Article Text

Abstract
Objective To compare the effect of two different automated oxygen control devices on target range (TR) time and occurrence of hypoxaemic and hyperoxaemic episodes.
Design Randomised cross-over study.
Setting Tertiary level neonatal unit in the Netherlands.
Patients Preterm infants (n=15) born between 24+0 and 29+6 days of gestation, receiving invasive or non-invasive respiratory support with oxygen saturation (SpO2) TR of 91%–95%. Median gestational age 26 weeks and 4 days (IQR 25 weeks 3 days–27 weeks 6 days) and postnatal age 19 (IQR 17–24) days.
Interventions Inspired oxygen concentration was titrated by the OxyGenie controller (SLE6000 ventilator) and the CLiO2 controller (AVEA ventilator) for 24 hours each, in a random sequence, with the respiratory support mode kept constant.
Main outcome measures Time spent within set SpO2 TR (91%–95% with supplemental oxygen and 91%–100% without supplemental oxygen).
Results Time spent within the SpO2 TR was higher during OxyGenie control (80.2 (72.6–82.4)% vs 68.5 (56.7–79.3)%, p<0.005). Less time was spent above TR while in supplemental oxygen (6.3 (5.1–9.9)% vs 15.9 (11.5–30.7)%, p<0.005) but more time spent below TR during OxyGenie control (14.7 (11.8%–17.2%) vs 9.3 (8.2–12.6)%, p<0.05). There was no significant difference in time with SpO2 <80% (0.5 (0.1–1.0)% vs 0.2 (0.1–0.4)%, p=0.061). Long-lasting SpO2 deviations occurred less frequently during OxyGenie control.
Conclusions The OxyGenie control algorithm was more effective in keeping the oxygen saturation within TR and preventing hyperoxaemia and equally effective in preventing hypoxaemia (SpO2 <80%), although at the cost of a small increase in mild hypoxaemia.
Trial registry number NCT03877198
- neonatology
- technology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Automated oxygen controllers, including the ones used in this study, increase time spent within the oxygen saturation target range compared with manual control.
Hypoxaemia and hyperoxaemia have been linked to morbidity and mortality in preterm infants.
What this study adds?
The OxyGenie controller was more effective in keeping the oxygen saturation within SpO2 target range than the CLiO2 controller.
With OxyGenie, less time was spent above target range, fewer hypoxaemic and hyperoxaemic episodes occurred, although with a small increase in time below target range.
Algorithm design influences how effective SpO2 targeting will be.
Introduction
Oxygen therapy for preterm infants with respiratory insufficiency aims to prevent or moderate the effects of hypoxaemia on the central nervous system, lungs and other organs. Conversely, the immaturity of the premature infant’s lungs, eyes and antioxidant system renders them vulnerable to exposure to supplemental oxygen, and hyperoxaemia has been linked to the development of bronchopulmonary dysplasia (BPD) and retinopathy of prematurity (ROP).1 2
Mindful of these morbidities, the inhaled fraction of oxygen (FiO2) is titrated manually, based on oxygen saturation (SpO2) readings derived from transcutaneous oximetry. Current guidelines recommend a lower limit for the SpO2 target range (TR) of at least 90% for the preterm infant,3 based on the recent NeOProM meta-analysis of individual patient data from large randomised controlled trials.4 These trials highlighted the potential impact of hypoxaemia and hyperoxaemia on preterm infants, with the lower TR (85%–89%) associated with an increased risk of mortality and necrotising enterocolitis and the higher TR (91%–95%) with an increased rate of ROP.
