Article Text

Abstract
Objective To determine the change in non-invasive ventilation (NIV) use over time in infants born at <32 weeks’ gestation and the associated clinical outcomes.
Study design Retrospective cohort study using routinely recorded data from the National Neonatal Research Database of infants born at <32 weeks admitted to neonatal units in England and Wales from 2010 to 2017.
Results In 56 537 infants, NIV use increased significantly between 2010 and 2017 (continuous positive airway pressure (CPAP) from 68.5% to 80.2% in 2017 and high flow nasal cannula (HFNC) from 14% to 68%, respectively) (p<0.001)). Use of NIV as the initial mode of respiratory support also increased (CPAP, 21.5%–28.0%; HFNC, 1%–7% (p<0.001)).
HFNC was used earlier, and for longer, in those who received CPAP or mechanical ventilation. HFNC use was associated with decreased odds of death before discharge (adjusted OR (aOR) 0.19, 95% CI 0.17 to 0.22). Infants receiving CPAP but no HFNC died at an earlier median chronological age: CPAP group, 22 (IQR 10–39) days; HFNC group 40 (20–76) days (p<0.001). Among survivors, HFNC use was associated with increased odds of bronchopulmonary dysplasia (BPD) (aOR 2.98, 95% CI 2.81 to 3.15) and other adverse outcomes.
Conclusions NIV use is increasing, particularly as initial respiratory support. HFNC use has increased significantly with a sevenfold increase soon after birth which was associated with higher rates of BPD. As more infants survive with BPD, we need robust clinical evidence, to improve outcomes with the use of NIV as initial and ongoing respiratory support.
- neonatology
- intensive care units
- neonatal
- epidemiology
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party through the National Neonatal Research Database with relevant approvals. The National Neonatal Research Database is a National Data Asset, a registry containing the Neonatal Data Set (a National Data Standard). Details of data items are searchable at the following webpage: https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/publications-and-notifications/standards-and-collections/isb-1595-neonatal-data-set.
Statistics from Altmetric.com
What is already known on this topic?
Non-invasive ventilation (NIV) is being used increasingly to provide respiratory support to very preterm infants.
While continuous positive airway pressure (CPAP) remains the mainstay of NIV, high flow nasal cannula oxygen (HFNC) is a popular mode of NIV and clinicians have reported increasing preference of using HFNC.
What this study adds?
NIV support, particularly HFNC, in very preterm infants increased significantly between 2010 and 2017 in England and Wales.
HFNC is increasingly used as initial respiratory support in extremely preterm infants, although there is a high rate of such infants requiring CPAP or mechanical ventilation within 7 days.
Introduction
In very preterm infants, increased use of antenatal steroids, early surfactant and attempts to minimise lung injury have encouraged increased use of non-invasive ventilation (NIV).1 Modalities such as nasal continuous positive airway pressure (CPAP) that provide a set distending pressure prevent some adverse effects associated with mechanical ventilation.2 Similarly, high flow nasal cannula oxygen (HFNC), which delivers a set gas flow, rather than a set distending pressure, has become increasingly popular.3
Continuous distending pressure directly, or generated via a continuous flow of oxygen-air mixture, stabilises the upper airway, maintains lung volumes and stimulates upper airways to maintain a respiratory drive.1 These mechanisms can reduce the need for prolonged invasive ventilation and may reduce the risk of bronchopulmonary dysplasia (BPD) and other ventilator-induced lung injuries.4 Meta-analyses suggest that, when used for initial respiratory support or as respiratory support after extubation, HFNC and CPAP are not different when comparing the risks of BPD and death in preterm infants.5 Both are now frequently used. Although UK clinicians report increased use of HFNC,6 there are no data quantifying the change in use of NIV in actual practice.
We aimed to quantify the change in use of NIV in infants born at <32 weeks’ gestation across England and Wales from 2010 to 2017 and analysed the association between these changes and clinical outcomes.
