Article Text

Abstract
Objective Hypoxic-ischaemic encephalopathy (HIE) remains a leading cause of neonatal mortality and neurodisability. We aimed to determine the incidence of HIE and management patterns against national guidelines.
Design Retrospective cohort study using the National Neonatal Research Database.
Setting Neonatal units in England and Wales.
Patients Infants 34–42 weeks gestational age (GA) with a recorded diagnosis of HIE.
Main outcomes Incidence of HIE, mortality and treatment with therapeutic hypothermia (TH) were the main outcomes. Temporal changes were compared across two epochs (2011–2013 and 2014–2016).
Results Among 407 462 infants admitted for neonatal care, 12 195 were diagnosed with HIE. 8166 infants ≥36 weeks GA had moderate/severe HIE, 62.1% (n=5069) underwent TH and mortality was 9.3% (n=762). Of infants with mild HIE (n=3394), 30.3% (n=1027) underwent TH and 6 died. In late preterm infants (34–35 weeks GA) with HIE (n=635, 5.2%), 33.1% (n=210) received TH and 13.1% (n=83) died. Between epochs (2011–2013 vs 2014–2016), mortality decreased for infants ≥36 weeks GA with moderate/severe HIE (17.5% vs 12.3%; OR 0.69, 95% CI 0.59 to 0.81, p<0.001). Treatment with TH increased significantly between epochs in infants with mild HIE (24.9% vs 35.8%, p<0.001) and those born late preterm (34.3% vs 46.6%, p=0.002).
Conclusions Mortality of infants ≥36 weeks GA with moderate/severe HIE has reduced over time, although many infants diagnosed with moderate/severe HIE do not undergo TH. Increasingly, mild HIE and late preterm infants with HIE are undergoing TH, where the evidence base is lacking, highlighting the need for prospective studies to evaluate safety and efficacy in these populations.
- neonatology
- epidemiology
- neurology
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data were extracted and supplied by the NDAU and are available from the corresponding author on reasonable request and with permission of the study team and NDAU.
Statistics from Altmetric.com
What is already known on this topic?
Therapeutic hypothermia is an effective and safe treatment for infants ≥36 weeks gestational age with moderate/severe hypoxic-ischaemic encephalopathy (HIE), improving survival and reducing severe neurodisability.
There is insufficient evidence to support the use of therapeutic hypothermia for mild HIE or in late preterm infants with HIE.
What this study adds?
Use of therapeutic hypothermia for moderate or severe HIE has increased over time and is associated with a reduction in mortality.
A large cohort of infants recorded as having moderate/severe HIE do not receive treatment with therapeutic hypothermia.
Use of therapeutic hypothermia for mild HIE and in late preterm infants with HIE is increasing despite a lack of efficacy or safety.
Introduction
Hypoxic-ischaemic encephalopathy (HIE) is the leading cause of mortality and neurodisability in near-term and term babies.1 2 Therapeutic hypothermia (TH) is an effective, safe treatment for infants ≥36 weeks gestational age (GA) with moderate/severe HIE, improving survival and major neurodisability.1 3 Following the Total Body Hypothermia (TOBY) cooling trial4 and the National Institute for Health and Care Excellence guidance in 2010,5 TH is now the standard of care for infants ≥36 weeks GA with moderate/severe HIE in England and Wales. However, recent data on the current management and outcomes of infants with HIE in the TH era are lacking. The ambitious UK government target of halving brain injury occurring at or soon after birth by 2025 requires an understanding of the current incidence and management of HIE, allowing healthcare providers to target areas most likely to achieve these goals.6
There are increasing concerns that infants with mild HIE or those more preterm are also undergoing TH without evidence of benefit.7–11 A recent UK survey highlighted 75% of cooling centres offered TH to infants with mild HIE.9 Although infants with mild HIE have an increased risk of mortality and adverse neurological outcomes, there is insufficient evidence to establish any significant benefits or harm with the use of TH in these infants.7 8 For the preterm population, Azzopardi et al 12 reported 3% (n=38) of UK TOBY cooling registrants were 34 or 35 weeks GA with a higher mortality rate (30%) compared with more mature infants (20%). Rao et al 10 also found preterm infants who received TH had a higher rate of mortality and white matter injury compared with term infants who received TH. These studies were limited by small numbers.
