Article Text

Abstract
Background Fetal ventriculomegaly is the the most common intracranial abnormality detected antenatally. When ventriculomegaly is mild and the only, isolated, abnormality detected (isolated mild ventriculomegaly (IMVM)) the prognosis is generally considered to be good. We aim to determine if there are features on in utero MRI (iuMRI) that can identify fetuses with IMVM who have lower risks of abnormal neurodevelopment outcome.
Methods We studied cases recruited into the MRI to enhance the diagnosis of fetal developmental brain abnormalities in utero (MERIDIAN) study, specifically those with: confirmed IMVM, 3D volume imaging of the fetal brain and neurodevelopmental outcomes at 3 years. We explored the influence of sex of the fetus, laterality of the ventriculomegaly and intracranial compartmental volumes in relation to neurodevelopmental outcome.
Findings Forty-two fetuses met the criteria (33 male and 9 female). There was no obvious correlation between fetal sex and the risk of poor neurodevelopmental outcome. Unilateral IMVM was present in 23 fetuses and bilateral IMVM in 19 fetuses. All fetuses with unilateral IMVM had normal neurodevelopmental outcomes, while only 12/19 with bilateral IMVM had normal neurodevelopmental outcomes. There was no obvious correlation between measure of intracranial volumes and risk of abnormal developmental outcomes.
Interpretation The most important finding is the very high chance of a good neurodevelopmental outcome observed in fetuses with unilateral IMVM, which is a potentially important finding for antenatal counselling. There does not appear to be a link between the volume of the ventricular system or brain volume and the risk of poor neurodevelopmental outcome.
- neurology
- neonatology
Data availability statement
Data are available upon reasonable request. Requests for patient-level data and statistical code should be made to the corresponding author and will be considered by members of the original trial management group, including the chief investigator and members of CTRU, who will release data on a case-by-case basis. Data will be shared following the principles for sharing patient-level data as described by Smith et al (2015) . The data will not contain any direct identifiers; we will minimise indirect identifiers and remove free-text data, to minimise the risk of identification.
Statistics from Altmetric.com
What is already known on this topic?
Isolated mild ventriculomegaly is thought to have a low risk of poor outcome, with fetal maternal experts quoting <10% or <5% risk.
However the diagnosis of isolated mild ventriculomegaly causes considerable concern for parents who would like to have more certainty about the risk to their fetus.
Ventriculomegaly is the most common intracranial abnormality detected in fetuses.
What this study adds?
Our results suggest that unilateral isolated mild ventriculomegaly is associated with a very low risk of poor neurodevelopmental outcomes, which is important for antenatal counselling.
Neither the sex of the fetus nor the brain and ventricular volumes appear to have a major effect on the risk of poor neurodevelopmental outcomes.
Introduction
Fetal ventriculomegaly is defined by a transverse measurement of a trigone of the lateral ventricles of ≥10 mm at any stage of pregnancy and is the most common intracranial abnormality detected prenatally (2.5/1000 pregnancies).1 The most important feature of a fetus with ventriculomegaly is to determine if other abnormalities or aetiologies are present, so blood tests are frequently offered to look for transplacental infections and amniocentesis to look for chromosomal/genetic abnormalities. Antenatal ultrasonography (USS) is used to look for structural abnormalities of the body or in other parts of the brain, while the results of a recent study have indicated that in utero MRI (iuMRI) should be offered routinely in cases of fetal ventriculomegaly.2–4
If ventriculomegaly is the only abnormality present it is termed ‘isolated’ and the degree of enlargement of the ventricles is used to stratify the risk of abnormal neurodevelopmental outcome used for prenatal counselling. The most frequently used grading system in the UK defines mild (10–12 mm), moderate (13–15 mm) and severe ventriculomegaly (≥16 mm). Isolated mild ventriculomegaly (IMVM) is thought to have a relatively low risk of poor neurodevelopmental outcome, with most fetal maternal experts quoting risk of either a <10% or <5%.5 The diagnosis of fetal IMVM often causes considerable concern for parents who would like to have more certainty about the risk to their individual fetus, over and above the established population-based data.