While the need to target an SpO2 range is widely accepted, data from cohort studies and randomised controlled trials point to the difficulty of SpO2 targeting by manual oxygen titration,5–10 with most studies reporting SpO2 values to be within the TR less than 50% of the time. Although bedside staff adjust the fraction of inspired oxygen (FiO2) relatively frequently to maintain SpO2 within TR, their workload limits time availability and makes it difficult to tailor FiO2 continuously to the infant’s need. This is compounded by the neonatal oxygenation physiology being unstable and non-linear with significant time delay between FiO2 adjustment and when SpO2 reaches a new stable level.11
Given both the importance and difficulty of SpO2 targeting, automated oxygen control (AOC) is a logical improvement on current practice. In essence, the concept is of an SpO2 input to a device holding a set of computational instructions (an algorithm), which then gives an output, an updated value for FiO2. Studies comparing automated oxygen titration systems with manual titration, conducted over short periods (2–24 hours per epoch), have demonstrated an absolute increase in the proportion of time spent with SpO2 within TR varying between 8% and 31%.12–23 A single study conducted in our institution has examined the effect of implementation of AOC as standard of care, finding a 14% increase in TR time in the postimplementation cohort, mostly related to a decrease in time above TR.24
Although several devices offering AOC are now commercially available and used in neonatal intensive care units (NICUs), comparisons between them are lacking. The NICU of the Leiden University Medical Center (LUMC) implemented AOC with the CLiO2 algorithm (Vyaire, Yorba Linda, California, USA) with the AVEA ventilator as routine care in August 2015. We recently replaced the AVEA ventilators with SLE6000 ventilators (SLE Limited, South Croydon, UK), which have the VDL 1.1 algorithm for AOC embedded as the “OxyGenie” option.17 25 This provided the unique setting where caregivers were competent to work with both ventilators, thus making feasible a safe comparison between the two oxygen controllers.
Based on described differences in the function of algorithms developed for AOC, it is likely that they will exhibit differences in performance.17 25 We recently observed that the CLiO2 algorithm was effective mostly in decreasing time above TR,24 whereas the first clinical study using OxyGenie reported a decrease in both time under and above TR and a virtual elimination of longer episodes outside the TR.23 We therefore hypothesised that the OxyGenie may be more effective than CLiO2 in maintaining SpO2 within the desired TR in preterm infants receiving respiratory support.
Methods
Study setting
We performed a randomised crossover trial in the NICU of the LUMC, a tertiary level neonatal unit with 25 NICU beds and 850 intensive care admissions per year. The Dutch Central Committee on Research Involving Human Subjects approved the study. Written informed parental consent was acquired prior to participation of each infant in the study.
Study population
Preterm infants born between from 24 weeks and up to and including 29 weeks of gestation who were receiving invasive mechanical ventilation or non-invasive respiratory support were assessed for eligibility . Initially, infants were considered eligible if they required supplemental oxygen with an FiO2 ≥0.25 at the time of enrolment and for at least 18 hours of the preceding 24 hours, but as the study progressed an alternative FiO2 eligibility criterion was added (FiO2 coefficient of variation ≥0.1 in the preceding 24 hours) to improve recruitment rate. Infants were excluded in case of major congenital anomalies or acute instability.
Automated oxygen control algorithms
The CLiO2 algorithm embedded in the AVEA ventilator is a hybrid rule-based adaptive controller. It makes initial FiO2 adjustments that are proportional to the difference between the measured SpO2 and the limits of the SpO2 TR. Subsequent adjustments also take into account this difference, as well as the SpO2 trend and basal oxygen requirement, the baseFiO2 . The baseFiO2 is periodically updated by interrogation of 5 min of recent SpO2 and FiO2 data where specific conditions are met, averaged along with the current baseFiO2 value.26
The OxyGenie algorithm embedded in the SLE6000 ventilator is an adaptive proportional-integral-derivative (PID) controller. The P, I and D terms each have separate coefficients, and in each case are adjusted from raw values to better suit the physiology of a neonate and account for the limitations of pulse oximetry. The basal FiO2, referred to as Reference FiO2 , is calculated every 30 min using 60 min of preceding FiO2 and SpO2 values.
Study procedures
A crossover design was used to study each infant on the same respiratory support mode. Infants received two consecutive study periods of 24 hours each, one with oxygen therapy under the control of the CLiO2 algorithm and the other with the OxyGenie algorithm, in random sequence. Web-based randomisation by Castor EDC (Castor, Amsterdam, The Netherlands) was used, stratified by mode of respiratory support (invasive or non-invasive) using variable (4, 6) block sizes. After the first study period, the alternative ventilator was substituted, and a washout period of 1 hour was applied before data recording restarted to prevent a carryover bias. The study was completed when AOC with each device had been applied for 24 hours, with standard respiratory management thereafter resuming. The SpO2 TR for both study periods was 91%–95%.