The primary aim of this study was to establish the incidence of HIE in the TH era. The secondary aim was to evaluate mortality and changes to TH management.
Methods
Study population
The National Neonatal Research Database (NNRD) holds prospectively recorded daily clinical data from every infant admitted to UK neonatal units along with outcomes. The NNRD contains an approved clinical database (the National Neonatal Data Set), within the NHS Data Dictionary national electronic data set,13 and provides newborn brain injury data in the UK.2 In 2011, approximately 90% of English neonatal units contributed to the NNRD and no units from Wales. From 2012 onwards, all units contributed to the database. Data are screened for errors and amended prior to entry into the database.
Data from the Office for National Statistics (ONS) were used as denominator data (excluding Scotland and Northern Ireland) to calculate national incidence rates of HIE using live birth by GA for each year of the study period.14
Data collection
Data were extracted on all infants 34–42 weeks GA who were admitted to neonatal units in England and Wales from 2011 to 2016. Infants with HIE were identified using the ‘Principal Diagnosis at Discharge’ and ‘HIE score’ data fields, as diagnosed and inputted by the clinical teams in each centre (online supplemental table 1), and allocated the most severe HIE grade issued during their admission. Infants managed with any TH were identified using the ‘Principal Procedures During Stay’ or ‘Principal Diagnosis at Discharge’ or ‘Therapeutic Hypothermia’ data fields. Infants who did not have a diagnosis of HIE but received TH were not categorised as HIE.
Supplemental material
Infants weighing greater than 5500 g (erroneous data) or missing key episode data items (GA, principal diagnosis, place of birth or mortality data) were excluded from the study.
Outcome
The primary aim was the incidence of HIE by live births for England and Wales in the TH era. The secondary aims were to evaluate the management of these infants and mortality and describe any temporal changes.
Statistical analysis
Extrapolation methods based on actual admission numbers and number of cases from 2012 to 2016 when all units contributed to the database were used to estimate the incidence of HIE for 2011 as previously described.2
The population incidence rate of HIE per 1000 live births was calculated using NNRD data to identify cases and ONS data for live birth rates per year by GA as the denominator. The study population was divided into two equal epochs (2011–2013 and 2014–2016) to evaluate any changes over time. Infants with moderate/severe HIE who died without undergoing TH were considered with babies who received TH for analysis as these are likely to represent infants who met the cooling criteria but were too sick to undergo treatment or care was reorientated; data for babies who died without undergoing TH are also presented.
For subgroup analyses, infants were further divided into late preterm (34–35 weeks GA) and mild (grade 1) HIE subgroups. Associations between demographic, clinical variables and death were assessed using χ2 test for categorical data and Mann-Whitney U test for non-normally distributed continuous data. Subgroup characteristics were compared and analysed with univariate analysis and presented as unadjusted OR with 95% CI. All statistical analyses were performed using Stata SE V.15.
Results
A total of 407 462 infants were admitted for neonatal care during the study period. Of these, 12 195 infants had a recorded diagnosis of HIE, giving an incidence of 2.96 per 1000 live births and accounting for 3% of neonatal unit admissions ≥34 weeks GA (online supplemental figure 1). Mortality for all infants with recorded HIE was 7.0% (n=851).
The incidence of moderate/severe HIE in infants ≥36 weeks GA was 2.03 per 1000 (n=8166); 1.26 per 1000 (n=5069) were treated with TH (n=4949) or died without TH treatment (n=120) (table 1, online supplemental table 2). The incidence of moderate/severe HIE in infants ≥36 weeks GA remained similar between epochs (table 1), but TH treatment significantly increased between epochs (54.6% vs 66.6%, p<0.001).
