Article Text

Abstract
Objective Establish if serial, multichannel video electroencephalography (EEG) in preterm infants can accurately predict 2-year neurodevelopmental outcome.
Design and patients EEGs were recorded at three time points over the neonatal course for infants <32 weeks’ gestational age (GA). Monitoring commenced soon after birth and continued over the first 3 days. EEGs were repeated at approximately 32 and 35 weeks’ postmenstrual age (PMA). EEG scores were based on an age-specific grading scheme. Clinical score of neonatal morbidity risk and cranial ultrasound imaging were completed.
Setting Neonatal intensive care unit at Cork University Maternity Hospital, Ireland.
Main outcome measures Bayley Scales of Infant Development III at 2 years’ corrected age.
Results Sixty-seven infants were prospectively enrolled in the study and 57 had follow-up available (median GA 28.9 weeks (IQR 26.5–30.4)). Forty had normal outcome, 17 had abnormal outcome/died. All EEG time points were individually predictive of abnormal outcome; however, the 35-week EEG performed best. The area under the receiver operating characteristic curve (AUC) for this time point was 0.91 (95% CI 0.83 to 1), p<0.001. Comparatively, the clinical course AUC was 0.68 (95% CI 0.54 to 0.80, p=0.015), while abnormal cranial ultrasound was 0.58 (95% CI 0.41 to 0.75, p=0.342).
Conclusion Multichannel EEG is a strong predictor of 2-year outcome in preterm infants particularly when recorded around 35 weeks’ PMA. Infants at high risk of brain injury may benefit from early postnatal EEG recording which, if normal, is reassuring. Postnatal clinical complications can contribute to poor outcome; therefore, we state that a later EEG around 35 weeks has a role to play in prognostication.
- neonatology
- neurology
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Although survival rates are improving, very preterm infants continue to be at high risk of neurodevelopmental delay.
The clinical condition of preterm infants can be monitored in the neonatal intensive care unit but providing parents with an accurate prediction of outcome is challenging.
Electroencephalography (EEG) has the potential to support more accurate prediction of long-term neurodevelopmental outcome in very preterm infants.
What this study adds?
EEG recorded around 35 weeks of age in preterm infants has the highest predictive ability for outcome, outperforming the predictive ability of EEGs recorded earlier.
EEG is a useful adjunct to provide information about early brain development .
Introduction
Although the survival rate for preterm infants has improved in recent decades, they still continue to be at high risk of neurodevelopmental delay.1 Specifically, infants <32 weeks’ gestational age (GA) are at an increased risk of cerebral palsy (CP) and other problems compared with more mature infants.2 3 Accurate recognition of infants at increased risk of abnormal neurodevelopment is challenging during the neonatal period. By providing additional physiological information, like cerebral function, infants may benefit from early intervention, influencing positive outcomes.4 The infant’s condition and development in the neonatal intensive care unit (NICU) can be monitored but providing parents with an accurate prediction of outcome is challenging.
Continuous electroencephalography (EEG) is used to evaluate brain function. The EEG of preterm infants varies, depending on GA. As infants mature, specific waves appear/disappear, change in morphology, characteristics and organisation. The evolving EEG reflects how the brain of a premature infant rapidly develops, making it very difficult to objectively evaluate brain activity and maturation.5 Previous studies have shown that early grading of the EEG6–9 and amplitude-integrated EEG (aEEG) can predict long-term neurodevelopmental outcome.10–16 To the best of our knowledge, this is the first study to record serial multichannel video EEG and use a recently published tailored and standardised preterm EEG assessment scheme.5 This study aims to establish whether serial multichannel video EEG in the preterm infant (<32 weeks’ GA), beginning on the first postnatal day, has a role in the prediction of outcome at 2 years of age.
Methods
Participants
This was a prospective, observational study performed between March 2013 and April 2014 in the NICU of Cork University Maternity Hospital. All infants born at <32 weeks’ GA were eligible for enrolment and were included if they had early continuous multichannel EEG monitoring. Enrolment was not determined by or related to the clinical condition of the infant. All infants were recruited prospectively. Infants with known congenital anomalies were excluded. Cranial ultrasound (CRUS) scan reports were reviewed for cerebral abnormalities such as intraventricular haemorrhage (IVH) or periventricular leukomalacia (PVL).