Methods
We performed a retrospective cohort study of infants born at <32 weeks’ gestation in England and Wales from 1 January 2010 to 31 December 2017 inclusive, whose data are held within the UK National Neonatal Research Database.7 8
Infants were excluded if there were missing data as described in online supplemental figure 1 and online supplemental table 1.7
Supplemental material
Exposures
From variables that record types of respiratory support received (invasive ventilation, NIV, supplemental oxygen, type of NIV), we identified infants who received any NIV (online supplemental table 1). Infants who received NIV were divided into two groups— those who received HFNC for any length of time (HFNC group) and those who received CPAP and had no record of receiving HFNC (CPAP-only group). Infants in the HFNC group may have received CPAP also.
Outcomes
BPD was defined as requiring any supplementary oxygen or respiratory support at 36 weeks’ corrected gestational age (CGA) (infants who died before 36 weeks were excluded).9 Other preplanned outcomes and their definitions are given in online supplemental table 1.
Statistical analysis
All data management and analyses were performed using STATA, V.15.1 (StataCorp, College Station, Texas, USA). After exclusions, we quantified the percentage of all admissions each year where HFNC was used, both for all infants and for two prespecified subgroups: those born at <28 weeks’, and those born at 28–31 weeks’ gestation. We compared the study groups, including demographic, pregnancy and delivery details, and the NMR-2000 score to describe infants’ risk of in-hospital mortality.10
We quantified and described changes in the highest mode of respiratory support received on the first day after birth. We described the percentage who subsequently ‘failed’ on the initial mode as those who had escalation of respiratory support within 7 days that is, for those on HFNC initially, if they received CPAP and/or mechanical ventilation and for those on CPAP initially, if they received mechanical ventilation. Where HFNC was not the initial mode of respiratory support, we quantified subsequent exposure to HFNC. Change in use over the study period (2010–2017) was analysed using the χ2 test for trends.
We used logistic regression for binary variables and quantile regression for continuous variables to explore the association between study groups and the prespecified outcomes. ORs and median differences were adjusted for: gestational age (GA) group (<28 weeks’ gestation or 28–31 weeks’ gestation); sex; birth weight for age z-score (<−2 SD or ≥−2 SD or between <2 SD and ≥−2 SD); exposure to antenatal steroids; NMR-2000 category (low risk, medium risk or high risk)10; need for mechanical ventilation on day 1 and year of admission. Any missing data for confounding variables were treated as separate categories and infants retained in the models. We used a robust variance estimator to account for clustering of infants within units. All p values were two-sided, significance was set at p<0.05 and we used a Bonferroni correction to account for multiple testing. A predefined subgroup analysis was performed for all outcomes for infants born at <28 weeks’ gestation and those born at 28–31 weeks’ gestation.
Results
From the population of 63 210 infants born at <32 weeks’ gestation, 56 537 infants were retained after exclusions (online supplemental figure 1). Of these, 45 898 infants received NIV.
Non-invasive ventilation (CPAP or HFNC) on day of birth
On the day of birth, 16 308/56 537 (28.8%) infants received NIV, which included 1065/17 061 (6.2%) infants of <28 weeks’ and 15 243/39 476 (38.6%) infants of 28–31 weeks’ GA. During the study period, those who received NIV on the first day increased from 1457/6479 (22.5%) to 2598/7401 (35.1%). This increase was larger among the 28–31 weeks’ GA group ((from 1357/4570 (29.7%) to 2471/5194 (46.5%)) as compared with that among infants <28 weeks’ GA (from 100/1909 (5.2%) to 181/2216 (8.2%)).