Incidence of HIE for the whole study population, infants ≥36 weeks gestational age with moderate/severe HIE and infants ≥36 weeks gestational age with moderate/severe HIE treated with TH
Comparison of antenatal and delivery characteristics of infants ≥36 weeks GA admitted to neonatal units with moderate/severe HIE who received, or died without, TH or did not receive TH
The characteristics of infants ≥36 weeks GA with moderate/severe HIE who did or did not undergo TH were compared (table 2). Overall, 62.1% (n=5069) of infants ≥36 weeks GA with moderate/severe HIE were cooled or died without TH. These infants were significantly more likely to have a background of acute intrapartum events, need for significant resuscitation, lower Apgar scores and lower cord venous pH compared with non-cooled infants. Mortality of infants ≥36 weeks GA with moderate/severe HIE was 9.3% (n=762) and decreased over time between epochs (10.0% vs 8.7%; OR 0.85 (95% CI 0.74 to 0.99), p=0.04). For those undergoing TH (excluding infants who died prior to cooling), there was a significant reduction in mortality between 2011–2013 (n=336, 15.1%) and 2014–2016 (n=297, 10.9%; OR 0.67 (95% CI 0.58 to 0.81), p<0.001). This pattern remained evident after inclusion of infants who died prior to cooling (mortality in epoch 1: 17.5% (n=402); epoch 2: 12.3% (n=355); OR 0.69 (95% CI 0.59 to 0.81), p<0.001). Overall, infants born between 2014 and 2016 had a higher rate of early infection and significant resuscitation (online supplemental table 3).
Infants ≥36 weeks with mild HIE
There were 3394 infants ≥36 weeks GA diagnosed with mild HIE (0.84 per 1000 live births), similar between 2011–2013 (n=1712) and 2014–2016 (n=1682, p=0.57). Mortality was low in this population, with six deaths overall and no difference over time, although infants admitted in 2014–2016 had a higher rate of early infection and significant resuscitation (online supplemental table 4). In total, 1027 (30.3%) were managed with TH and 338 (10.0%) were transported within the first 48 hours from non-tertiary units into a cooling centre. The proportion of infants treated with TH significantly increased over time between 2011–2013 (n=426, 24.9%) and 2014–2016 (n=603, 35.8%, p<0.001).
The characteristics of infants ≥36 weeks GA with mild HIE who did or did not undergo TH were compared (table 3). Those who received TH (including the six infants who died without TH treatment) had a lower birth weight, required more resuscitation, had lower Apgar scores and had lower cord venous pH. Infants with moderate/severe HIE were significantly more likely to have acute intrapartum events, require significant resuscitation and have lower Apgar scores compared with infants with mild HIE (online supplemental table 5).
Comparison of antenatal and delivery characteristics between infants ≥36 weeks GA admitted to neonatal units with mild HIE who received, or died without, TH or did not receive TH
Late preterm infants (34–35 weeks)
In total, 635 late preterm infants (6.27 per 1000) were diagnosed with any grade HIE (online supplemental table 6); this remained stable through epoch 1 and epoch 2 with 6.00 per 1000 vs 6.55 per 1000, respectively (p=0.27). Of these 81.5% (n=518) had moderate/severe HIE. Late preterm infants treated with TH were significantly more likely to have acute intrapartum events, require significant resuscitation, have lower Apgar scores and have lower cord venous pH (table 4).
Comparison of antenatal and delivery characteristics of infants 34–35 weeks GA admitted to neonatal units with hypoxic-ischaemic encephalopathy who received, or died without, TH or did not receive TH
Among late preterm infants, 259 (40.8%) were treated with TH (n=210) or died without TH (n=49). This significantly increased between epoch 1 (n=103, 34.3%) and epoch 2 (n=156, 46.6%, p=0.002), although mortality remained unchanged (n=36 (12.0%) vs n=47 (14.0%), p=0.51). The rate of moderate/severe HIE and the associated mortality were greatest in the late preterm population compared with those ≥36 weeks GA (p<0.001; figure 1 and online supplemental table 6). The characteristics between epochs were similar (online supplemental table 7). Overall, mortality in infants with moderate/severe HIE in the late preterm population was 16.0% (n=83) compared with those ≥36 weeks GA at 9.3% (n=762, p=0.005).