EEG recording
Three EEG machines were used: the NicoletOne EEG system (CareFusion, San Diego, USA); the Nihon Kohden, EEG-1200, Neurofax (Tokyo, Japan); and the Moberg ICU Solutions, CNS-200 EEG and Multimodal Monitor (Ambler, Pennsylvania). Disposable Ambu Neuroline 700 single-patient surface electrodes were applied to the scalp using a modified neonatal version of the international 10/20 system.17
EEGs were recorded at three time points (EEG-1, EEG-32 and EEG-35) over the neonatal course. EEG-1 was a continuous, long-term recording acquired as soon as possible after birth and continued until approximately 72 hours of age. Two-hour epochs of EEG-1 were extracted at four different time points (12, 24, 48 and 72 hours of age) to capture postnatal changes.18 The whole recording was assessed for seizures and the background activity of the epochs was graded. EEG-1 grade was based on the most abnormal grade selected from the four epochs. EEG-32 and EEG-35 were shorter (2–4 hours) recordings at 32 and 35 weeks’ GA, respectively.
EEG grading
EEGs were scored based on a published standardised grading system which uses temporal organisation/cyclicity, normal features, abnormal waves and abnormal features for grading.5 This grading system comprises five EEG grades: grade 0 (normal); grade 1 (mild low voltage, slightly prolonged interburst intervals (IBI), positive temporal sharp wave, other sharp waves); grade 2 (moderately low voltage, moderately prolonged IBI, positive rolandic sharp waves, deformed mechanical brushes, deformed delta, asymmetry, abnormal asynchrony, brief intermittent rhythmic discharges, immature waves (26 weeks<), no cyclicity (<28 weeks)); grade 3 (severely low voltage, excessively prolonged IBI, seizures, burst suppression (28 weeks<)); and grade 4 (isoelectric and status epilepticus).
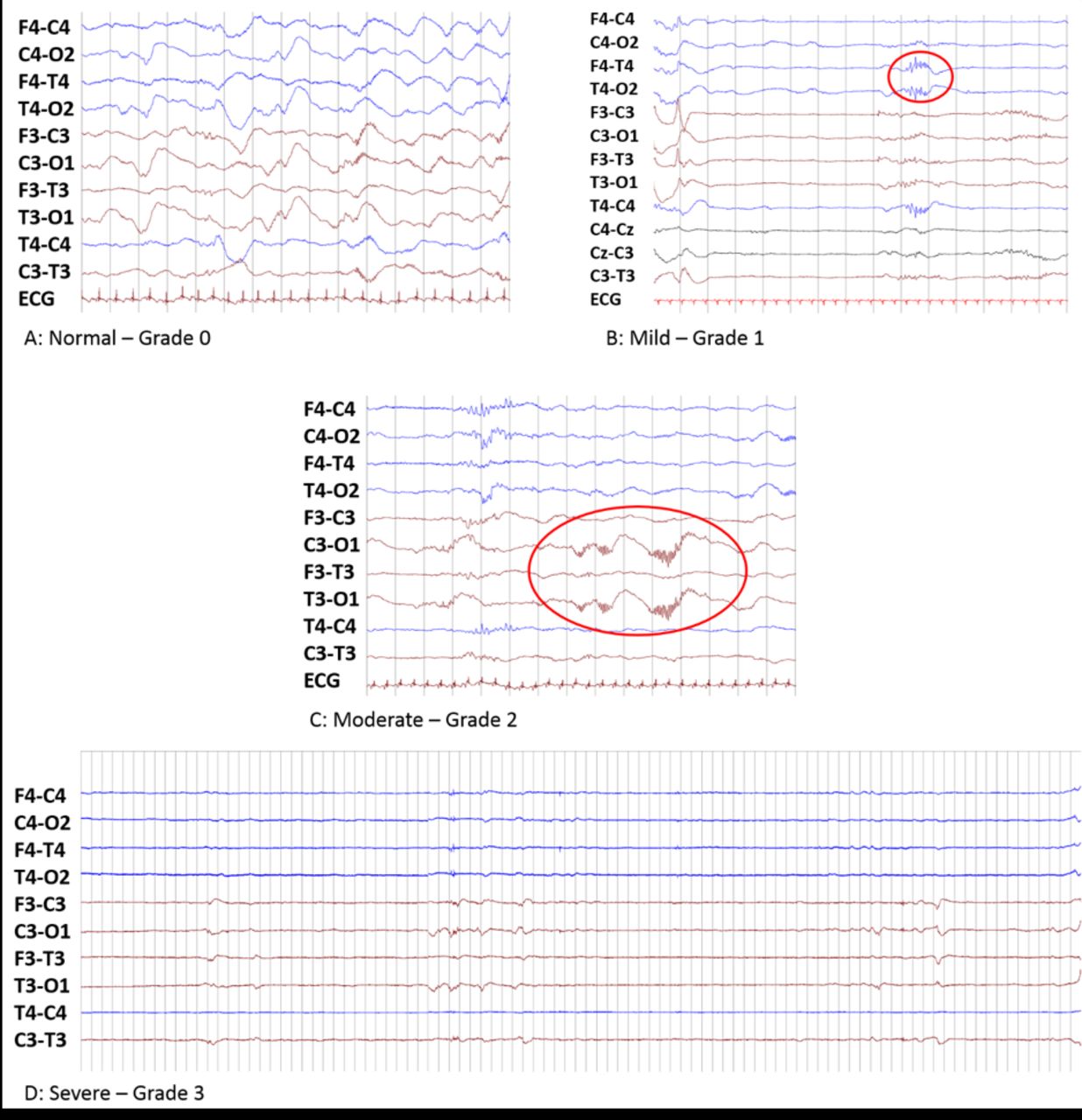
