Article Text

Abstract
Objective To identify risk factors associated with delivery room respiratory support in at-risk infants who are initially vigorous and received delayed cord clamping (DCC).
Design Prospective cohort study.
Setting Two perinatal centres in Melbourne, Australia.
Patients At-risk infants born at ≥35+0 weeks gestation with a paediatric doctor in attendance who were initially vigorous and received DCC for >60 s.
Main outcome measures Delivery room respiratory support defined as facemask positive pressure ventilation, continuous positive airway pressure and/or supplemental oxygen within 10 min of birth.
Results Two hundred and ninety-eight infants born at a median (IQR) gestational age of 39+3 (38+2–40+2) weeks were included. Cord clamping occurred at a median (IQR) of 128 (123–145) s. Forty-four (15%) infants received respiratory support at a median of 214 (IQR 156–326) s after birth. Neonatal unit admission for respiratory distress occurred in 32% of infants receiving delivery room respiratory support vs 1% of infants who did not receive delivery room respiratory support (p<0.001). Risk factors independently associated with delivery room respiratory support were average heart rate (HR) at 90–120 s after birth (determined using three-lead ECG), mode of birth and time to establish regular cries. Decision tree analysis identified that infants at highest risk had an average HR of <165 beats per minute at 90–120 s after birth following caesarean section (risk of 39%). Infants with an average HR of ≥165 beats per minute at 90–120 s after birth were at low risk (5%).
Conclusions We present a clinical decision pathway for at-risk infants who may benefit from close observation following DCC. Our findings provide a novel perspective of HR beyond the traditional threshold of 100 beats per minute.
- respiratory
- neonatology
Data availability statement
Data are available upon reasonable request. Sharing of data will be considered for specific research projects. Requests should be sent to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Delayed cord clamping supports the fetal-to-neonatal transition and is recommended for infants who are vigorous at birth.
Some infants nevertheless require respiratory support in the delivery room.
Failure to recognise delayed transition may result in neonatal morbidity.
What this study adds?
This study identifies risk factors associated with delivery room respiratory support in at-risk infants born at >35+0 weeks gestation who received delayed cord clamping.
A clinical decision pathway is presented for infants who may benefit from close observation after initially appearing vigorous.
Our findings call into question the neonatal heart rate threshold that should raise concern at births attended by paediatric doctors.
Introduction
Healthcare workers with skills in newborn resuscitation routinely attend births where the infant is at increased risk of requiring support. At hospitals in high-resource settings this commonly involves attendance by a paediatric doctor (paediatrician or paediatric trainee). The birth of a vigorous, crying infant is considered a reassuring sign and cord clamping is routinely delayed in accordance with international recommendations.1 2 It is not uncommon for the paediatric doctor to leave at this stage, at times following a limited assessment.
Delayed cord clamping (DCC) facilitates the fetal-to-neonatal transition by maintaining oxygen supply and left ventricular preload until the lungs are aerated.3 The majority of vigorous term infants will successfully initiate this cardiopulmonary adaptation during the first 60 s after birth,4 5 but some go on to develop respiratory distress. At low-risk births, the risk of delivery room respiratory support and neonatal unit admission after DCC ranges between 7% and 11% and between 3% and 5%, respectively.6 7
Delayed recognition of incomplete lung aeration and hypoxia is an important cause of neonatal unit admission and infant–mother separation.8 9 At the severe end of the spectrum, apparent life-threatening events may occur shortly after birth where the infant is found to be apnoeic and floppy during skin-to-skin contact with their mother. Unrecognised incomplete transition may play a role alongside increased vagal tone and positional airway obstruction for infants who deteriorate within the first few minutes after birth.10 11 Identification of infants who may need early respiratory support among the large number of at-risk infants who are initially vigorous and cry after birth is challenging.
There are no data to help risk-stratify infants who may require respiratory support after initially appearing vigorous and receiving DCC. Furthermore, there are no data on infant characteristics that may be assessed by the attending paediatric doctor during or immediately after DCC that may be predictive of risk. Closer observation of selected at-risk infants at the mother’s side may help avoid later deterioration. We therefore aimed to:
Identify risk factors associated with delivery room respiratory support for vigorous infants managed with DCC at >35+0 weeks gestation who were considered at risk prior to birth.
Describe the probability of delivery room respiratory support in relation to these risk factors.