No other extra interventions were given. Infants did receive all standard treatments, and ventilation settings were at the discretion of the caregiver.
Data collection and analysis
Baseline characteristics were noted for each infant, including details on respiratory support and clinical state. The primary outcome was the proportion of time spent within the SpO2 TR (91%–95% with supplemental oxygen or 91%–100% without supplemental oxygen). SpO2 and intended FiO2 values were recorded each second from the data port or display of the ventilator under investigation. Secondary outcomes included: proportion of time in various degrees of hypoxaemia (SpO2 <80%, SpO2 80%–84%, SpO2 85%–90%, SpO2 ≤90%) and hyperoxaemia (SpO2 >95%, SpO2 96%–98% and SpO2 >98% while receiving supplemental oxygen); SpO2 and FiO2 coefficient of variation; frequency of 30 and 60 s episodes in hypoxaemia and hyperoxaemia; bradycardic episodes (heart rate <100 beats per minute for ≥10 consecutive seconds); frequency of FiO2 adjustments, both manual and automatic and average oxygen exposure.
Continuous data are represented as median (IQR) or mean±SD as appropriate, with standard tests for normality. Time within particular SpO2 ranges was collated for each infant individually and expressed as proportion of usable recorded time. Differences in time in TR and other outcomes were assessed with the Wilcoxon matched-pairs test. The intention-to-treat principle was applied. Statistical analyses were performed by an analysist blinded to allocation using R V.3.4.4 (R Core Team (2016). R: A language and environment for statistical computing, R Foundation for Statistical Computing, Vienna, Austria, URL: https://www.R-project.org/).