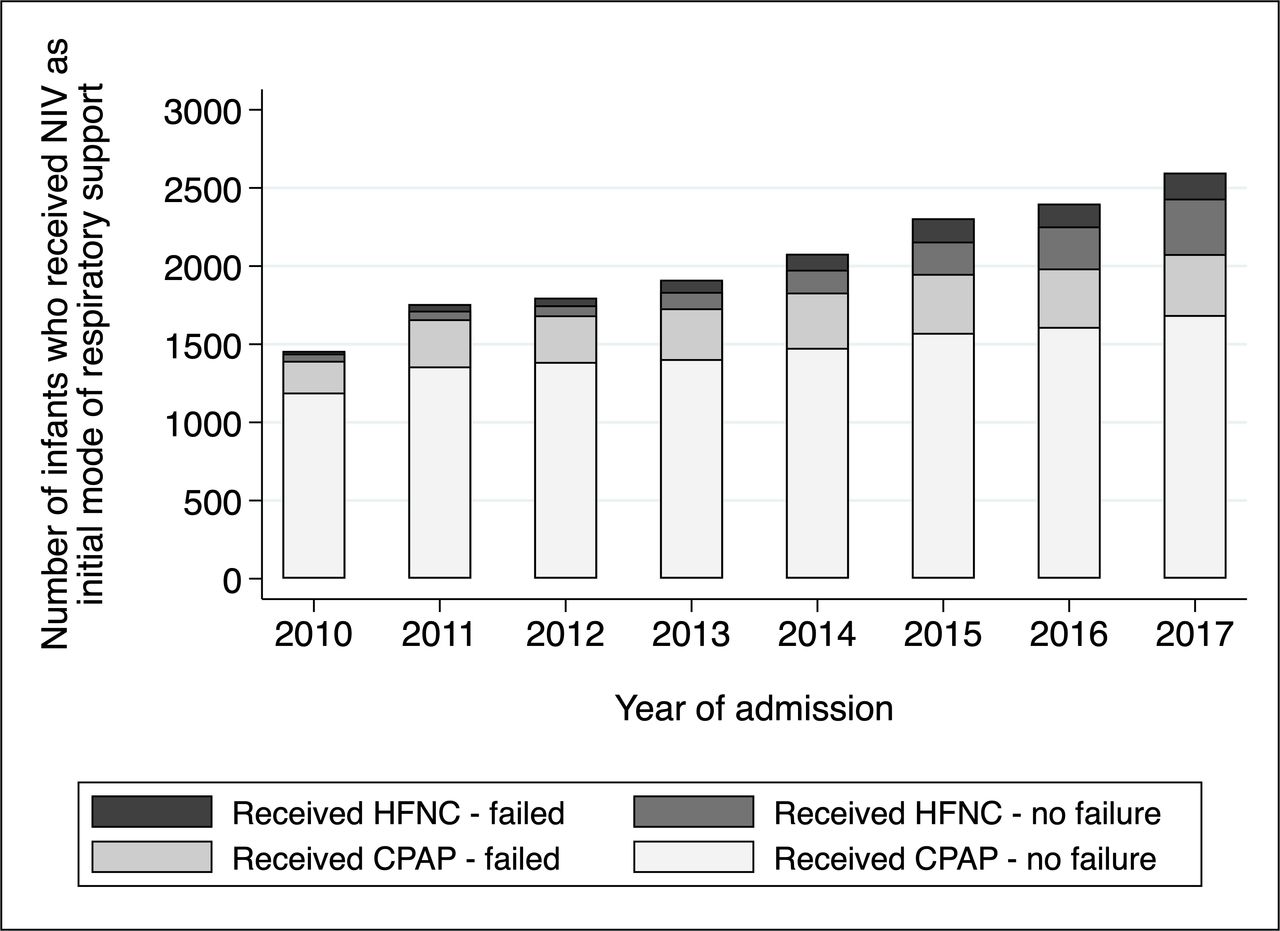
Figure 1 shows the respiratory support received by the infants on the first day (initial respiratory support) from 2010 to 2017. The percentage receiving CPAP increased 1.3-fold from 21.5% to 28.0% while HFNC use increased by 7-fold from 1.0% to 7.0%. This increase was seen both in infants born at <28 weeks’ and those born at 28–31 weeks’ GA, though the magnitude of increase was greater among the latter (table 1).

Use of HFNC as the initial mode of respiratory support in infants born at <32 weeks' gestational age in England and Wales (2010–2017). Failure refers to escalation of respiratory support within 7 days, that is, HFNC failed refers to those infants who received HFNC as the initial mode of respiratory support but needed CPAP and/or mechanical ventilation within 7 days and CPAP failed refers to those who received CPAP as the initial mode of respiratory support but needed mechanical ventilation within 7 days. Image created by authors using STATA, V.15.1 (StataCorp, College Station, Texas, USA). CPAP, continuous positive airway pressure; HFNC, high flow nasal cannula; NIV, non-invasive ventilation.