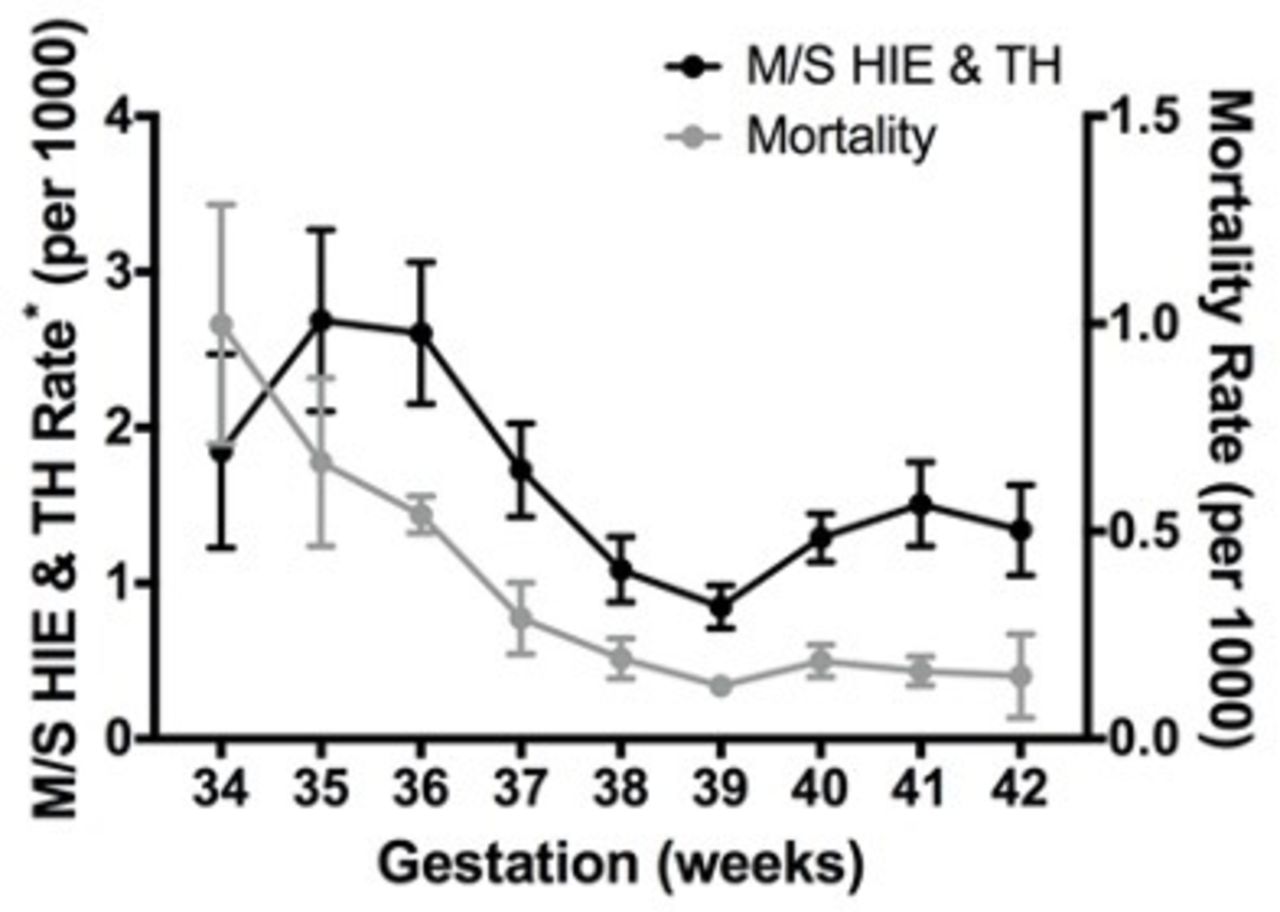{kind=link}
Rate of moderate/severe HIE treated with therapeutic hypothermia and mortality within the study population per 1000 live births at each gestational week. *Data include infants with M/S HIE but were not cooled. HIE, hypoxic-ischaemic encephalopathy; M/S, moderate/severe; TH, therapeutic hypothermia.