Sample size calculation was based around data from previous studies of the two automated control algorithms. In a study using the CLiO2 in Leiden in preterm infants the proportion of time in the SpO2 TR was 60.4% (±15.6%).24 In the first clinical study of the OxyGenie algorithm TR time was 78% (±15%). We considered a difference of 5% TR time a clinically relevant difference. For a two-sided paired statistical test, 44 infants would be needed assuming a SD of 10% for a power of 90% and an alpha of 0.05. Because a non-parametric test would be used in the analysis, we made a 15% addition to the sample size, as described by Lehmann,27 requiring a total of 50 participants.
Early termination
Just prior to study commencement, the SLE6000 ventilator was deployed as the standard device for neonatal respiratory support at LUMC. The AVEA ventilators were thereafter only used when an infant was included in the study. Based on historical data, we anticipated to complete recruitment in a year, which was also considered the maximum time competence of medical staff in working with both ventilators could be guaranteed. However, the recruitment rate was slower than expected and to ensure patient safety and an unbiased comparison of both oxygen control with the two ventilators the trial was terminated after a 12-month recruiting period.
Results
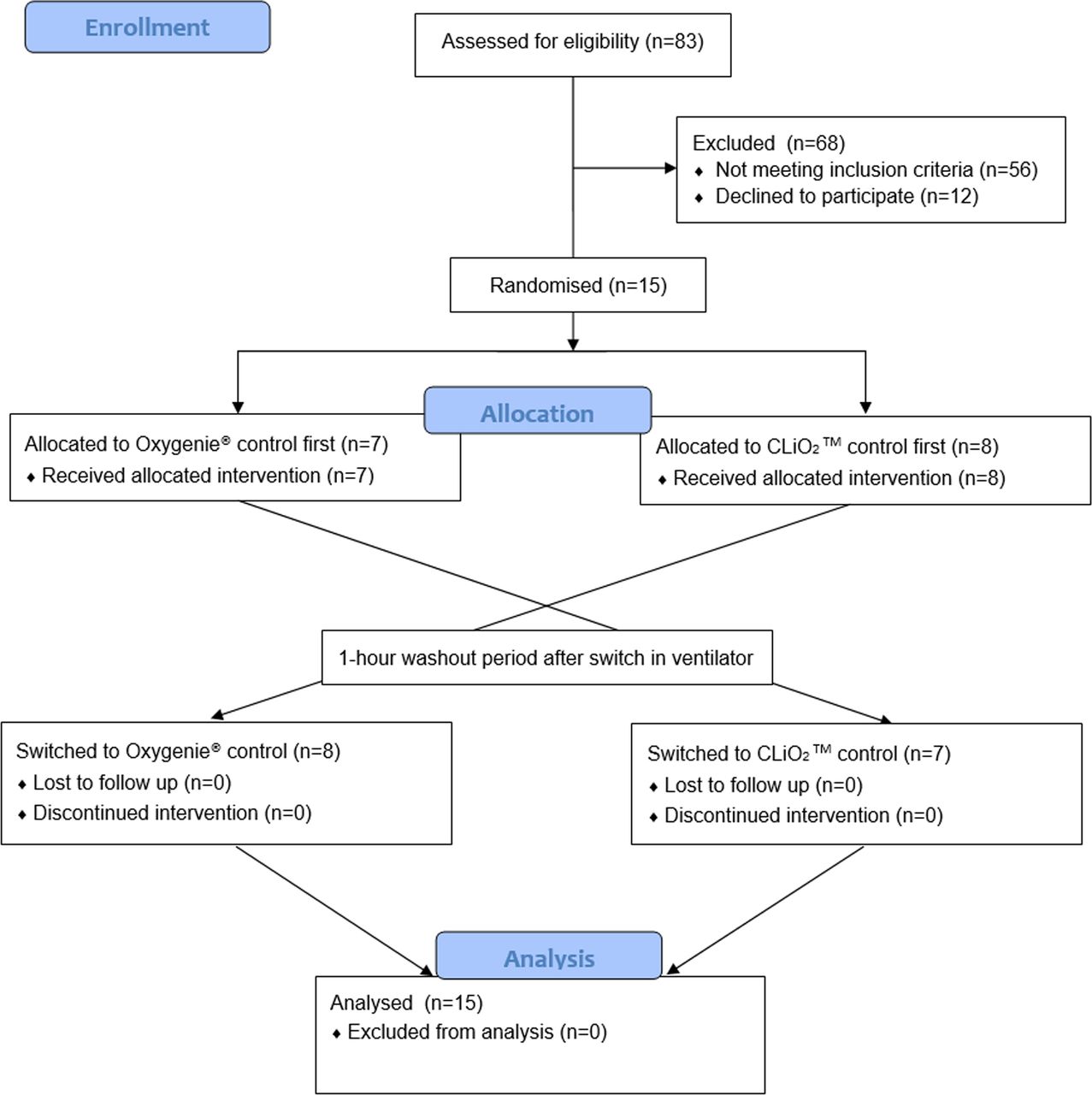
The study ran from February 2019 to February 2020, during which consent was sought from 27 parent couples of which 15 agreed to participate (figure 1). All participating infants (n=15, baseline characteristics table 1) completed the crossover comparison. In one infant, the second study period (OxyGenie control) was halted after 18 hours to allow treating clinicians to switch from continuous positive airway pressure to nasal high flow in response to nasal pressure areas. All study periods were included in the analysis. The total duration of recordings was 23 hours and 19 min (22:52–23:30) during OxyGenie control and 23 hours and 51 min (23:49–23:56) with the CLiO2 controller. A total of 2.9% (2.1%–5.0%) and 0.3% (0.2%–0.6%) of the time the SpO2 signal was missing, respectively.

CONSORT flow diagram.