NIV support use on day of birth and rates of requiring escalation in respiratory support within 7 days in infants born at <32 weeks’ gestation from 2010 to 2017 in England and Wales
CPAP was used as initial support in 14 312/56 537 infants (25.3% of all admissions), of whom 18.3% (n=2623/14 312) went on to receive mechanical ventilation within 7 days (table 1). The failure rate was higher among infants born at <28 weeks, of whom 263/836 (31.5%) were ventilated within 7 days compared with 2360/13 476 (17.5%) infants born at 28–31 weeks.
HFNC was used as the initial respiratory support in 1996/56 537 infants (3.5% of all admissions); 748/1996 (37.5%) went onto receive CPAP (n=571/1996 (28.6%)) or mechanical ventilation (n=347/1996 (17.4%)) within 7 days, including 170/1996 (8.5%) who received both CPAP and mechanical ventilation. The failure rate was higher among the more immature infants (<28 weeks’ GA: 135/229 (59.0%), including 84/229 (36.7%) who were mechanically ventilated; 28–31 weeks’ GA: 613/1767 (34.7%), including 263/1767 (14.9%) who were mechanically ventilated). Among the infants who received HFNC on the first day, those who ‘failed’ included more infants who were extremely preterm, that is, <28 weeks’ GA (135/784 (18.0%) vs 94/1248 (7.5%); p<0.001); of lower birth weight (1285 (346) g vs 1396 (318) g; p<0.001); multiple births (35.2% vs 28.2%; p=0.001); born by caesarean section (64.7% vs 55.4%; p<0.001); had prolonged rupture of membranes (17.8% vs 28.6%; p<0.001) and who had not had surfactant (15.0% vs 9.5%; p<0.001). There was no difference in the sex of the infants or receipt of antenatal steroids.
CPAP use during neonatal care
The use of CPAP at any point during an infant’s stay in neonatal care significantly increased from 68.5% infants in 2010 (n=4439/6479) to 80.2% in 2017 (n=5941/7410) (χ2 test for trend p<0.001). Further data on the use of CPAP in infants who received mechanical ventilation as initial respiratory support are described in table 2.
Use of HFNC and CPAP for respiratory support following support with mechanical ventilation and/or CPAP in infants born at <32 weeks’ gestation in England and Wales (2010–2017)
HFNC use during neonatal care
The use of HFNC at any point significantly increased from 14.3% of infants in 2010 (n=928/6479) to 68.0% in 2017 (n=5039/7410) (figure 2, p<0.001). The increase in percentage of infants who received mechanical ventilation or CPAP as their initial respiratory support and then went on to receive HFNC, and data demonstrating earlier and more prolonged use of HFNC, are described in table 2.

{kind=link}
{kind=link}
Percentage of all infants born at <28 weeks’ gestational age (GA) and those born at 28–32 weeks’ GA in England and Wales (2010–2017) who received any high flow nasal cannula oxygen (HFNC) during their neonatal care. Image created by authors using STATA, V.15.1 (StataCorp, College Station, Texas, USA).
Clinical outcomes associated with use of CPAP and HFNC
There were 18 926 infants who had CPAP only and 26 936 infants who received any HFNC (online supplemental figure 1). Infants receiving HFNC were more immature and smaller at birth, more were exposed to antenatal steroids and received surfactant while a smaller proportion were delivered by caesarean section, were multiple births and were less likely to be born to mothers who had prolonged rupture of membranes (online supplemental table 2).
The outcomes are shown in table 3 and by subgroup in online supplemental tables 3 and 4. The odds of death before discharge were significantly higher in infants who had CPAP only compared with those who had any HFNC (adjusted OR (aOR) 0.19 (95% CI 0.17 to 0.22)). Infants who had CPAP only died at an earlier chronological age than those who received HFNC (median (IQR) age of death: CPAP group, 22 (95% CI 10 to 39) days; HFNC group, 40 (95% CI 20 to 76) days; p<0.001) (online supplemental figure 2). Excluding deaths before 36 weeks’ CGA, 3136/18 003 (17.4%) infants who had CPAP only developed BPD compared with 12 336/26 260 (47.0%) who received any HFNC. The odds of developing BPD were significantly higher in the HFNC group (adjusted aOR 2.98 (95% CI 2.81 to 3.15)). Infants who had HFNC spent significantly longer on respiratory support, had longer hospital stay, higher odds of NEC and other complications as compared with those who had CPAP only (table 3).