For prediction of neurodevelopmental outcome, EEG grades were dichotomised to ‘normal’ (grades 0–1) and ‘abnormal’ (grades 2–4).9 19 A neonatal electroencephalographer (rater 1) graded all EEG time points, blinded to all clinical information except for GA and administration of morphine/phenobarbitone. For validation, another neonatal electroencephalographer (rater 2) reviewed a random subset of 66 epochs from the recordings. Examples of EEG grades are seen in figure 1.
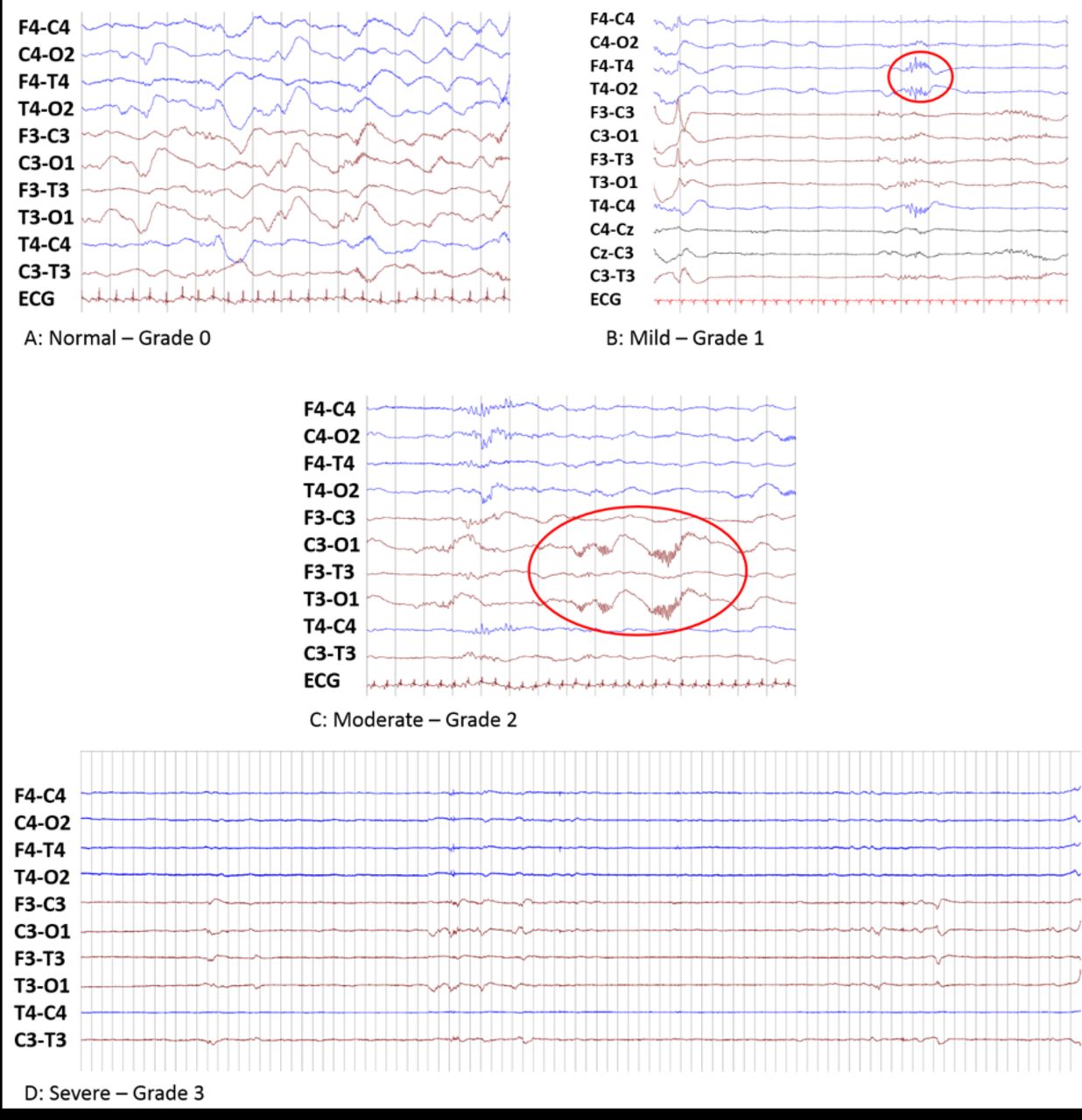
Examples of electroencephalography (EEG) from four different infants, presenting varying degrees of EEG abnormal severity. Infant A: female, 30+3 weeks’ gestational age (GA) at 12 hours of life, with continuous activity and no abnormal activity. Infant B: male, 30+2 weeks’ GA at 12 hours of life, positive temporal sharps (PTS). Infant C: male, 26+0 weeks’ GA at 12 hours of life, occipital deformed mechanical brush activity and asymmetry. Infant D: female, 26+4 weeks’ GA at 48 hours of life, excessive discontinuity period lasting 95 s.
Assessment of neonatal clinical course
As described in a previous report,19 five major clinical complications over the neonatal course (from admission to the NICU to discharge) were considered as high risk for later morbidity: grade 3/4 IVH/cystic PVL (cPVL), chronic lung disease, necrotising enterocolitis, sepsis and retinopathy of prematurity. Each infant was classified with either a ‘complicated clinical-course score’ based on the presence of at least one of these complications, or an ‘uncomplicated clinical-course score’ based on the absence of any of these complications.20–24
Two-year outcome assessment