Baseline characteristics
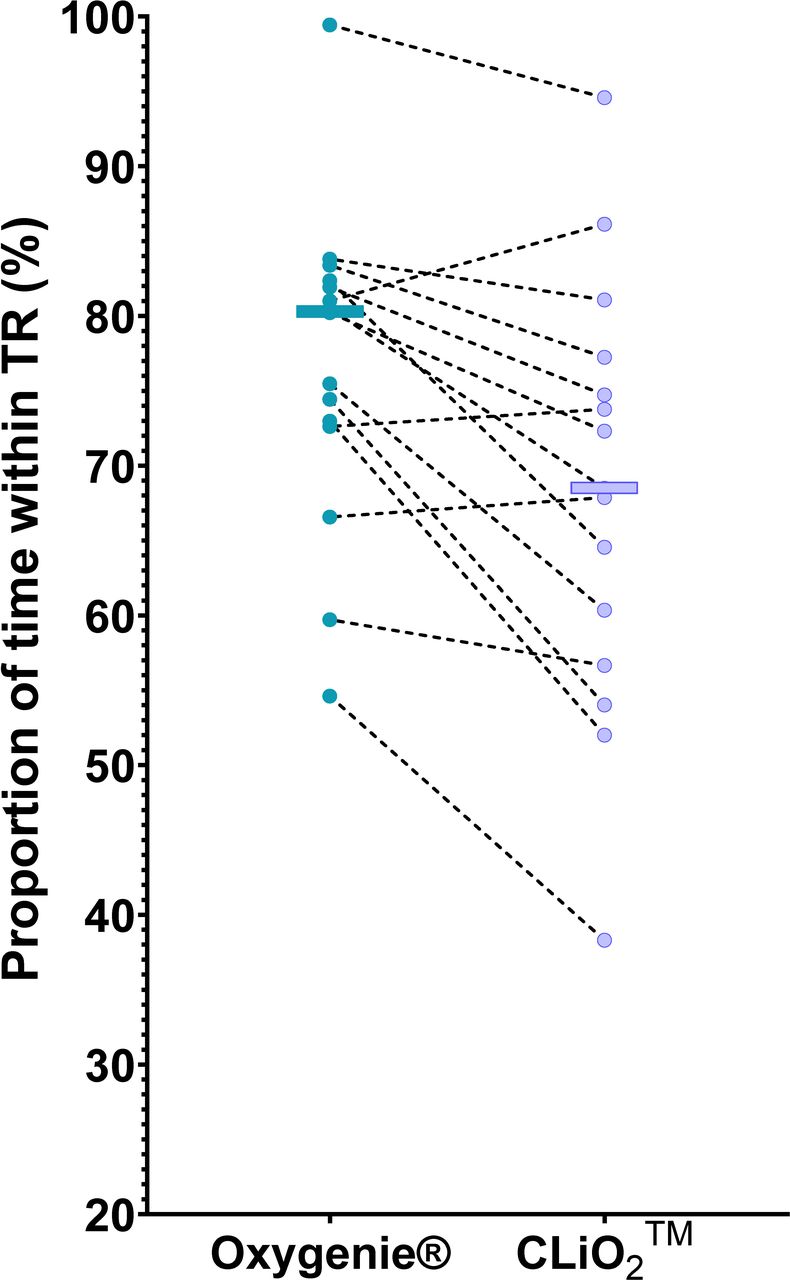
Histograms of pooled SpO2 data from the two automated control periods are shown in figure 2, demonstrating a narrower SpO2 distribution and a lower median SpO2 during OxyGenie control resulting in a higher proportion of time within the SpO2 TR. On per patient analysis, for the study primary outcome, there was a 11.7% increase in time within the SpO2 TR during oxygen control with the OxyGenie algorithm when compared with the CLiO2 device (table 2). Twelve infants spent more time in TR with OxyGenie control and three with CLiO2 control (figure 3). During the OxyGenie period, less time was spent above the TR while in supplemental oxygen, but more time spent below TR. SpO2 values <80% were very infrequent throughout the study, and the time with SpO2 <80% did not differ between control devices. The coefficient of variation for SpO2 was similar for both devices (3.3% (2.6%–4.0%) vs 3.2% (3.0%–3.4%), p=0.82).