Methods
We conducted a prospective cohort study at The Royal Women’s Hospital and Monash Medical Centre in Melbourne, Australia, between 5 August 2018 and 15 March 2020. Written informed parental consent was obtained for all participants. Deferred parental consent was obtained if the participant became eligible only immediately prior to an emergency birth when prospective consent could not be sought. This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology statement.12
Infants meeting the following criteria were eligible for inclusion:
Gestation ≥35+0 at birth.
Paediatric doctor requested by the obstetric or midwifery team to attend an at-risk birth as per local hospital policy (figure 1).
Researcher available to attend.
Infant vigorous at birth and received >60 s of DCC.

(A) Description of infants included in the study. *’At-risk’ is defined as birth at ≥35+0 weeks gestation with the presence of one or more perinatal risk factors for needing resuscitation at birth, requiring the attendance of a paediatric doctor as per hospital policy. (B) Criteria requiring paediatric attendance at birth for The Royal Women’s Hospital (RWH) and Monash Medical Centre (MMC). CS, caesarean section; GA, general anaesthesia.
The following were the exclusion criteria:
Fetuses with known congenital anomalies compromising cardiorespiratory transition. These were prespecified as congenital diaphragmatic hernia, hydrops fetalis, congenital heart defects and airway anomalies that may compromise the ability to provide facemask positive pressure ventilation (PPV).
Infants whose mothers were at high risk of obstetric complications mandating early cord clamping. These included abnormal placentation, abruption, suspected uterine rupture and coagulopathy.
Monochorionic twins and multiples >2.
Recruitment occurred in parallel with an ongoing randomised trial (figure 1).13
In accordance with study protocol, cord clamping was performed at ≥2 min after birth followed by oxytocic administration. Where there was concern regarding early maternal bleeding, cord clamping could be expedited by the maternal care team.
Immediately after birth and with the cord intact, a researcher dried the infant and placed three ECG chest leads and a preductal pulse oximeter to measure oxygen saturation. Monitoring was similar at both caesarean and vaginal births as previously described and continued for 10 min after birth.14 Heart rate (HR) and oxygen saturation were displayed on a portable Intellivue X2 (Philips Healthcare, USA) or Infinity M540 (Dräger, Germany) monitor which was visible to the clinician. The monitor screen and the NeoPuff (Fisher & Paykel Healthcare, New Zealand) manometer were captured using a GoPro Hero Session (GoPro, USA) and the video downloaded for offline data extraction. To ensure high fidelity, we manually extracted HR data at 10 s intervals until 10 min after birth. Data points with poor QRS waveforms were excluded. Data were extracted unblinded to the study outcome by two assessors trained by a single researcher (SB). We did not video-record the infant, but the researcher stated when events occurred after birth and this was captured by the audio recording.
We defined cases as infants who received any respiratory support, that is, PPV, continuous positive airway pressure or supplemental oxygen, within 10 min of birth. Controls comprised infants who did not receive respiratory support but included those who received stimulation or airway manoeuvres. The decision to provide respiratory support and the type of support were at the discretion of the attending paediatric registrar or resident trained in the Australian and New Zealand Committee on Resuscitation Neonatal Resuscitation Guidelines.15
Maternal and infant demographic details, perinatal characteristics, resuscitation measures and clinical outcomes were entered by the study researcher into an electronic study database (REDCap) immediately after birth.16
Analysis
There was no prespecified sample size. Recruitment for this study was concluded when the parallel randomised trial was paused during the COVID-19 pandemic.
For the comparative analysis we chose perinatal variables typically available within 2 min of birth that might predict the need for respiratory support based on clinical experience and previous studies.17–19 We used average HR between 90 and 120 s after birth as a predictive variable as it coincides with a time window when HR can be feasibly assessed following 60 s of DCC, particularly at caesarean births. However, as most infants in our study had cord clamping at 120 s, we did a sensitivity analysis using average HR between 120 and 150 s as a predictor variable to explore the immediate effect of cord clamping. A narrow time window was chosen to ensure limited variability in HR. We did not include 1 min Apgar score as a predictive variable as it is not typically tallied within 2 min of birth and was assigned by the clinician subsequent to the study primary outcome. Time to regular cries was extracted from the audio recordings and was defined as the time to hear the second cry after birth when this was followed by regular cries.