The Bayley Scales of Infant Development III (Bayley-III) was used to assess neurodevelopmental outcome at 2 years’ corrected age. Abnormal outcome was defined as death, diagnosis of CP following assessment through interventional services, or if any of the three subscales (motor, cognitive and language) were below 1 SD from the mean; thus, for the standardised scores, a value of <85 in any of the three subscales was deemed abnormal.25
Statistical analysis
Cohen’s kappa coefficient quantified inter-rater agreement for EEG grading. Area under the receiver operating characteristic curve (AUC), sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and their corresponding 95% CIs quantified prediction of abnormal outcome for each EEG time point. These metrics were also used to test the association of clinical course and abnormal outcome. To test the independence of the EEG grades in predicting abnormal outcome potential confounders (birth weight, Apgar score, intrauterine growth restriction (IUGR) and IVH grade) were evaluated using univariable logistic regression analysis. Variables with p<0.1 in the univariable analysis were included in the multivariable logistic regression analysis giving adjusted ORs and 95% CIs for the association between EEG grade and outcome. Cochran’s Q-test was used to investigate if EEG abnormality changed over the three time points. In addition to using dichotomised outcome and EEG grades, we also used Spearman’s correlation coefficient (rs) to investigate relationships between actual scores on each subscale of the Bayley’s, and the five EEG grades.
Continuous variables were described using median and IQR and categorical variables were described using numbers and percentages. For comparisons between the outcome groups (normal and abnormal), the Mann-Whitney U test was used for continuous variables and Fisher’s exact test for categorical variables. Fisher’s exact test also assessed the associations between outcome and EEG grading at each of the time points. CIs for Spearman’s correlation coefficient were calculated using a bootstrap approach.