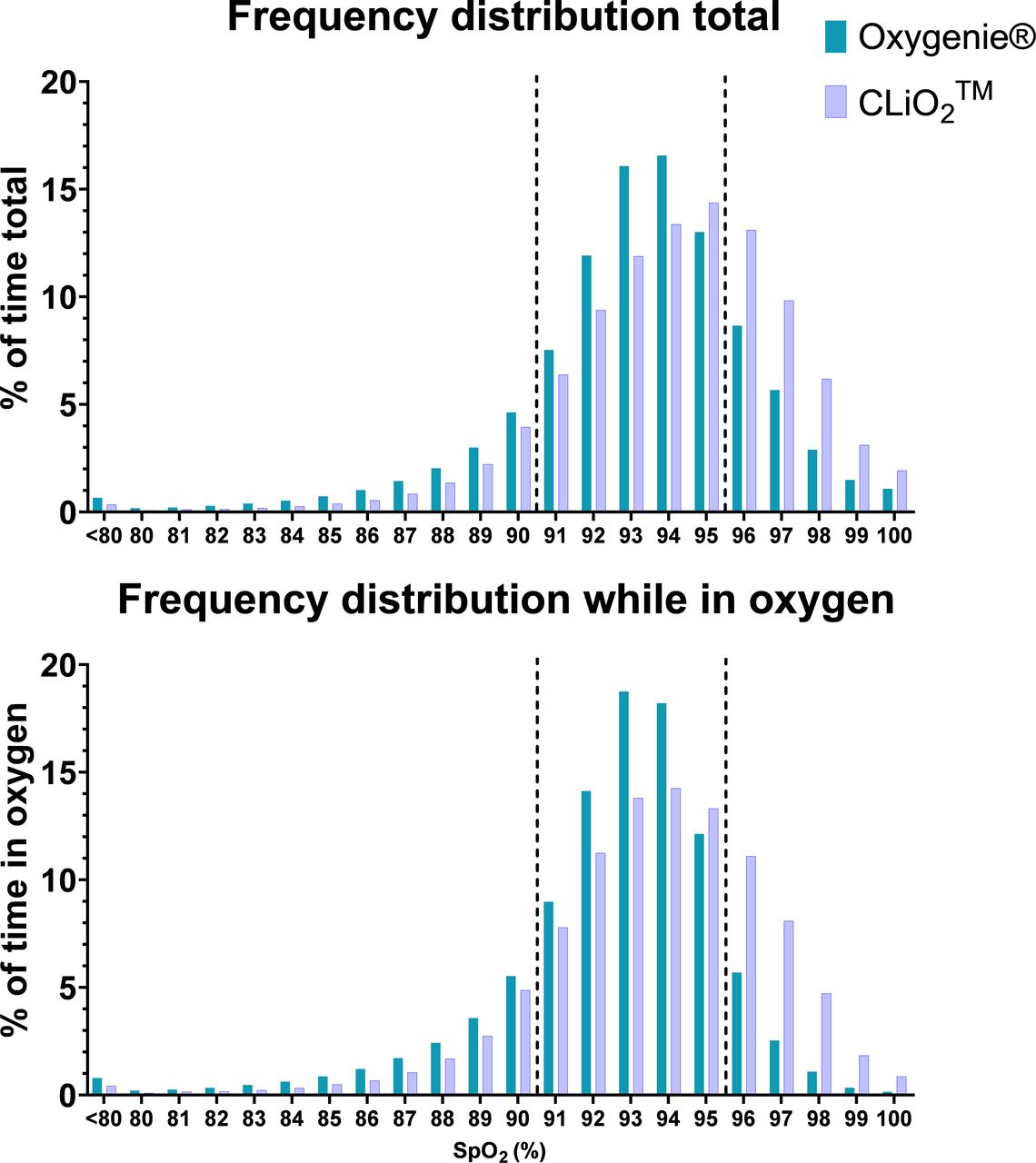
SpO2 histograms. Pooled time spent per SpO2 value as proportion of total usable time, while receiving supplemental oxygen and ambient air (total) or while only receiving supplemental oxygen. Dashed lines represent the limits of the SpO2 target range.
{kind=link}
{kind=link}
{kind=link}
Comparison of OxyGenie control with CLiO2 control. Individual paired values of proportion of time within TR while on OxyGenie control and while on CLiO2 control. Horizontal bar=median. Within TR=91%–95% with supplemental oxygen or 91%–100% without supplemental oxygen. TR, target range.
Proportions of time within SpO2 ranges
There was a decrease in frequency of both hypoxaemic and hyperoxaemic episodes during OxyGenie control (table 3). Bradycardic episodes (<100 bpm for ≥10 s) were rare in both epochs and were not different (0.3 (0.1–0.6) vs 0.2 (0.0–0.5) per hour, p=0.22).