All analyses were performed in R V.3.6.2 (R Foundation, Vienna, Austria). For categorical variables comparison was performed using χ2 test unless otherwise specified. For continuous variables the mean (or median) was compared using a two-sided t-test (or a Mann-Whitney U test for skewed variables). In the adjusted analysis we used a backward stepwise log-binomial regression retaining variables with p<0.1. We report risk ratios and their respective 95% CIs for variables in the final model with p<0.05. To display the relationship between risk factors and the outcome, we used the final model to plot the fitted (predicted) probability of respiratory support within the observed range of values of the predictor variables.
Conditional inference decision trees were created using the partykit package.20 Decision trees have similar modelling ability to logistic regression with the advantage of generating an intuitive visual tool for clinical decision-making.21–23 In this analysis, the study population is recursively split into subgroups based on the predictive variables that are most strongly related to the outcome. Using a Bonferroni-adjusted p value the algorithm chooses which variables to split, their discriminatory value and the order in which the splitting occurs. Outcome discrimination can thus be maximised at each step by accounting for the relationships between variables while limiting both overfitting and biased variable selection.21 We used the default settings of the ‘ctree’ function, with no growth limit criteria for the minimum number of infants in each terminal node.
We explored post hoc the predictive accuracy of HR using receiver operating characteristic (ROC) analysis and used Youden’s method to validate the optimum cut-off threshold (pROC package).24
Results
All 298 infants meeting the eligibility criteria were included in the study. The median (IQR) gestational age was 39+3 (38+3–40+3) weeks. Cord clamping occurred at a median of 128 (123–145) s after birth.
Forty-four (15%) cases received respiratory support at a median (IQR) of 214 (156–326) s after birth. Of these 44 cases, 14 (32%) were admitted to the neonatal unit for respiratory support, compared with 3 of 254 (1%) in the control group (p<0.001). Participant characteristics and clinical outcomes are detailed in table 1.
Participant characteristics and clinical outcomes
Infants receiving respiratory support had a lower average HR between 90 and 120 s after birth and took longer to establish regular cries. Differences in gestational age and in 1 min and 5 min Apgar scores between cases and controls were statistically significant but of marginal clinical importance. Unadjusted comparisons for risk factors are shown in table 2, alongside the adjusted risk ratios from the regression model.
Univariable and multivariable analyses of characteristics associated with respiratory support in the delivery room
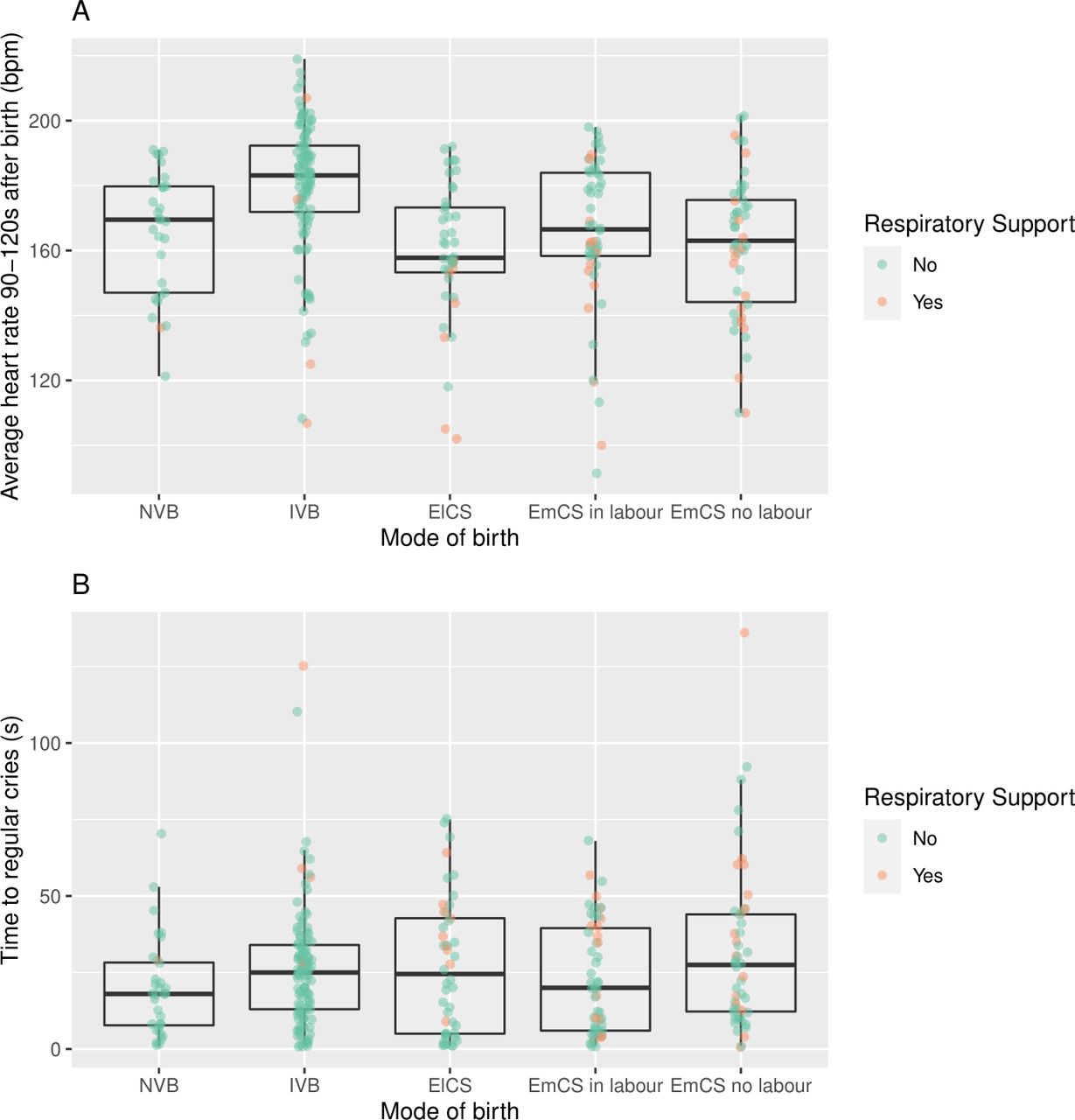
Among variables associated with respiratory support, only type of birth, average HR between 90 and 120 s after birth and time to establish regular cries contributed significantly to the multivariable model. Figure 2 summarises, for each mode of birth, the average HR between 90 and 120 s and time to regular cries.