Discussion
This large national population-based study has shown the incidence of recorded moderate/severe HIE in infants ≥36 weeks GA remains similar over time, but there has been a reduction in mortality. Based on national guidance for HIE, only 62.1% of eligible infants received TH. Furthermore, we have shown for the first time the increasing number of infants with mild HIE and those born late preterm undergoing TH, without sufficient evidence to support this approach. During the most recent epoch, TH was administered to 36% of infants with mild HIE and 47% of late preterm infants with HIE. These findings are important particularly for late preterm infants where mortality associated with moderate/severe HIE increases with decreasing gestation.
Following publication of the TOBY trial4 and the national guidance for TH,5 treatment with TH for moderate/severe HIE in infants ≥36 weeks GA has increased in England and Wales, with a reduction in mortality. Mortality for infants undergoing TH has decreased by more than half since the TOBY study from 23.9%4 to 15.1% in 2011–2013 and 10.9% in 2014–2016. These findings could reflect changes in practice with earlier recognition and treatment, mild cases being diagnosed as moderate and undergoing TH, as well as improving intensive care management. In our study, 37.9% of infants with recorded moderate/severe HIE did not receive TH. These infants may include those who were too sick to cool or in whom HIE was diagnosed outside the therapeutic cooling window. The clinical decisions for not cooling an eligible infant are not recorded within this database. However, the grading of HIE can be subjective, leading to some clinicians opting not to treat borderline infants, whereas others may have graded these infants as moderate HIE. Likewise, infants may have been incorrectly misclassified as HIE or misdiagnosed as mild and therefore not cooled. Another potential explanation is that TH use was recorded inaccurately or was unrecorded despite being administered; however, TH data are used to reimburse individual hospitals so this data item is usually well recorded. Our findings do, however, potentially suggest a large proportion of eligible infants do not receive TH.
The number of infants with mild HIE undergoing TH has increased over time and their mortality rate is very low. Previous studies of infants with mild HIE demonstrated an increased risk of mortality and adverse neurological outcome.15–17 However, TH in these infants has not been shown to reduce death or neurodisability,7 8 although one study reported less brain injury on MRI scans.18 Management of these infants with TH in the absence of robust evidence risks exposing them to unnecessary treatment with its associated morbidity, such as pain and respiratory support.19 20 In the UK, TH is mainly undertaken in tertiary centres, increasing the pressure on cot capacity and specialist neonatal transportation services21 with the need to transfer more infants. Current, ongoing prospective studies (Therapeutic Hypothermia for Infants with Mild Encephalopathy(TIME)22 and Optimising the Duration of Cooling Therapy in Mild Neonatal Encephalopathy (COMET)23) may provide much needed evidence to establish the benefit and safety of TH use for mild HIE.
To our knowledge, this is the largest study to date of late preterm infants with HIE including those treated with TH. Our study has shown preterm infants have a higher incidence rate of moderate/severe HIE diagnosed compared with term infants. The TOBY study demonstrated TH was a safe and effective treatment in infants ≥36 weeks GA,4 yet TH is increasingly being used in late preterm infants. Other large randomised controlled trials of TH for HIE included infants at 35 weeks GA but did not separately report their outcomes.19 24 25 The pathophysiology of brain injury in late preterm infants is likely to be different from those at term; Rao et al 10 reported a higher incidence of white matter injury and mortality due to the severity of the encephalopathy in late preterm infants. Our study also demonstrated late preterm infants with moderate/severe HIE were four times more likely to die than infants ≥36 week GA (0.80 per 1000 vs 0.19 per 1000 live births), highlighting the need for well-designed prospective randomised controlled studies to evaluate the safety and efficacy in this subgroup.