Hypoxaemic and hyperoxaemic episodes
OxyGenie adjusted FiO2 about 10 times more frequently than the CLiO2 device (1155 (1044–1255) vs 194 (178–205) adjustments/hour, p=0.001). The average delivered FiO2 was similar during both study periods (0.27+−0.05 vs 0.26 +−0.08, p=0.56). FiO2 was more variable when titrated by the OxyGenie algorithm (coefficient of variation 19.5% (15.2%–25.0%) vs 13.3% (12.8%–19.0%), p=0.015). During OxyGenie control, manual overrides of the AOC were made only in one individual subject (four adjustments) versus nine individuals (16 adjustments) with manual overrides during the period of CLiO2 oxygen control.
Discussion
In this randomised controlled crossover study, automated titration of inspired oxygen concentration using the OxyGenie controller significantly increased the time spent within the SpO2 TR when compared with the CLiO2 controller. The difference in controller function was reflected in the SpO2 histogram, with a more balanced distribution of SpO2 values within and around the TR during OxyGenie control. This resulted in significantly less time spent above the TR, and fewer hyperoxaemic episodes, although at the cost of a small increase in time spent with SpO2 values below TR. The greater time with SpO2 in the range 80%–90% with OxyGenie compared with CLiO2 control was not accompanied by an increase in the frequency of hypoxic episodes, which were, indeed, significantly fewer during OxyGenie control. These results suggest that algorithm design, and in particular algorithm responsiveness, plays an important role in how successful SpO2 targeting will be with a given oxygen control device.
This is the first study to compare two different ventilators incorporating AOC algorithms head-to-head. Although earlier studies have individually compared the algorithms in question to manual oxygen titration,15–20 23 24 heterogeneity between the studies has precluded drawing inferences about their function relative to each other. Our findings in relation to proportion of time within TR were similar to previous studies, implying that the SpO2 targeting results achieved by controllers in our study were representative of their overall performance. Compared with the TR time of 80% in this study, other studies of OxyGenie control have demonstrated TR times of 81%23 and 88%.28 For CLiO2 (69% TR time in this study), other studies have shown TR time of 40%,15 58%,16 62%,18 76%,19 73%20 and 62%24).
The study was terminated before reaching the predetermined sample size of 50 infants. The deployment of the SLE6000 ventilator at LUMC had an impact on numbers of eligible infants by virtue of (1) the option of nasal high flow (not available with the AVEA ventilator) being taken up at an early juncture in many preterm infants, precluding involvement in the study and (2) fewer infants spending >18 of the preceding 24 hours with an FiO2 ≥0.25, in part attributable to the progressive approach to weaning FiO2 inherent in OxyGenie control. As a result, the recruitment rate was lower than expected. To prevent a loss of competence in handling the AVEA ventilator, potentially introducing a bias into the study, we decided to terminate the study prematurely. Truncated clinical studies can lead to overexaggerated observed effects.29 30 For our study, this would mean that the observed benefit for the OxyGenie controller in comparison to CLiO2 controller may overestimate the true benefit. However, if we had planned for an interim analysis to decide for stopping the trial after 15 patients, we would have surpassed both the Pocock and O'Brien-Fleming boundary criteria for clearly showing evidence of benefit for the OxyGenie controller. For a single interim analysis, Pocock recommends a p-threshold of 0.029431 and O'Brien-Fleming recommends a more conservative 0.0054 p-threshold32 to control for type I error due to repeated testing. The apparent benefit of OxyGenie is also demonstrated by a 11.7% improvement which is more than twice the clinically relevant difference of 5% for which the current study was powered.
There was an imbalance between the two oxygen control devices in the proportion of missing values. Both algorithms use a built-in Masimo pulse oximeter with similar algorithms making it unlikely that the actual reliability of pulse oximeter measurement was different between ventilators. But, to ensure a prompt response to TR deviations, OxyGenie uses a 2–4 s averaging time whereas CLiO2 uses an 8 s averaging time. This could lead to more missing signal, as shorter averaging times are inherently more susceptible to disturbances. Furthermore, although the same SET technology is used, manufacturers are free to choose the signal quality threshold below which SpO2 is reported as missing. It seems likely that the handling of the SpO2 signal within the SLE6000 is more conservative in this respect. Because the proportion of missing signal was still relatively low in both oxygen control periods, its effect on the outcomes of this study is likely to have been modest.