Boxplots showing (A) the distribution of average heart rate 90–120 s after birth and (B) time to regular cries for each mode of birth. Dots represent individual infants who either did (red) or did not (green) receive respiratory support. bpm, beats per minute; ElCS, planned (elective) caesarean section; EmCS, unplanned (emergency) caesarean section; IVB, instrumental vaginal birth; NVB, normal vaginal birth.
Figure 3A shows a visualisation of a simplified multivariable model of the relationship between these variables and the predicted probability of respiratory support. In this model, normal and instrumental vaginal births are grouped together, as are unplanned caesarean sections both in and not in labour. This is to aid interpretability of the plot and was guided by the similarity in risk in the grouped variables. Model performance between the original and simplified models, assessed using Akaike information criterion (AIC), was similar (AIC 209 and 206, respectively). From the simplified model, for a <20% probability of respiratory support among infants who established regular cries within 30 s of birth, infants must have an average HR between 90 and 120 s greater than the following thresholds: for vaginal births, 110 beats per minute (bpm); for planned caesarean sections, 155 bpm; for unplanned caesarean sections, 176 bpm.

{kind=link}
{kind=link}
{kind=link}
Probability of delivery room respiratory support in relation to identified risk factors. (A) Predicted probability from the regression model. Each curve describes the predicted probability of respiratory support in relation to average heart rate between 90 and 120 s after birth for the following modes of birth: unplanned emergency caesarean sections both in and not in labour grouped together (EmCS, green), planned elective caesarean sections (ElCS, blue), and normal and instrumental vaginal births grouped together (VB, red). The upper margin of the shaded area for each mode of birth corresponds to the modelled probability of respiratory support when time to regular cries=60 s, the lower margin the modelled probability when time to regular cries=0 s, and the middle line the probability when time to regular cries=30 s. Ninety-five per cent of infants in the cohort had time to regular cries within this range. Dots represent individual infants who either did (plotted at y=1) or did not (plotted at y=0) receive respiratory support. 15 infants had no data for average heart rate between 90 and 120 s. (B) Decision tree. Average heart rate between 90 and 120 s after birth (Average_HR_90_120 s) in beats per minute, type of birth and time to regular cries (Time_Reg_Cries) in seconds were the most discriminatory variables in the study population. The probability of receiving respiratory support at each terminal node is shaded in black. bpm, beats per minute; ElCS, planned elective caesarean section; EmCS, unplanned emergency caesarean section; HR, heart rate; VB, normal or instrumental vaginal birth.