Statistical analyses were performed using MedCalc and IBM SPSS Statistics V.21 (SPSS). All tests were two sided and a p value <0.05 was considered statistically significant.
Results
During the study period, 103 infants <32 weeks’ GA were eligible and 70 were enrolled in the study. Thirty-three infants were not enrolled due to unavailability of EEG machines, declined consent or unavailability of research staff. Three infants with EEG recordings were excluded due to congenital anomaly and consent withdrawal. Sixty-seven infants were included in the final analysis and follow-up.
At 2 years’ corrected age, 10 infants were lost to follow-up: 1 was excluded due to a late diagnosis of Beckwith-Wiedemann syndrome, 1 declined to attend appointments and 8 did not respond. Outcome was therefore available in 57 of the 67 infants (85%). Four infants died prior to NICU discharge and two infants were diagnosed with CP. The outcome of the remaining 51 infants was based on their Bayley-III assessment. Forty (70%) infants had a normal neurodevelopmental outcome and 17 (30%) had an abnormal outcome. Clinical and demographic characteristics are detailed in table 1.
Clinical demographics and characteristics of all the infants by outcome
EEG recordings
Data were available for 57 infants at EEG-1, 53 infants at EEG-32 (4 infants had died) and 45 infants at EEG-35 (8 infants were transferred or discharged earlier). EEG-1 commenced at a median postnatal age of 7 hours 38 min (IQR: 4 hours 46 min to 11 hours 51 min). The median recording duration was 68 hours 24 min (IQR: 63 hours 57 min to 71 hours 13 min). The median recording duration of EEG-32 and EEG-35 was 2 hours 46 min (IQR: 2 hours 1 min to 4 hours 4 min) and 2 hours 11 min (IQR: 2 hours to 2 hours 59 min), respectively. Inter-rater agreement for EEG grading was high (Cohen’s kappa coefficient=0.91).
In total, 18 infants (32%) had a normal EEG-1 (grades 0 and 1) and 39 (68%) had an abnormal EEG-1 (grades 2 and 3). No EEG epoch was graded isoelectric or status epilepticus (grade 4).
EEG and outcome assessment
All three serial EEGs were individually predictive of 2-year outcome. In table 2, sensitivity calculates the ability of the EEG to correctly classify infants with an abnormal outcome, while specificity calculates the ability of the EEG to correctly classify the infants with a normal outcome. Dichotomised outcome was used as our main finding to allow the six infants who died or were diagnosed with CP to be included in the analysis.
Confusion matrix, sensitivity, specificity, positive and negative predictive value (PPV and NPV) of EEG at three different time points and the relationship with neurodevelopmental outcome in all available infants
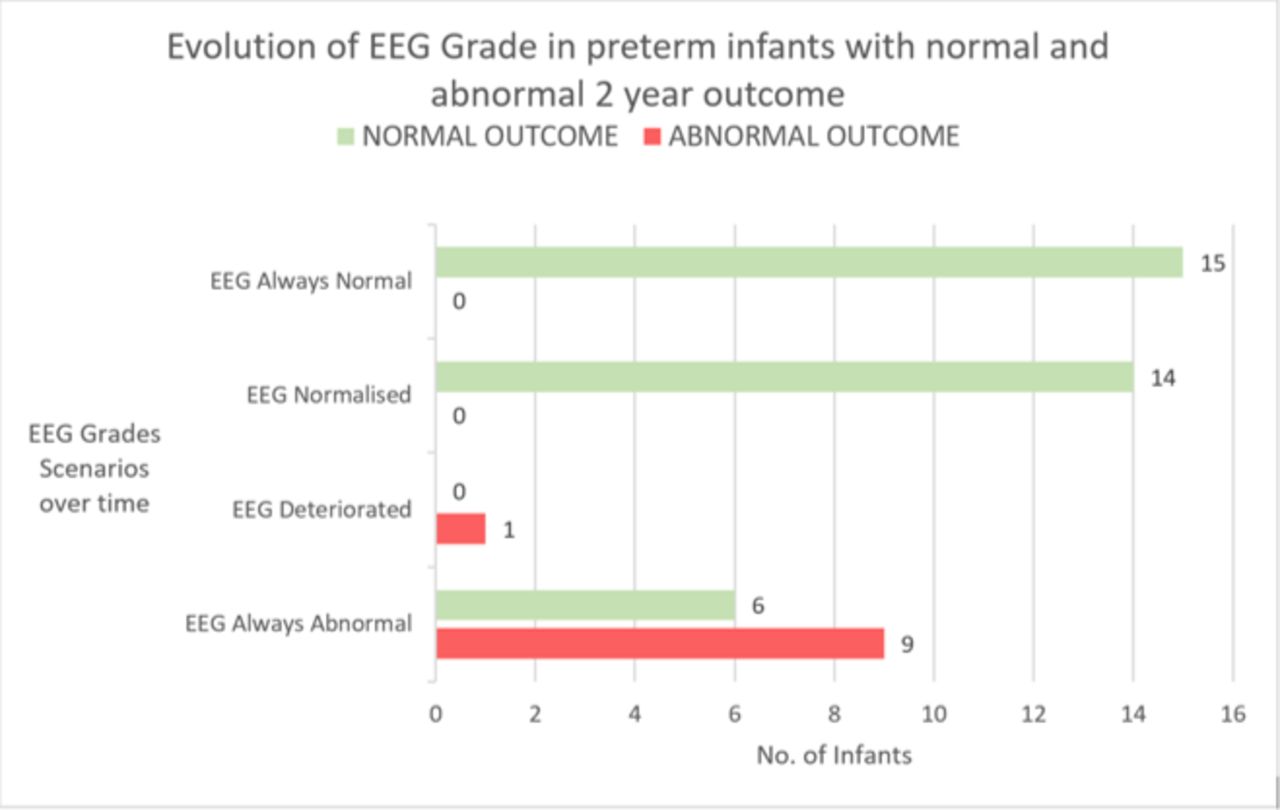