Strengths and limitations
The study’s main strength is the use of national data set from a reliable database of prospective, routinely recorded data.26 This has allowed analysis with a large sample size and provides an estimate of the incidence of HIE within a national healthcare service. To our knowledge, this study has analysed the largest group of late preterm infants with HIE to date compared with previous studies.10–12 27 28 Because only 90% of neonatal units contributed to the NNRD in 2011, we calculated the lower and upper estimates of missing data using actual data from admission and HIE rate from 2012 to 2016.2
A further strength is the analysis of data after the introduction of a national guideline providing diagnostic criteria for treatment,5 although we acknowledge clinical evaluation and grading of HIE are subjective and may lead to variations in diagnosis. Furthermore, the database does not hold the individual components of the scoring system, so we were limited by the diagnostic coding of the clinical team caring for the infant. To address the ambition to minimise newborn brain injury in the UK,6 it would be useful to standardise recorded data with diagnostic criteria and outcomes, allowing more robust national rates and comparisons between centres. Inclusion of additional data fields based on established severity scoring systems (including modified Sarnat score and amplitude-intergrated electroencephalography (aEEG) as specified in UK guidance29) could help in standardisation and accuracy of data entry.
The main limitation of studies using large databases is the errors or imprecision in data entry. This is limited through screening the data for erroneous entries, although this cannot mitigate completely if the data are incorrect at the point of entry. A further limitation is that we do not have neuroimaging results or long-term neurodevelopmental outcome data as these are not recorded in the database or are often incomplete, making analysis unreliable. These outcomes would be of significant interest with such a large data set and are more useful as a measure of brain injury, than the requirement for TH treatment alone, as many infants will have a normal outcome without injury.
Conclusion
The use of TH for infants with moderate/severe HIE is increasing and is associated with a reduction in mortality, although a large proportion of potentially eligible infants do not receive treatment. There are also increasing numbers of infants with mild HIE and late preterm infants with HIE undergoing TH outside of the current evidence base. These data highlight the urgent need for initiatives to improve delivery of effective evidence-based practice to all eligible infants and well-designed, prospective studies to evaluate the safety and efficacy in late preterm infants and those with mild HIE.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. All data were extracted and supplied by the NDAU and are available from the corresponding author on reasonable request and with permission of the study team and NDAU.
Ethics statements
Ethics approval
Ethical approval was given by the London-City and East Research Ethics Committee (REC: 17/LO/1822).
Acknowledgments
Electronic patient data recorded at participating neonatal units that collectively form the UK Neonatal Collaborative (UKNC) are transmitted to the Neonatal Data Analysis Unit (NDAU) to form the National Neonatal Research Database (NNRD). We are grateful to all the families that agreed to the inclusion of their baby’s data in the NNRD, the health professionals who recorded data and the NDAU team.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrCGale, @DrDonSharkey
Contributors LS and DS made substantial contributions to the concept, planning, design of the study and acquisition of data. LS and DS analysed and interpreted the data. All authors assisted in drafting and editing the manuscript. All authors approved the final version for publication. DS had full access to all the data in the study and takes full responsibility for the integrity of the data and accuracy of the data analysis.
Funding This study was partly supported by a University of Nottingham, School of Medicine Impact Funding award.
Competing interests CG has received support from Chiesi Pharmaceuticals to attend an educational conference; in the past 5 years he has been an investigator on received research grants from Medical Research Council, National Institute for Health Research, Canadian Institutes of Health Research, Department of Health in England, Mason Medical Research Foundation, Westminster Medical School Research Trust and Chiesi Pharmaceuticals, and has been an unremunerated member of the Neonatal Data Analysis Unit Board, which oversees the NNRD.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Fantoms