Clinical outcomes in infants who received NIV from 2010 to 2017 in England and Wales: comparison between those who received any HFNC versus those who had CPAP only
Discussion
We found that, in England and Wales, there have been significant changes in the use of NIV in very preterm infants with substantial increase in use of HFNC from <15% of all infants born at <32 weeks’ gestation in 2010 to 68% in 2017, both as initial respiratory support (from 1% to 7%) and as support received later (from 15.7% to 69.8%). This is similar to the trend seen in Australia and New Zealand.11
Use of NIV on the day of birth has increased from 22% to 35% over the study period although, overall, only 8% of those born <28 weeks’ gestation received NIV on this day. In an Australia-New Zealand cohort (2007–2013), 29% of infants <29 weeks’ gestation received CPAP for initial respiratory support, 43% of whom required mechanical ventilation within 72 hours.12 The overall CPAP failure rate was lower in our cohort (31%) even though we measured failure over a longer 7-day period. Systematic reviews of randomised controlled trials (RCTs) comparing early prophylactic CPAP with mechanical ventilation show a nearly 50% reduction in need for mechanical ventilation.13 Our data demonstrate a more conservative use of CPAP as the initial respiratory support in England and Wales.
The Cochrane systematic review did not find any study that investigated the use of HFNC as the initial mode of respiratory support in infants <28 weeks’ gestation while other reviews reported that HFNC has higher failure rates than CPAP when used as first-line support in <28 weeks’ gestation infants.14 15 We found that 60% of <28 weeks’ gestation infants who received HFNC as initial support subsequently required escalation of support within 7 days, compared with 31.5% of the CPAP group. In the subgroup of infants born at 28–31 weeks’ gestation, 34.7% who received HFNC as initial mode required escalation within 7 days. This is similar to the 32.9% failure rate for HFNC among 28–31 weeks’ gestation infants reported by Roberts et al 16 in an RCT that was stopped early due to the high rate of HFNC treatment failure. When CPAP was used as initial mode of respiratory support, we found that 17.5% were ventilated within 7 days, similar to the rate reported by Roberts et al (16.1%), although they measured rates of intubation up to 72 hours only. HFNC use as the initial respiratory mode is increasing in popularity particularly in more mature infants. In a two-centre study in the UK, Zivanovic et al, found that use of HFNC without the need for CPAP as ‘rescue’ was successful in preventing intubation in infants between 28 and 36 weeks’ gestation.17
Similarly, we found an increase in the use of HFNC later in neonatal care with significant increases in the number of infants who received any HFNC and the number of days on HFNC per infant. In addition, we also found that HFNC was given increasingly earlier with 12 days difference in initiation between 2010 and 2017.