All infants whose EEG remained normal or was initially abnormal but normalised over the course of the three recordings had a normal 2-year outcome. One infant with abnormal outcome had a normal EEG-1, then became abnormal by EEG-32 following an episode of sepsis. When the EEG was initially abnormal and remained abnormal from EEG-1 to EEG-35, 60% had an abnormal outcome. Six infants had a normal 2-year outcome even though the EEGs were abnormal at all time points. All six infants had major complications within the first 72 hours. Figure 2 shows the trajectory of the grades at different time points, from all possible scenarios, for both outcomes.

{kind=link}
{kind=link}
Bar graph of the number of preterm infants with different electroencephalography (EEG) grade evolutions from EEG-1 to EEG-35 and their neurodevelopmental outcome (n=45). EEG always normal—when EEG-1, EEG-32 and EEG-35 were normal; EEG normalised—when EEG-1 was abnormal and EEG-35 was normal; EEG deteriorated—when EEG-1 was normal and EEG-35 was abnormal; EEG always abnormal—when EEG-1, EEG-32 and EEG-35 were abnormal.
EEG-1 remained statistically significant for the prediction of outcome when we controlled for potential confounders (birth weight, Apgar at 1 and 5 min, IVH and IUGR). Table 3 presents the unadjusted ORs for EEG-1 and adjusted OR controlling for these possible confounding variables. EEG-1 remained statistically significant in each multivariable logistic regression analysis (adjusted OR range: 9.14–13.96). None of the potential confounding variables were statistically significant in the multivariable model.
Results of multivariable logistic regression adjusting for possible confounding clinical variables testing the association with the EEG-1 recording, n=57
Furthermore, statistically significant, moderate to large, negative correlations were found between EEG grade (normal to severe) and each Bayley-III subscale on at least one time point, with strongest correlations found for the language subscale at all time points and cognitive subscale during EEG-32 and EEG-35 (online supplemental table).
Supplemental material
Clinical course and outcome assessment
Of the 45 infants who had all EEG recordings, 15 had an uncomplicated clinical course and 14 had normal outcome at 2 years. The infant with an uncomplicated clinical course but abnormal outcome had abnormal EEGs at all time points.
Of the 30 infants with clinical complications, nine had abnormal outcome. All nine infants had an abnormal EEG-35; however, another six infants with abnormal EEG-35 had a normal outcome. All 15 infants with a complicated clinical course and normal EEG-35 had a normal outcome. The clinical course was predictive of abnormal neurodevelopmental outcome, with an AUC of 0.65 (0.47–83), sensitivity of 90% (56%–100%) and specificity of 40% (24%–58%) reported. Additionally, infants with IVH grade 3/4 or cPVL following abnormal CRUS findings were also investigated, reporting an AUC of 0.58 (95% CI 0.41 to 0.75), p=0.342.
Discussion
We report the utility of serial, multichannel EEG in preterm infants for the prediction of neurodevelopmental outcome at 2 years of age. EEGs were recorded in preterm infants during the first 3 postnatal days and at approximately 32 and 35 weeks. All recordings at each time point proved useful; however, EEG-35 had the highest AUC of 0.91 (95% CI 0.83 to 1.00). At this time point, infants are less vulnerable to complications and more stable. Infants with normal or mildly abnormal EEG recordings at approximately 32 and 35 weeks’ GA had normal outcomes in every case. This finding suggests that an EEG between 32 and 35 weeks could offer valuable early prognostic information for healthcare teams and parents.
Both analysis methods, with dichotomised and continuous outcome and EEG grading, showed statistically significant results with the more abnormal EEG grading being predictive of more abnormal neurodevelopmental outcome: unadjusted OR 11.83 (95% CI 1.43 to 98.06) for the former and rs=−0.354 to −0.564 for the latter. Dichotomising neurodevelopmental outcome is a standard approach in many EEG studies.9 11 25 It allows us to form a composite score across the three Bayley subscales which may be of clinical benefit to quickly identify those infants at risk of delayed neurodevelopment who may need additional clinical follow-up assessments or early interventional strategies. For these reasons, we present results from the dichotomised outcome as our main finding.
The high predictive ability of the EEG could be a result of using our EEG grading system.5 It is a very detailed age-specific scheme which has numerous features incorporated. Visual EEG interpretation is challenging as features change with maturation,26 27 therefore using an age-specific preterm grading system can enhance a more standardised way of analysis. The strong inter-rater agreement results (Cohen’s kappa of 0.91) confirm this.
This study has shown different findings to our previous study in 2016,19 which used the Watanabe EEG grading system28 in a model with other physiological measurements, with a different cohort of infants (n=43). This 2016 study used early recordings only, that is, equivalent to the EEG-1 time period from this current study, which showed similar AUC (0.68); however, the sensitivity was higher in this study at 94% while the specificity was lower at 43%. This could be due to study differences, such as different infants in both cohorts, different EEG grading system used, different epochs used (with the current study also using 48 and 72-hour epochs) and different epoch duration (2-hour epochs for the current study; 1 hour for the 2016 study).
Previous studies have used serial EEG to predict outcome in very preterm infants,6 8 9 29 identifying later recordings as more useful. In these studies, adverse outcome was associated with severe EEG abnormalities, such as seizures, acute and chronic stage abnormalities or abnormal features. Sensitivity and specificity to predict outcome ranged from 16%–83% and 88%–96%, respectively,6 8 9 in comparison to our results of 100% and 83%. Our results are not completely comparable, however, due to numerous methodological differences, such as different EEG grading scheme, different serial recording duration, timing and age.6 8 9 Many studies have examined the use of quantitative preterm EEG analysis but results are inconclusive.25 30 Studies have also reported an association between aEEG/limited EEG and abnormal outcome, with sensitivity and specificity values ranging from 73%–93% and 41%–97%, respectively.10 11 15 Particular features such as early depression, absent cyclicity, seizures, prolonged IBI, burst suppression and specific characteristics of burst activity were predictive of an abnormal outcome.11–14 31
Even though EEG-1 provided the lowest specificity, PPV and the lowest AUC, the number of infants with an abnormal outcome was significantly higher in the group with an abnormal EEG-1 compared with the group with a normal EEG-1. This difference remained after adjusting for the potential confounding effects of weight, Apgar score, IUGR and IVH grade. We have found that a normal EEG at 32 and 35 weeks predicted normal outcome at 2 years in our group of infants. At 35 weeks, both sensitivity and specificity were highest (100% and 83%, respectively), with PPV and NPV of 63% and 100%, respectively. These PPV results were higher (63%) than a study investigating moderate/severe MRI white matter abnormalities at term equivalent age, with PPV results of 21%32 . The suitability of predischarge CRUS and MRI recordings has previously been discussed33; however, this study offers a potential role for EEG at predischarge (approximately 35 weeks). Additionally, the EEG-1 recording was a better predictor of abnormal outcome than CRUS, with an AUC of 0.68 (0.55–0.80, p=0.011) and 0.58 (0.41–0.75, p=0.342), respectively, suggesting that early EEG assessment of background activity has a role to play in the early postnatal period.14 34 Background EEG activity evolves gradually with maturity in preterm infants, therefore serial recordings can identify deteriorating or improving brain function following a resolving acute injury.8 We report that all infants with normal 35-week EEG regardless of prior EEG findings had a normal 2-year outcome. Furthermore, as standard, the clinician would be aware of a complicated clinical course in infants. Adding 35-week EEG to the clinical course score could compliment current clinical practice.
The Bayley-III score allowed for standardised assessment of all surviving infants but there are some well-documented limitations.35 36 We used a cut-off score of 85 to ensure that infants with borderline abnormal results were identified and entered into a longer term 5-year follow-up programme. It is possible the Bayley-III assessment at 2 years might have underestimated possible developmental issues35 and that later testing at school age may reveal other problems.
Although the sample size was small, we have shown statistically significant results for the prediction of neurodevelopmental outcome using EEG grading when potential confounders were controlled for. Although objective, the EEG grading system is still dependent on interpretation by specially trained reviewers. This is a commonly recognised limitation in EEG studies; however, this particular assessment scheme is markedly different from previous grading systems due to the detailed definitions in the user instructions manual, which considerably reduces reviewers’ subjectivity (Cohen’s kappa coefficient=0.91).5 We do appreciate, however, that subtle differences in definitions can always lead to inter-rater variability. Future studies could make the grading scheme more accessible for non-experts, or explore an automated system similar to those available for the term EEG.37 38 Alternatively, exploring other physiological signals, such as heart rate and SpO2, along with serial EEG monitoring in the NICU may provide further improvements for the prediction of outcome.19 A future multicentre study, following the same protocols, would be advantageous to verify our findings.
A large amount of EEG data was collected during the lengthy NICU stay of very preterm infants. Experienced neonatal electroencephalographers reviewed the recordings anonymously, blinded to clinical information and were not involved in the clinical care of the baby. We analysed multichannel EEG rather than the aEEG because of the more detailed temporal and spatial information.39 In addition, the grading system used has previously been tested for inter-rater reliability between two specialists in the field of neonatal EEG.5 The effect of medication was considered during interpretation of the EEG, as drugs such as antiepileptic drugs and morphine can suppress the EEG and increase discontinuity. It was also essential to integrate EEG data with clinical information to aid investigation and prediction of adverse neurodevelopmental outcome in a clinical setting.40
In conclusion, we report that multichannel EEG in preterm infants can be a useful tool for predicting neurodevelopmental outcome at 2 years of age. The 35-week EEG proved to be the most accurate. A normal EEG at 32 and 35 weeks was an excellent indicator of normal neurodevelopmental outcome at 2 years, while an abnormal EEG highlights the potential for an abnormal outcome. Early EEG monitoring in the first 72 hours can also provide a useful baseline for early brain development. Comparing EEG and CRUS results showed that an EEG during any of the three postnatal periods was more predictive of outcome than CRUS. EEG should be considered as a useful adjunct to provide an indication of early brain development or to identify infants in need of further investigations such as MRI, ahead of discharge from the NICU.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Ethics approval
Ethical approval was granted by the Clinical Research Ethics Committee of the Cork Teaching Hospitals, Ireland. Written informed parental consent was obtained.
Acknowledgments
We are extremely grateful for the help provided by our research support team at the INFANT Research Centre during this study. We thank all the staff at the NICU at Cork University Maternity Hospital and the families of all neonates included in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors RL had the primary responsibility for protocol development, literature search, study design, collecting of EEG data and writing the manuscript. JMO and PF participated in the development of the protocol and study design and contributed to the writing of the manuscript. VL participated in the statistical analysis and contributed to the writing of the manuscript. GBB helped develop he protocol and analyse the EEG data, supervised the design and execution of the study and contributed to the writing of the manuscript.
Funding This research was funded by a Science Foundation Ireland Research Centre Award (12/RC/2272). JMOT was supported by a research grant from Science Foundation Ireland (15/SIRG/3580).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.