Using decision tree analysis, we found that the most discriminatory variable for the outcome of respiratory support was the average HR between 90 and 120 s after birth (figure 3B). The best cut-off value was 165 bpm. Infants with HR above this threshold were at low risk (9 of 186, 5%). Infants with HR below this threshold born by planned elective or unplanned emergency caesarean birth were at highest risk (31 of 80, 39%). Infants with HR below this threshold born by vaginal birth (which included normal vaginal and instrumental births) who established regular cries after 28 s were at intermediate risk, but numbers were small (3 of 13, 23%). Infants with HR below this threshold born by vaginal birth who established regular cries before 29 s remained at low risk (0 of 19, 0%).
Using receiver-operator curve analysis, we confirmed the optimal HR discriminatory threshold as 164 bpm in a post-hoc analysis. At this value, sensitivity was 70%, specificity 79%, positive predictive value 32% and negative predictive value 95%. Overall the area under the curve was 0.76 (online supplemental figure 1).
Supplemental material
Given the predictive value of both type of birth and HR, we constructed additional decision trees stratified by type of birth (online supplemental figure 2). For planned caesarean and unplanned caesarean births, the most discriminatory variable was again the average HR between 90 and 120 s after birth, but the thresholds were different: 157 bpm and 165 bpm, respectively. For vaginal births, the best predictor of respiratory support was time to regular cries ≥45 s.
The above analyses were performed using average HR between 90 and 120 s as a predictor variable, corresponding to the timepoint just before cord clamping in the majority of infants. As assessing HR may be more feasible subsequent to cord clamping, and to explore whether cord clamping had an immediate effect on the predictor variables, we ran the regression model and decision tree analyses using average HR between 120 and 150 s as a predictor variable in a post-hoc sensitivity analysis. The results were similar, with HR being the strongest predictor of respiratory support, alongside type of birth and time to regular cries (online supplemental figures 3–5). Decision tree and receiver-operator curve analysis identified the optimum HR threshold as 161 bpm (online supplemental figure 1).
Discussion
To our knowledge, this is the first study to evaluate the risk factors for delivery room respiratory support following DCC at births commonly attended by paediatric doctors. We found that the mode of birth along with early assessment of HR and time taken to establish regular cries were predictive of infants at risk.
Previous studies that evaluated perinatal risk factors for resuscitation included infants who were non-vigorous at birth and unsuitable for DCC.17–19 These studies were aimed at informing which births should have a paediatric doctor attend. Apart from Aziz et al,17 these studies focused on the wider group of all births, not just those attended by paediatric doctors. Our study instead focused on a different, at-risk cohort, where a paediatric doctor was in attendance at a birth of a vigorous infant who received DCC and aimed to inform when clinicians should remain vigilant. Comparing our cohort with the DCC arm of previous randomised trials that almost exclusively enrolled low-risk normal vaginal and planned caesarean births, the incidence of respiratory support and admission for respiratory distress was higher in our cohort (15% vs 7%–11% and 6% vs 3%–5%, respectively).6 7 One in three infants in our cohort who received respiratory support were admitted to the neonatal unit admission for respiratory distress, indicating a strong association with clinically important outcomes.
Animal studies describing the physiology of fetal-to-neonatal transition have shown that the newborn must clear lung liquid and achieve adequate lung aeration.25 26 It is therefore unsurprising that infants born by caesarean section, who have a greater quantity of lung liquid to clear, were at increased risk of receiving respiratory support.27 28 This is particularly the case when labour has not been established, as the physiological changes that aid the resorption of lung liquid have not occurred.29 Crying increases the hydrostatic pressure gradient between the airways and surrounding tissue for liquid clearance.26 Our finding that time taken to establish regular cries was associated with respiratory support therefore aligns with the physiology of newborn transition. Delayed establishment of regular cries may, however, also be a consequence of hypoxia, which in the newborn results in reduced breathing effort.30
DCC maintains placental oxygen supply and cardiac preload.3 However, there is likely to be a spectrum of oxygenation and lung aeration, particularly at births attended by paediatric doctors where the placental circulation may be compromised. Accordingly, we found significant variation in infant HR between 90 and 120 s after birth. This timepoint was prior to cord clamping in nearly all infants. HR is influenced by several factors, including autonomic drive, cardiac preload and temperature, but is particularly sensitive to hypoxia in the newborn.31 32 A relatively low HR may therefore correspond with infants at the lower end of the spectrum of oxygenation and lung aeration.
