While we did not examine cerebrovascular injury in this study, our previous findings10 12 suggest that PBCC may be neuroprotective in asphyxiated newborns. Conversely, we have previously shown that a single SI can increase cerebrovascular haemorrhage in mildly asphyxiated lambs.18 More research is required to ensure that interventions delivered at the time of birth do not cause downstream consequences, particularly for the newborn brain.
Limitations
Our asphyxia model uses lambs which were sedated/anaesthetised and intubated with a tightly sealed endotracheal tube. This prevents endotracheal tube leak and optimises lung aeration during respiratory support, but this may not occur in the delivery room as face masks or uncuffed endotracheal tubes are routinely used. We used two different methods of inducing asphyxia to reduce the overall number of ewes required, which allowed us to use twin pregnancies.10 This did mean that PBCC and ICC lambs received different methods of asphyxia. However, the same criteria for determining asystole were used for all lambs, and the blood-gas values at asphyxia were similar in all four groups. We used two different types of CCs in this study: 3:1 compression asynchronous ventilation ratio for the SISING groups and continuous CC for the SICONT groups. Previous studies have found that continuous CC provides better minute ventilation and a faster recovery of CBF than the standard 3:1 C:V approach.19–21 We did not observe any differences between groups that would indicate that the different CC approaches had an influence on our findings, but the study was not designed to explicitly detect potential differences due to CC technique.
Conclusion
In this study, we found no significant benefit of continuous sustained inflations during CPR on the time to ROSC or post-ROSC haemodynamics. We did, however, demonstrate the feasibility of continuous SIs during advanced CPR on an intact umbilical cord. Further longer-term studies are recommended in appropriate transitional models before this technique is used routinely in clinical practice.
Data availability statement
Data are available on reasonable request. All data are available upon request to Prof Graeme Polglase.
Ethics statements
Patient consent for publication
Ethics approval
Monash Medical Centre Animal Ethics Committee A, Monash University (MMCA2018_10).
Acknowledgments
The authors would like to thank Karyn Rodgers, Valerie Zahra and Alison Moxham for their technical support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SBH and GRP are joint senior authors.
Twitter @calumtheroberts
Contributors Study design: GMS, CTR, MK, AWG, SBH, GRP. Study conduct: GMS, CTR, DAB, SB, SLM, KJC, VS, RG, MK, AWG, SBH, GRP. Data analysis and review: GMS, CTR, DAB, SB, SLM, KJC, VS, RG, MK, AWG, SBH, GRP. Manuscript preparation: GMS, CTR, DAB, SB, SLM, KJC, VS, RG, MK, AWG, SBH. GRP is responsible for the overall content as guarantor.
Funding This research was supported by National Institute of Health R01HD072848-01A1, the Research Foundation of the Cerebral Palsy Alliance, a joint National Heart Foundation of Australia and National Health and Medical Research Council (NH&MRC) Research Fellowship (GRP: 1105526), NH&MRC Research Fellowships (SBH: 545921, SM: 1136216, CTR: 1175634, RG: 1090890) and the Victorian Government's Operational Infrastructure Support Program. GMS is a recipient of the Heart and Stroke Foundation/University of Alberta Professorship of Neonatal Resuscitation, a National New Investigator of the Heart and Stroke Foundation Canada and an Alberta New Investigator of the Heart and Stroke Foundation Alberta.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.