We aim to show if there are any features on iuMRI of the fetal brain (and other intracranial compartments) that can be used to identify fetuses with IMVM who have a lower risk of abnormal neurodevelopment outcome. Specifically, we will study the influence of sex of the fetus, laterality of the ventriculomegaly (unilateral or bilateral) and intracranial compartmental volumes measured on volumetric iuMRI.
Methods
All of the cases reported in this paper were recruited into either the original MERIDIAN Study (fetuses with abnormal brains),2 or the MERIDIAN add-on study (normal fetuses).6 Each woman provided fully informed written consent.
Fetuses with IMVM
Women recruited into the main MERIDIAN Study carried a fetus with a suspected brain abnormality on antenatal USS and underwent iuMRI imaging in order to determine if diagnostic accuracy was improved. Subsequently neurodevelopmental assessments were obtained in some of the children as detailed in an earlier publication.7 Families were invited to either an assessment using the Bayley Scales of Infant and Toddler Development - Third Edition (BSID3) or, if they declined, to complete an Ages and Stages Questionnaire third Edition (ASQ3) screening tool and/or consent to review their child’s medical notes. Participants were categorised as ‘normal’, ‘at risk’ or ‘abnormal’ in the original study7 but the present analysis uses a binary outcome: normal (combining the ‘normal and ‘at risk’ groups) or abnormal. For clarity, the definition of abnormal in this study did not change: ‘One or more BSID3 composite score below 70 OR; if BSID not done, where ASQ3 scores were below the cut-off level in two or more developmental domains OR; ASQ3 scores were below the cut-off level in one domain and near the cut-off level in two or more domains; OR; the child had cerebral palsy with a Gross Motor Function Classification System (GMFCS) score of 2 or greater’.
The GMFCS is a five-level clinical classification system that describes the gross motor function of people with cerebral palsy on the basis of self-initiated movement abilities.
Inclusion criteria were:
Consented into the main MERIDIAN Study and successful iuMRI in Sheffield including 3D volume imaging.
Survival to 3 years and successful postnatal neurodevelopmental assessment.
Postnatal confirmation of IMVM.
A flow diagram of the cases included is shown in figure 1.
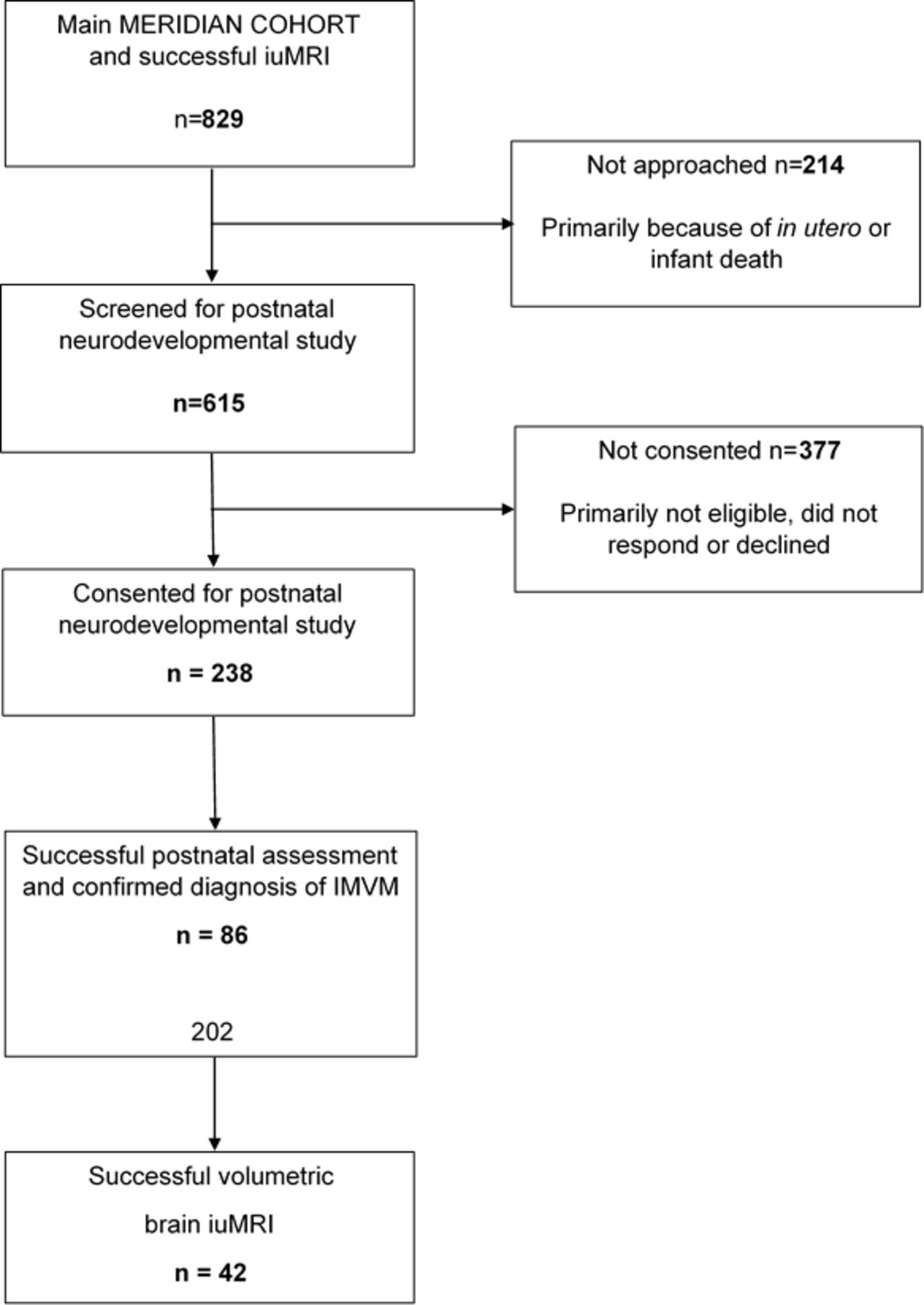
Flow diagram of participants through the study. The authors produced this figure and have permission to use it. IMVM, isolated mild ventriculomegaly; iuMRI, In utero MRI.
Normal fetuses
Two hundred women with normal fetuses had iuMRI in the MERIDIAN add-on study. Normality was assumed on the basis of a low-risk pregnancy, no abnormalities (brain or somatic) on antenatal USS and normal brain imaging on iuMRI. Fetuses were scanned between 18 gestational weeks and 37 gestational weeks and the results of the volumetric analyses described below have been previously published.8 Two out of 200 fetuses in the add-on study had unexpected brain abnormalities on iuMR6 and were replaced with two new cases of matched gestational ages for the present study.
iuMRI technique
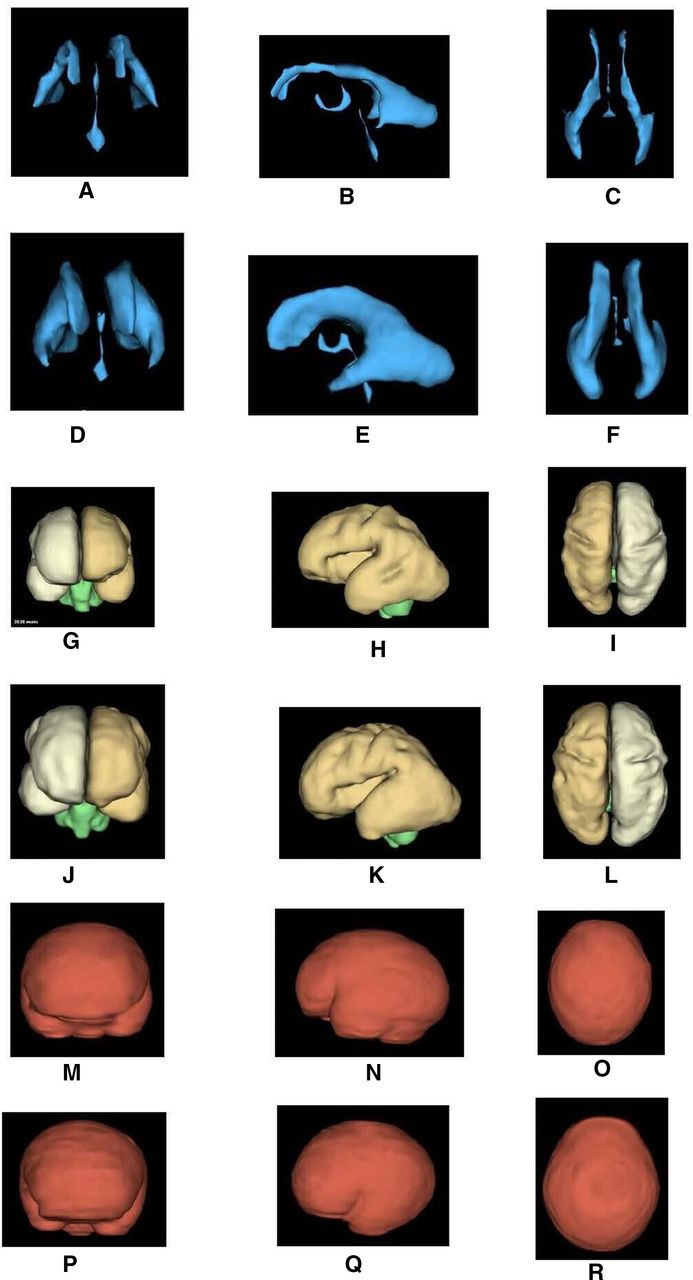
The full iuMRI protocol has been reported elsewhere.2–4 All iuMRI studies were performed on the same 1.5 T whole body scanner (Signa HDx, GE Healthcare, Milwaukee, Wisconsin, USA). iuMRI consisted of T2-weighted single shot fast spin echo sequences of the brain in the three orthogonal planes, T1-weighted and diffusion-weighted imaging in the axial plane and volumetric imaging using a balanced steady-state imaging sequence (3D-FIESTA, GE Healthcare, Milwaukee, Wisconsin, USA) acquired in the axial plane.9 10 The examinations were reported by an experienced paediatric neuroradiologist (PDG). The volumetric data sets were processed by a senior research MR radiographer (DJ) using ‘3D Slicer’ software (http://www.slicer.org). The surfaces of the intracranial compartments (cerebral ventricles, brain and the internal table of the skull) were outlined manually in order to isolate the following compartments: cerebral ventricles, brain parenchyma and the extra-axial cerebrospinal fluid (CSF) spaces. Those volumes were created as electronic models by 3D Slicer (figure 2) and absolute volume measurements were obtained by multiplying the number of voxels in each electronic model by the voxel size in order to calculate: ventricular volume (VV), brain parenchymal volume (BPV) and extra-axial CSF volume (EAV) directly. VV, BPV and EAV were summed to derive the total intracranial volume (TICV). We have previously described good intraobserver and interobserver reproducibility.11 12

{kind=link}
{kind=link}
Images of the intracranial surfaces used for analysis in the study. Figures A–C show the anterior (A), lateral (B) and superior (C) projections of the cerebral ventricles of a normal 26-gestational-week fetus and figures D–F show the equivalent images from a 26-gestational-week fetus with ventriculomegaly. Figures G–I show the anterior (G), lateral (2 hours) and superior (I) projections of the brain of a normal 26-gestational-week fetus and figures J–I show the equivalent images from a 26-gestational-week fetus with ventriculomegaly. Figures M–O show the anterior (M), lateral (N) and superior (O) projections of the surface of the extra-axial spaces of a normal 26-gestational-week fetus and figures P–R show the equivalent images from a 26-gestational-week fetus with ventriculomegaly. The method of deriving ventricular volume, brain volume and extra-axial space volume from these data sets is described in the text. The authors produced these figures and have permission to use them.
Analysis
The chance of a normal neurodevelopmental outcome was calculated for the whole cohort and then for subgroups based on sex of the fetus and laterality of the ventriculomegaly (unilateral compared with bilateral) presented as percentages. The absolute volumes of the four intracranial compartments (VV, BPV, EAV and TICV) for each fetus with IMVM were converted to Z-scores by comparing them with the means and SD of normal fetuses. The mean Z-score for each compartment was calculated along with the 95% confidence limits of the mean. The analysis was repeated for the groups of fetuses with normal and abnormal neurodevelopmental outcomes and their mean values were compared using a two-tailed t-test.
Results
Forty-two fetuses met the entrance criteria and their neurodevelopmental outcome data are summarised in table 1. The cohort included 33/42 (78.6%) male and 9/42 (21.4%) female fetuses (approximately 3.5:1 ratio). Overall, 35/42 (83%) fetuses had normal neurodevelopmental assessments and there was no substantial difference in the chance of a normal outcome between male (28/33–85%) and female (7/9–78%) fetuses. Unilateral IMVM was present in 23/42 (55%) fetuses and bilateral IMVM in 19/42 (45%). In fetuses with unilateral IMVM the left lateral ventricle was involved slightly more frequently than the right—14/23 (60.9%) and 9/23 (39.1%), respectively. Of the fetuses with unilateral IMVM 23/23 (100%) had normal neurodevelopmental assessments, while only 12/19 (63%) fetuses with bilateral IMVM had normal neurodevelopmental assessments. Unilateral IMVM was present in 18/33 (54.5%) male fetuses and 5/9 (55.56%) female fetuses.
The number and proportions of neurodevelopment outcome status at 3–4 years in 42 fetuses in relation to the sex of the child and the symmetry of ventriculomegaly (unilateral or bilateral trigone measurements 10–12 mm) diagnosed in utero
As expected, the fetuses with IMVM had significantly larger VV when compared with an aged-matched fetus from the normal cohort and the difference reached statistical significance at the 5% level (mean Z- score +4.01% and 95% CIs +3.32 to+4.70). In contrast, the EAV in fetuses with IMVM showed no statistical difference from normal fetuses. Both BPV and TICV were larger in fetuses with IMVM when compared with normal fetuses; the changes were relatively modest but reached statistical significance at the 5% level (CIs +0.15 to +0.81 and+0.09 to +0.89, respectively). There were no statistically significant differences between the VV, BPV, EAV or TICV of fetuses with normal and abnormal neurodevelopmental outcomes (table 2).
The relationship between the volume of the intracranial compartments and neurodevelopmental outcome status at 3–4 years in 42 fetuses with confirmed isolated mild ventriculomegaly diagnosed in utero.
Discussion
The original diagnosis of possible ventriculomegaly in cases used in this study was made on ultrasound using the guidance of the International Society of Ultrasound in Obstetrics & Gynecology, which advises measuring the trigones of the lateral ventricles using the following approach: Symmetrical axial view/optimal zoom, atrium (trigone) measured at the level of the glomus of choroid plexus, opposite the parieto-occipital sulcus, callipers placed touching the inner edge of the ventricle wall at its widest part, aligned perpendicular to the long axis of the ventricle. The antenatal confirmed diagnosis of mild ventriculomegaly relied on iuMRI measurements of the trigones, which attempted to follow the USS guidance as described and illustrated previously.13 Some degree of disagreement between the two methods should be expected but in practice there was a close correlation between trigone measurements derived from USS and iuMRI as shown by the data from the MERIDIAN Study.3 There was categorical agreement (mild, moderate or severe) in 84% of cases and 81% of USS and iuMRI measurements were within 2 mm of each other. In addition, we did not confirm the suspicion that trigone measurements are consistently larger on iuMRI, as the differences were broadly equal in both directions, indicating that there is no tendency for iuMRI to systematically underestimate or overestimate the trigone size compared with USS.
Ventriculomegaly is routinely defined as a trigone measurement of ≥10 mm as the cut-off of 10 mm indicates approximately 4 SD above the mean USS measurements and, using that definition, ventriculomegaly is by far the the most common intracranial abnormality detected antenatally. Ventriculomegaly was confirmed in 74% of the 570 fetuses in the primary MERIDIAN cohort and in the majority of cases ventriculomegaly was the only intracranial finding (306/570–54% of cases). Mild ventriculomegaly accounted for 80% of those cases with smaller numbers of moderate (12%) and severe ventriculomegaly (8%). In a small number of cases there were relevant other findings, such as somatic abnormalities (5%) and chromosomal/genetic abnormalities (4%).3 4 One of the major benefits of iuMRI was shown in the cases with USS-diagnosed IMVM because 5.7% of those fetuses had other brain abnormalities that were correctly shown on iuMRI in the majority of fetuses with an overall diagnostic accuracy of over 99% in such cases. Most of the iuMRI-derived diagnoses had substantial effects on clinical management.
In the original study, developmental or mortality data were available in 268 children; 78 had died in utero or postnatally. Of the 190 survivors, 88 children were assessed with BSID3, 175 with ASQ and 11 from case note review. The BSID is a formal, developmental assessment validated in US and UK cohorts that produces a composite score with a mean of 100 and a SD of 15, and allows calculation of centiles for development. As such, it is a robust developmental assessment test, although there are concerns the correlation been BSID3 and earlier editions and later developmental outcomes is weak.14–17 In contrast, the ASQ is a screening test, which produces a relatively high number of false positives and is designed to have a low false negatives rate. Sensitivity ranges from 41% to 95% and specificity from 32% to 84% in the largest studies.18–22 Eighty-four participants had both BSID3 and ASQ3 assessments. In these participants, the results from BSID3 were preferred, as it is a formal developmental assessment, rather than the ASQ3. The present study focuses on fetuses in whom IMVM was the only finding on USS and confirmed on iuMRI. Most of the published literature describes poor neurodevelopmental outcomes in <10% of cases in this situation, with more recent papers quoting a <5%. The results of the MERIDIAN Study were less optimistic as 19/86 (22%) children with antenatal IMVM having abnormal neurodevelopmental assessments.7 The subset of those cases reported in this study had poor neurodevelopmental outcomes in 17%. The most obvious explanations for the variance between the published literature and the MERIDIAN Study results include selection bias, and the use of a developmental screening test, which has known false positives (ASQ3).7
Although there is a clear signal in the literature towards a ‘favourable’ outcome (defined as >90% chance of a good outcome in the MERIDIAN Study) there is considerable variation in the information fetal medicine clinicians provided to parents about fetuses with IMVM. Clinicians who recruited into the MERIDIAN Study were approached before the study opened and asked what prognostic information they would give about a fetus with IMVM. All said ‘favourable’ and when asked to define ‘favourable’ 64% said >90% and 36% said >95% chances of normal outcome. However, when the actual prognostic information of the 312 cases of IMVM from the MERIDIAN Study was analysed, 24% did not say ‘favourable’ (‘normal’—2%, ‘intermediate’—17%, ‘don’t know’—5%).5 We can’t explain this variance but we assume there must have been other factors that influenced their opinion not captured by the study. This highlights the difficulty in giving prognostic information to parents with a fetus with IMVM.
In common with most other studies, we found a marked male preponderance, although our sex ratio (m:f 3.5:1) was higher than previous reports that range between 1.3:1 and 3.25:1.23–27 Some authors have suggested a connection between this finding and the widely held view that male fetuses are more likely to have neurodevelopmental problems.27 We are reluctant to enter into that discussion because of the relatively small numbers in our study but we have shown a slightly higher frequency of normal neurodevelopmental outcomes in male fetuses with IMVM (approximately 85%) when compared with female fetuses (78%). The published literature reports that normal male fetuses have larger trigones of the lateral ventricles when compared with female fetuses and our analysis of the 200 normal fetuses suggests that male fetuses have larger overall VV at every gestational age studied (manuscript in preparation). It is important to remember that the arbitrary 10 mm cut-off between normal and abnormal ventricle sizes is not sex-dependant, so it is perhaps not surprising that there is a male preponderance in fetuses with IMVM if male fetuses normally have larger ventricles than female fetuses. Although we agree that male fetuses are more likely to have developmental delay, our data do not suggest that it is anything to do with a higher rate of IMVM defined by an arbitrary 10 mm trigone measurement.
We were not aware of indicators on iuMRI that contribute to antenatal risk stratification for ‘normal’ and ‘abnormal’ neurodevelopmental outcomes before the start of this study. Possibly the most important finding of this study is the relationship between clinical outcome and the extent of IMVM in terms of being either unilateral or bilateral. Previous studies and meta-analyses based on USS have suggested that outcomes are similar between unilateral and isolated ventriculogegaly (VM)26 28–33 but the potential problem of diagnosing unilateral ventriculomegaly on USS is discussed below. That is in marked contrast to the current study in which there were no fetuses with unilateral IMVM with abnormal neurodevelopmental outcomes, in contrast to 37% abnormal outcomes in fetuses with bilateral IMVM. This is an important and potentially clinically relevant finding as unilateral IMVM was present in well over half of the fetuses in our study. We cannot claim that our study is sufficient to confirm this finding and the differences between our results may represent the different definitions of mild VM, ages at time of assessment, recruitment methods and developmental assessments used. Although the MERIDIAN Study was a prospective, hypothesis-driven study we did not hypothesise that unilateral IMVM would be associated with better clinical outcomes when compared with bilateral IMVM and so the current study was not formally powered to address this issue and indeed the number of cases we report is unlikely to be sufficient. However, these findings, and the flaws with the published data, should provide the basis of a prospective study with in-depth developmental assessment to test the hypothesis that fetuses with unilateral IMVM have better clinical outcomes when compared with fetuses with bilateral IMVM.
The potential importance of the extent of IMVM (in terms of unilateral and bilateral involvement) highlights the pivotal role of iuMRI in the assessment of fetuses with IMVM. Our previous work argued that a woman with a fetus with apparent IMVM on antenatal USS should have iuMRI because of the high rate of detecting other brain abnormalities. If the extent of ventriculomegaly in terms of unilateral/bilateral involvement is confirmed to be important for prognostication, iuMRI becomes more important for two reasons. First, the presence of ‘near-field’ artefacts on USS in the hemisphere closest to the transducer, coupled with progressive ossification of the fetal skull can result in suboptimal or non-visualisation of the proximal lateral ventricle.34 Hence, the delineation of ‘unilateral’ or ‘bilateral’ ventriculomegaly can be unreliable on USS and the ability to see both sides of the brain with equal clarity is a major advantage of iuMRI. Second, there are some unilateral pathologies that can cause unilateral ventriculomegaly which require iuMRI for full assessment, which can be either developmental in nature (such as hemimegaencephaly or unilateral polymicrogyria) or acquired (such as ischaemic or haemorrhagic stroke).
A further important, but negative, finding in the present study was the lack of association with any changes in VV, TBV, EAV and TICV and the rate of poor developmental outcome. Again, our study was not powered to address this issue in a formal fashion but our results give no hint that there may be a connection with changes in intracranial compartmental volumes and neurodevelopmental outcome. If this is subsequently confirmed it will be perhaps fortunate because the techniques for assessing intracranial compartmental volumes are time-intensive and not widely available.
In summary, we have studied a possible association between a range of iuMRI-based findings and neurodevelopmental outcome in children who had IMVM in utero. The most important finding is the apparent high chance of good neurodevelopmental outcome in fetuses with unilateral IMVM. We hope our findings will form the basis of a prospective, formally powered study to confirm or refute our findings.
Data availability statement
Data are available upon reasonable request. Requests for patient-level data and statistical code should be made to the corresponding author and will be considered by members of the original trial management group, including the chief investigator and members of CTRU, who will release data on a case-by-case basis. Data will be shared following the principles for sharing patient-level data as described by Smith et al (2015) . The data will not contain any direct identifiers; we will minimise indirect identifiers and remove free-text data, to minimise the risk of identification.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was obtained from the Yorkshire and the Humber – South Yorkshire ethics committee (11-YH-0006).
Acknowledgments
The authors thank the members of their Trial Steering Committee and Data Monitoring and Ethics Committee for the support and advice.
References
Footnotes
Contributors PDG, CM, NE and ARH conceptualised and designed the work. All others were involved in the acquisition of data. PDG analysed the data. PDG, DJC, NE and ARH were involved in the interpretation of data for the work. PDG and CM drafted the work and DJ, DJC, NE and ARH revised it critically for important intellectual content. PDG is the guarantor.
Funding This project was funded by the National Institute for Health Research (NIHR) Health Technology Assessment Programme (project number 09/06/01).
Disclaimer The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Health Technology Assessment Programme, NIHR, National Health Service, or the Department of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.