Most striking was our finding that the infant’s HR between 90 and 120 s after birth was the most important predictor of respiratory support. Regression analysis showed an inverse relationship between HR and risk of respiratory support, modified by the type of birth and time to establish regular cries. Decision tree analysis determined that the HR threshold with greatest discrimination for risk of respiratory support in the overall cohort, as well as among unplanned caesarean births, was 165 bpm. This threshold was lower for the subgroup of planned caesarean births (157 bpm). Our findings call into question the current paradigm of using a neonatal HR threshold of <100 bpm or <120 bpm to raise concern at births attended by paediatric doctors.1 Infants with HR >180 bpm, normally considered tachycardic, were at lowest risk of respiratory support. Our findings likely reflect an elevated level of fetal stress that is partly dependent on the type of birth, among births attended by paediatric doctors.
A limitation, therefore, is that our findings may have limited generalisability to lower-risk births that were not included in our cohort, where a lower HR threshold may apply. The risk factors and thresholds identified may therefore not apply to all births. An additional potential modifier of the HR threshold is temperature, which we did not measure shortly after birth. During the 2 min of DCC, infants born by caesarean were dried and loosely covered in a sterile drape, and all infants born by vaginal birth were held on the mother’s chest/abdomen. Additionally, single decision trees are prone to overfitting, particularly without external validation. Although we aimed to mitigate this using conditional inference trees alongside ROC analysis to determine the optimal cut-off for HR, we encourage others to validate our model in their delivery room settings. Consistent with our findings, Murphy et al 33 found that the average infant HR measured by ECG within 1 min at elective caesarean section births was close to 180 bpm. Infants in this study received early cord clamping. This randomised trial of ECG versus pulse oximetry, in addition to other observational studies, has shown that the previously reported bradycardia in a large proportion of vigorous infants within the first 2 min of birth is due to inaccuracy in readings from pulse oximetry.34–37 While our primary analysis investigated HR at a timepoint prior to cord clamping for most infants, the optimal discriminatory threshold was not substantially different when compared with the timepoint immediately after cord clamping. We extracted HR data unblinded to the study outcome, raising the possibility of observer bias. However, HR was measured objectively with ECG and data extracted at multiple (10-secondly) timepoints. Finally, we did not have data on respiratory distress, colour or tone within 2 min of birth. These characteristics may be assessed by some attending clinicians and may add discriminatory value for identifying at-risk infants.
While ECG-based HR measurement is considered the gold standard, ECG is not commonly used when an infant is vigorous at birth.38 Practical application of our findings would likely involve assessment of HR by auscultation. Auscultation has been shown to underestimate HR by 2–20 bpm and should be taken into account when applying our findings.39 40 Oxygen saturation data were not included as a predictor variable. While hypoxia may well be a useful marker, pulse oximetry is not routinely applied to births where the infant initially appears to transition well and would incur an additional cost and need for sterilisation at caesarean births.
Our results have implications for the large number of births attended by paediatric doctors. Routine HR assessment at around 2 min after birth, particularly at caesarean births, may help identify infants who would benefit from ongoing observation. While we did not document which births had early skin-to-skin contact, prospective studies are warranted to evaluate whether this monitoring could safely occur while the infant remains skin-to-skin with their mother. Some infants may require only stimulation and airway positioning, but 15%, approximately twice the proportion compared with low-risk births,6 7 may require respiratory support to prevent deterioration. Further work to prospectively validate the proposed decision pathway in a variety of settings is warranted prior to clinical application.
Data availability statement
Data are available upon reasonable request. Sharing of data will be considered for specific research projects. Requests should be sent to the corresponding author.
Ethics statements
Ethics approval
All study procedures were approved by the Human Research Ethics Committees at The Royal Women’s Hospital (reference number 17/19) and Monash Health (reference number RES-18-0000-035A).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception and design: SB, DAB, PGD, MT. Approvals and recruitment: SB, DAB, AW. Data acquisition and analysis: SB, DAB, GAS, AH. Interpretation and supervision: PGD, SBH, GRP, MT, AW. All authors participated in reviewing the data and editing the manuscript.
Funding This study was supported by the National Health and Medical Research Council (NHMRC) through a Programme Grant (#606789) and Fellowships (SBH: APP545921, GRP: APP1105526, PGD: APP1059111). SB is supported by an Australian Government Research Training Program Scholarship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.