We analysed the associations of these changes in practice with clinical outcomes and found higher mortality among infants who never received HFNC. Among those who survived to 36 weeks’ CGA, we found that the adjusted odds of BPD were significantly higher among those who received HFNC compared with those who had CPAP only. Infants in the CPAP only group died significantly earlier than those in the HFNC group. It is possible that attending clinicians did not choose HFNC for infants with more disease in the first few weeks of life. Such infants remained on mechanical ventilation or CPAP and may have died before they were considered well enough to receive HFNC. The survivors, particularly those who required prolonged respiratory support, were then more likely to receive HFNC, resulting in a higher rate of both survival and BPD among them. This suggests an element of confounding by indication, that is, the differences in outcome are related to the way a particular intervention is used rather than the intervention itself, which may explain some of the relationship between HFNC and death and HFNC and BPD. However, the use of HFNC may also be a step in the causal pathway18 of BPD. The variable and unregulated distending pressure generated by HFNC may cause uncontrollable overexpansion and/or atelectasis that aggravate lung injury leading to higher risks of BPD. Meta-analysis of RCTs showed no difference in BPD between HFNC and CPAP use, although the studies did not include many infants born at <28 weeks’ gestation.5 Our findings are similar to previous smaller observational studies.19
Other important clinical outcomes such as late onset sepsis, necrotising enterocolitis, patent ductus arteriosus, pneumothorax and retinopathy of prematurity were also more frequent in babies who received HFNC. Infants who received HFNC required respiratory support for longer and received in-hospital neonatal care for longer. Prolonged need for respiratory support with HFNC has been demonstrated in meta-analyses of RCTs5 and observational studies.19 20 Our study, due to its retrospective, observational design, cannot show a direct link between choice of NIV and any of the clinical outcomes we report. It has been suggested that the increased perceived patient tolerance, and ease of application and maintenance, may result in less urgency to wean leading to longer lengths of respiratory support and hospital stay.21
Our study of 56 537 infants, limited by observational design, cannot imply a causative link between HFNC and either reduced mortality or increased BPD as highlighted by Roberts et al.22 RCTs remain the gold-standard for demonstrating causation and clinical trials suggest that HFNC does not increase the risk of death or BPD compared with CPAP at least in the more mature population.5 However, outcomes in research trials can be superior to the same practice in clinical situations, possibly due to the greater level of control over patient selection and better adherence to treatment protocols in trial settings.23 The worse outcomes, such as increased odds of BPD, in observational studies may be a consequence of indication creep24 and outcomes may also vary with experience and training of practitioners. Careful patient selection and individualised application of HFNC may improve outcomes.
With a database that covers almost the entire population of England and Wales, we achieved a large sample size that enabled us to quantify the changes comprehensively and account for several confounding variables. In addition, we have accounted for multiple testing and used a robust variance estimator to account for clustering of infants within units. These make a robust observational study but do not remove the inherent limitation that associations do not imply causation.
Conclusion
NIV use is increasing. CPAP use increased 1.3-fold while HFNC use increased by 7-fold as respiratory support soon after birth. As more infants survive with BPD, we need clinical evidence and ongoing monitoring to ensure practice evolves in keeping with the best evidence to support the use of NIV as initial and ongoing respiratory support.
Data availability statement
Data are available on reasonable request. Data may be obtained from a third party through the National Neonatal Research Database with relevant approvals. The National Neonatal Research Database is a National Data Asset, a registry containing the Neonatal Data Set (a National Data Standard). Details of data items are searchable at the following webpage: https://digital.nhs.uk/data-and-information/information-standards/information-standards-and-data-collections-including-extractions/publications-and-notifications/standards-and-collections/isb-1595-neonatal-data-set.
Ethics statements
Patient consent for publication
Ethics approval
The dataset was created by the NDAU and this study was approved by Yorkshire & The Humber—Sheffield Research Ethics Committee (IRAS 259802).
Acknowledgments
Electronic patient data recorded at participating neonatal units that collectively form the United Kingdom Neonatal Collaborative are transmitted to the Neonatal Data Analysis Unit to form the National Neonatal Research Database (NNRD). We are grateful to all the families that agreed to the inclusion of their baby’s data in the NNRD, the health professionals who recorded data and the Neonatal Data Analysis Unit team.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrDonSharkey, @shaliniojha7
Contributors LSa: participated in the concept and design, performed the analysis of data, participated in interpretation of data and drafted the manuscript. LSz: participated in the concept and design, performed the analysis of data, participated in interpretation of data and drafted and revised the manuscript. TCK: participated in the concept and design, analysis of data and interpretation of data and revised the manuscript. DS: participated in the concept and design, analysis of data and interpretation of data and revised the manuscript. DAT: participated in the concept and design, interpretation of data and revised the manuscript. HB: participated in the concept and design, analysis of data and interpretation of data and revised the manuscript. SO: designed and conceptualised the study, participated in analysis and interpretation of data and drafted and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LSa was funded by the Health Education England, Academic Foundation Training Programme. SO has received funds from the National Institute of Health Research, UK and the Medical Research Council, UK for other research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.