This study compared two ventilators rather than purely the AOC algorithms. It is possible that ventilator mechanics also played a role in the effectiveness of oxygen control as well as other aspects of ventilator function including the circuit flow characteristics.33 However, this was a pragmatic choice as license agreements precluded us from implementing two algorithms in one ventilator.
Contrary to our hypothesis, the benefit of an increase in SpO2 TR time with OxyGenie control was gained with a lesser occurrence of hyperoxaemia, at the cost of a minor increase in time spent with SpO2 80%–90%. Although at first glance it appears there is a trade-off between hyperoxaemia and hypoxaemia, the reduction in hypoxaemic episodes with OxyGenie control suggests that hypoxaemia is resolved more quickly. This is in line with the clinical observation of caregivers, who reported that OxyGenie responded more rapidly to SpO2 deviations into hypoxaemia than CLiO2. Compared with other studies, time with SpO2 <80% was modest with both controllers. For the OxyGenie controller, it was 0.5% in our study vs 0%23 previously; for the CLiO2 controller, it was 0.2% whereas other studies reported 9.8%,15 1.2% and 0.8%,18 3.1%,19 1.3%20 and 0.9%.24
The increase in time spent under TR could be due to a lower median SpO2 during OxyGenie control (93% vs 94%) on the steeper part of the oxygen-dissociation curve. The higher median SpO2 during CLiO2 control could be because, according to the patent, an SpO2 of 94% is targeted while in TR and the FiO2 is rarely titrated below the BaseFiO2 .26
Even though the benefit of AOC on SpO2 TR time is well-established, the effect on clinical outcome is still unknown. The effect of SpO2 targeting within different ranges on clinical outcome was demonstrated by the NeOPRoM trials,4 and a range of studies have evidenced the harmful effects of hypoxaemia and hyperoxaemia (and episodes thereof),34–39 both of which are affected by AOC. We would maintain that when searching for clinical effect of AOC, it is important to use an algorithm that most successfully avoids and mitigates SpO2 deviations, because the effect on clinical outcomes may be modest and in some cases may be difficult to detect given their relatively low incidence.
Finally, low compliance in TR adherence such as reported in the NeOPRoM trials4 could be improved on by using AOC. For the best differentiation between treatment groups, it is important to have a controller that best targets the predefined ranges.
Conclusion
In this study, the OxyGenie controller was more effective in keeping the oxygen saturation within TR and preventing hyperoxaemia, and just as effective in preventing hypoxaemia (SpO2 <80%), although at the cost of a small increase with SpO2 80%–90%.
Data availability statement
Data are available on reasonable request.
Ethics statements
References
Footnotes
Twitter @None
Contributors HHS: co-conceived the study (with ABtP) conducted the study, compiled, analysed and interpreted the data (with SCP), co-wrote the first draft of the manuscript and approved the final version of the manuscript. SJEC: reviewed and edited the manuscript, conducted the study and approved the final version of the manuscript. RSGMW: reviewed and edited the manuscript, acquired data and approved the final version of the manuscript. TJG: reviewed and edited the manuscript, interpreted the data and approved the final version of the manuscript. PAD: interpreted the data, reviewed and edited the manuscript and approved the final version of the manuscript. SCP: reviewed and edited the manuscript, performed the analysis and interpretation of the data and approved the final version of the manuscript. ABtP: co-conceived the study, oversaw the study conduct, interpreted the data, cowrote the first draft of the manuscript and approved the final version.
Funding This work was supported by SLE Limited by an unrestricted research grant.
Disclaimer SLE Limited had no role in study design nor in the collection, analysis and interpretation of data, writing of the report and decision to submit the paper for publication.
Competing interests ABtP has received an unrestricted research grant from SLE Limited; they had no role in study design nor in the collection, analysis, and interpretation of data, writing of the report and decision to submit the paper for publication. The University of Tasmania and Royal Hobart Hospital have a patent concerning automated control of inspired oxygen concentration in the new-born infant and have a licensing agreement with SLE Limited in relation to OxyGenie automated oxygen control software.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms