Article Text

Abstract
Objective To compare rectal and axillary temperatures in preterm newborns on admission to the neonatal intensive care unit (NICU).
Design Secondary analysis of data collected in a randomised controlled trial (RCT).
Setting Maternity hospital, level 3 NICU.
Patients Seventy-two newborns <31 weeks who were enrolled in the BAMBINO RCT (A randomised trial of exothermic mattresses to prevent heat loss in preterm infants at birth, ISRCTN31707342).
Interventions Newborns were placed in polyethylene bags and were randomised to placement on exothermic mattresses, or not in the delivery room. All infants had rectal and axillary temperatures measured in immediate succession using a digital thermometer on NICU admission.
Outcome measures Admission rectal and axillary temperatures.
Results Mean (SD) gestational age was 28 (2) weeks and birth weight was 1138 (374) g. Mean rectal-axillary temperature difference was 0.1 (0.5°C) (range −1.4°C to +1.5°C). Rectal and axillary temperatures differed by ≥0.5°C in 18/72 (25%) infants; axillary temperature was higher than rectal in 6 (8%) and lower in 12 (17%). There was a positive linear relationship between rectal and axillary measurements (Pearson’s correlation R=0.84). Applying the Bland-Altman technique, the width of 95% prediction interval was 1.8°C (−0.8°C to 1.0°C) implying that rectal and axillary measurements may vary by up to 1.0°C. Axillary temperature had a sensitivity of 65% when used to detect rectal hyperthermia and 100% sensitivity for hypothermia.
Conclusion Paired rectal and axillary temperature measurements in preterm newborns on NICU admission vary significantly. Axillary temperature was sensitive at detecting rectal hypothermia but not hyperthermia. Axillary temperature may not be an accurate proxy for rectal temperature measurement in all preterm newborns on NICU admission.
- infant, newborn
- preterm
- temperature
- hypothermia
- hyperthermia
- NICU
Data availability statement
Data are available on reasonable request to LKMC. The identified clinical data are held on password-protected computers at the National Maternity Hospital, Dublin.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
In preterm newly born infants, abnormal temperature on admission to the neonatal intensive care unit (NICU) is associated with adverse outcome.
The WHO defines normal body temperature for infants as 36.5°C–37.5°C.
In the NICU, temperature is often measured at the axilla rather than the rectum as it is more accessible and less invasive.
What this study adds?
Rectal and axillary temperature measurements in preterm newborns on NICU admission may vary considerably.
Axillary temperature was sensitive for detecting rectal hypothermia but not hyperthermia.
Axillary temperature may not be an accurate proxy for rectal temperature measurement in all preterm newborns on admission to the NICU.
Background
Newborn preterm infants lose heat rapidly after birth. Despite measures to prevent heat loss during stabilisation in the delivery room (DR) many preterm newborns have abnormal temperature on admission to the neonatal intensive care unit (NICU).1 Abnormal temperature on NICU admission is an independent risk factor for morbidity and mortality in very preterm newborns.2–4
The WHO defines normal body temperature for infants as a core temperature of 36.5°C–37.5°C.5 There is no gold standard for measuring body temperature, but temperature measured at the rectum is considered to be representative of core body temperature (temperature around the hypothalamus) and is a more pragmatic approach to measuring infant temperature. Trends in rectal temperature measurements are reflective of changes in core temperature with sufficient accuracy to guide clinical care.6 In the NICU, temperature is often measured at the axilla rather than the rectum as it is more accessible and less invasive. Older studies using glass and mercury thermometers have reported complications when measuring rectal temperatures in infants.7–9 There are conflicting data on how well rectal and axillary temperature measurements correlate when taken with digital thermometers in infants in the NICU.
Pooled data from a review of 20 studies of 3201 term infants and children showed a wide variation in rectal and axillary temperatures across studies. The pooled, random effects mean temperature difference (rectal minus axillary temperature) for electronic thermometers in this meta-analysis was 0.85°C (−0.19°C to 1.90°C). There was less variability in the pooled mean temperature difference for newborns: 0.17°C (−0.15°C to 0.50°C); however, most of the included studies used mercury thermometers.10 In a study of 63 term infants >1 hour of age admitted to the NICU, Cusson et al observed moderate correlation between rectal and axillary temperatures measured with the IVAC digital thermometer.11 Hissink Muller et al reported a wide variation between paired rectal and axillary temperature measurements using digital thermometers (Thermoval Waterproof) in 33 infants (25–42 weeks’ gestation) in the NICU. The authors concluded that the two measurements should not be used interchangeably as infants in their study had significantly lower axillary temperatures (0.27°C±0.20°C) and the 95% limits of agreement ranged from −0.13°C to 0.67°C.12 Roll et al compared rectal and axillary temperatures in 20 very preterm and unstable term neonates in the NICU. In their subgroup analysis, mean axillary temperature was only 0.06°C lower than rectal temperature in infants <1000 g compared with 0.37°C lower at the axilla in infants >2500 g.13
Most studies report data on rectal-axillary temperature correlations in non-newborn, stable, normothermic infants at different stages during their NICU admission. There are little data on the correlation between rectal and axillary temperatures in newborn very preterm infants on admission following stabilisation in the DR. Many of these infants are not normothermic and are not clinically stable. Abnormal temperature at this time, in this population, is associated with adverse outcome.2–4
The objective of this study was to compare rectal and axillary temperatures in newborn very preterm infants <31 weeks’ gestation measured with digital thermometers on admission to the NICU.
Patients and methods
Study design
This is secondary analysis of data collected prospectively in cohort of newborn preterm infants enrolled in a randomised controlled trial (RCT) conducted at the National Maternity Hospital, Dublin, Ireland, between February 2011 and February 2012.
Participants
Infants in this study were enrolled in the BAMBINO RCT (A randomised trial of exothermic mattresses to prevent heat loss in preterm infants at birth, ISRCTN31707342).14 Inborn infants <31 weeks’ gestation were eligible for inclusion. We compared rectal temperature on NICU admission in preterm newborns wrapped in polyethylene bags (PB) to infants wrapped in PB and placed on exothermic mattresses (EM) in the DR. We found that more infants who were placed on EM had temperatures outside the range of 36.5°C–37.5°C and were more likely to be hyperthermic on admission to the NICU. The trial was stopped early due to the high rate of hyperthermia detected in infants in the EM group, as measured by rectal temperature.14
DR care
After birth, all infants were transferred to a CosyCot Infant Warmer. They were placed without drying in a bag with a hat placed on their head. Infants randomised to treatment with an EM were placed on an activated TransWarmer mattress (Cooper Surgical, Trumbull, Connecticut, USA). Stabilisation was otherwise carried out in accordance with international recommendations.15 16 Infants in both groups were transferred to the NICU in transport incubators. All infants remained in their PB and those randomised to the EM group remained on their mattress for transfer.
Temperature on NICU admission
On arrival to the NICU, all infants had a rectal and axillary temperature measurement taken in immediate succession using the Vicks V900F-EE SmartTemp Digital Thermometer (Procter & Gamble, Ohio, USA). This thermometer was the standard digital thermometer used in the NICU at that time and is licensed for oral, axillary and rectal use in children and infants. The manufacturer states that the accuracy of the thermometer is ±0.1°C between 35.5°C and 41.6°C at room temperature of 21.6°C; and its temperature range is 32.0°C–42.8°C. They say that the thermometer is calibrated at the time of manufacture and if the instructions are followed, the accuracy of measurements will not be affected.
Rectal temperature was measured first in all cases. Caregivers were instructed to turn the thermometer on, wait for it to signal before opening the incubator portholes, then open the PB and gently insert the tip of the thermometer into the rectum to 1 cm. The thermometer displayed the temperature continuously until it signalled again (eight beeps) that peak temperature was reached (~30 s). For axillary readings the thermometer was placed in the axilla with the tip touching the skin and the reading awaited as previously described. The same thermometer was used for both measurements and was cleaned with an alcohol wipe between readings. Infants remained inside the transport incubator, wrapped in a PB with or without an EM until the temperature was measured. Demographic data on gestational age, birth weight, gender, multiple births, mode of delivery, maternal fever, respiratory support in the DR, proportion of infants placed on EM in the DR and time from birth to NICU admission were recorded.
Statistical analysis
Data were analysed using SPSS V.18.0. Continuous outcome variables with a normal distribution were expressed as mean (SD) and variables with an abnormal distribution as median (IQR). Differences between temperature readings were analysed using a Student’s paired t-test. A p value <0.05 was taken to be statistically significant. Dichotomous variables were expressed as numbers and percentages. We determined the Pearson’s correlation (R) between rectal and axillary temperatures and presented the data in a scatterplot. The degree of agreement between temperature measurements recorded at the axilla and rectum was assessed using the Bland-Altman technique. The difference between their measurements was plotted against their average. Two SDs around the mean difference represented the upper and lower limits of agreement.17 18
Results
Seventy-two infants <31 weeks’ gestation were enrolled in the BAMBINO trial. All 72 infants enrolled in the trial at the time of stopping were included for analysis in this study. All infants had a rectal and axillary temperature measured on admission to the NICU. In the DR, all infants were wrapped in PB and 37 (51%) were placed on EM. The mean (SD) gestational age was 28 (2) weeks and the mean (SD) birth weight was 1138 (374) g. Twenty-nine infants were <28 weeks’ gestation. All 72 infants received respiratory support and 10 (14%) were intubated in the DR. The median (IQR) age at the time of admission was 20 (17, 26) min (table 1).
Results: characteristics of 72 infants enrolled in the study
The mean (SD) rectal-axillary temperature difference was 0.1 (1.5)°C, with a range of −1.4°C to +1.5°C. Rectal and axillary temperatures differed by ≥0.5°C in 18/72 (25%) infants; axillary temperature was higher in 6 (8%) infants and lower in 12 (17%). Using the Bland-Altman technique, we plotted the difference between each pair of readings against the average rectal and axillary temperatures (figure 1). Overall, the temperature readings correlated well (Pearson’s correlation R=0.84, figure 2) but our analysis showed that the width of the 95% prediction interval was 1.8°C (from –0.8°C to 1.0°C). This suggests that individual rectal and axillary temperature measurements may vary by up to 1.0°C.
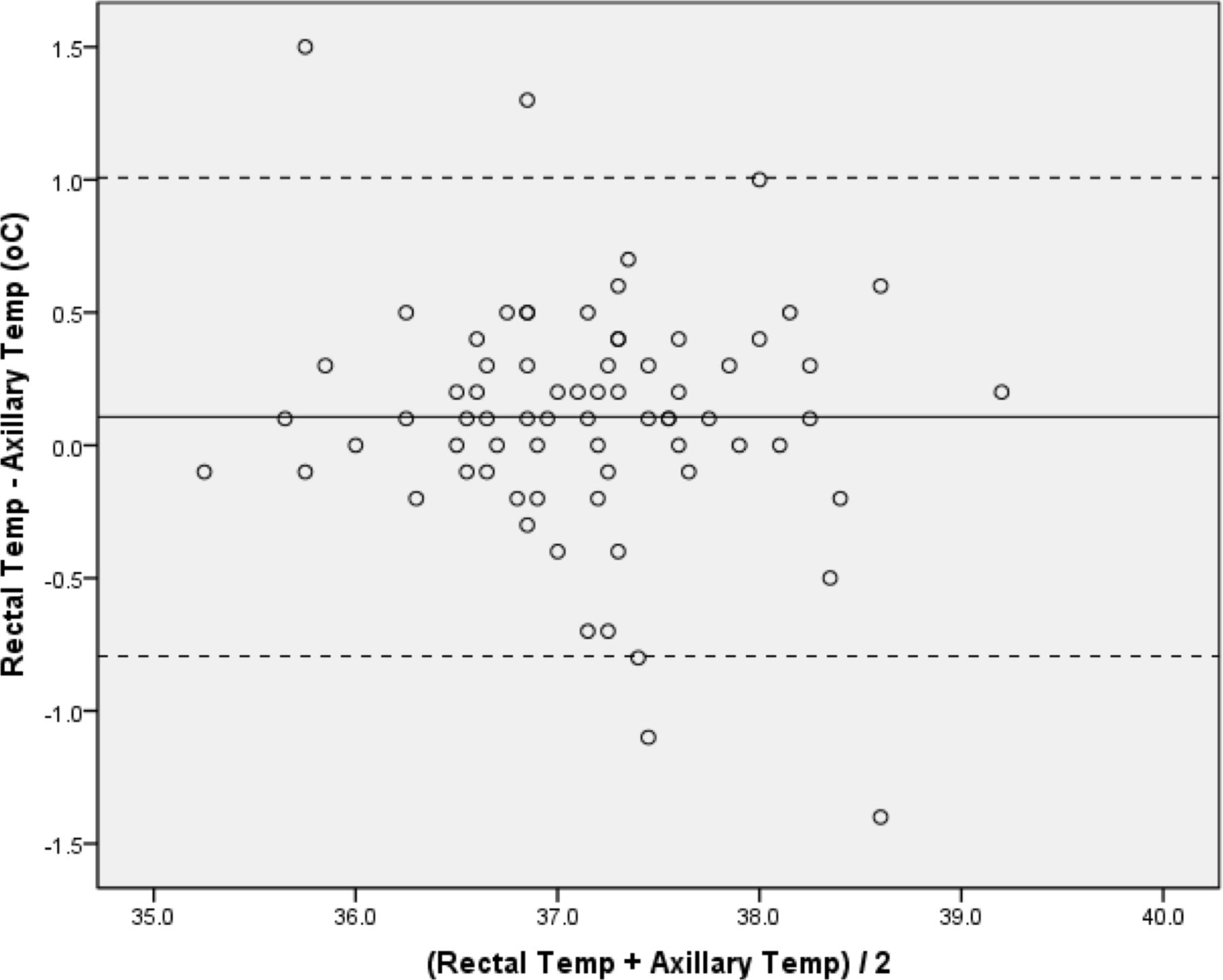
Results: Bland-Altman plot for rectal and axillary temperature measurements on neonatal intensive care unit admission. The solid line represents the mean (rectal-axillary) difference and dashed lines represent the 95% limits of agreement.

{kind=link}
{kind=link}
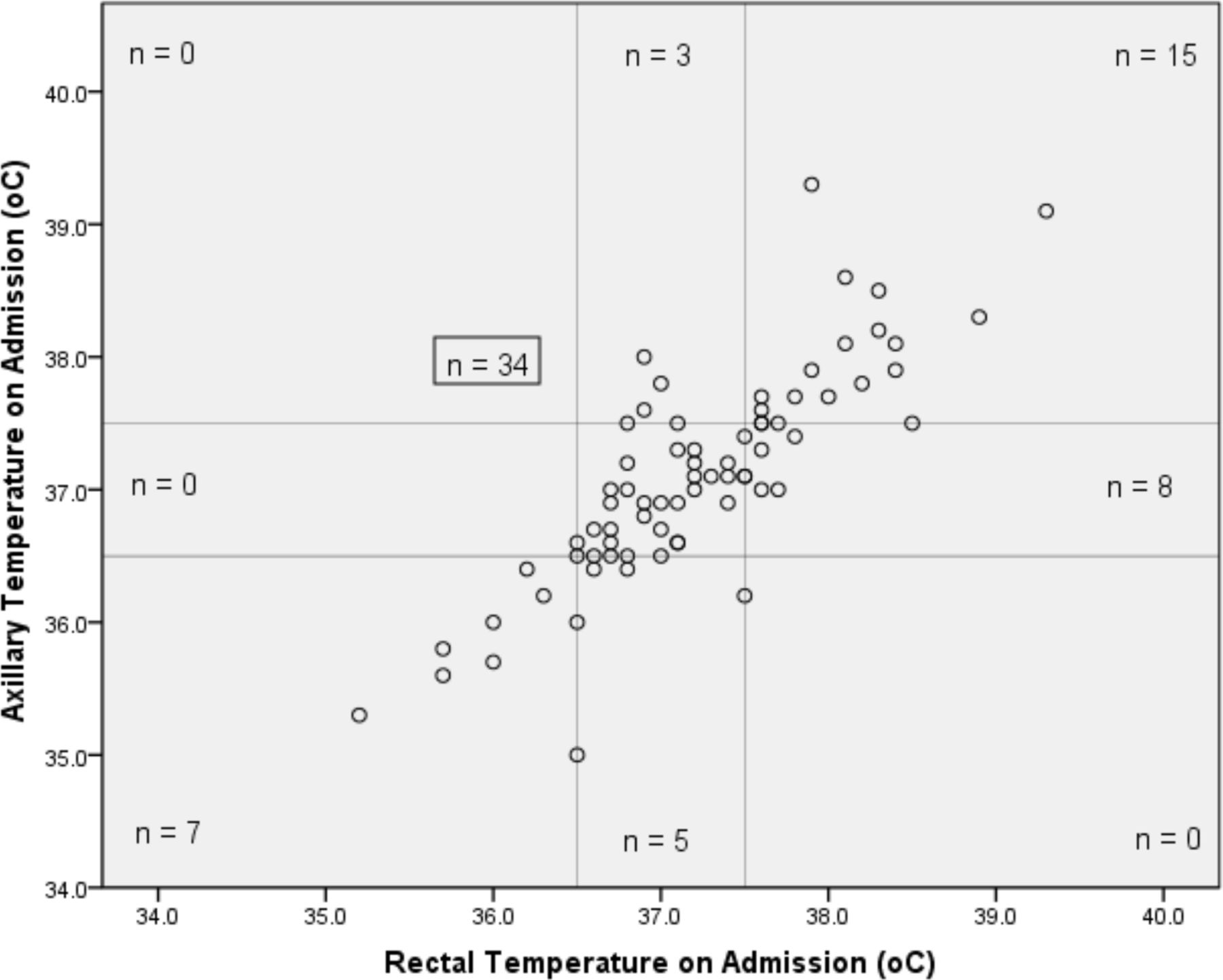
Results: scatterplot of rectal and axillary temperatures on admission to the neonatal intensive care unit (n=72). The vertical and horizontal lines represent the normal temperature range (36.5°C–37.5°C). Pearson’s correlation R=0.84, R2=0.69.
Hyperthermia is defined as a temperature >37.5°C and hypothermia <36.5°C.5 In this cohort, 42 infants had a normal rectal temperature, and of these 34 infants had a normal axillary temperature (figure 2). Axillary temperature measurements were a reasonably sensitive marker for rectal normothermia (sensitivity: 81% (34/42), positive predictive value (PPV): 81% (34/42)) and although the numbers were small (n=7), axillary temperature was an excellent marker for rectal hypothermia (sensitivity: 100% (7/7), negative predictive value: 100% (60/60)). However, when axillary temperature was used to detect rectal hyperthermia it had low sensitivity of 65% (15/23) (figure 2).
Discussion
In this study, mean rectal temperature was 0.1°C higher than axillary temperature in newborn preterm infants on admission to the NICU. This, however, does not adequately describe the agreement between the two measurements. We applied the Bland-Altman method of analysis to further assess the relationship between rectal and axillary temperatures and found that although the mean difference appeared small (0.1°C), the width of the 95% prediction limits for the difference between rectal and axillary temperatures was ±0.9°C. This suggests that in some cases there was wide variability between the paired readings of up to 1.0°C. The normal temperature range for infants is narrow, between 36.5°C and 37.5°C, therefore a difference of up to 1°C in temperature readings may be the difference between normal and abnormal temperatures. This may have significant implications for adverse outcome.
In our cohort, the axillary temperature was a reasonably sensitive marker for rectal normothermia and highly sensitive for hypothermia. In all seven cases, infants with axillary hypothermia had a low rectal temperature. These infants are at increased risk of death as a result of their admission hypothermia.2 3 Conversely, our analysis suggests that axillary temperature is quite insensitive at detecting admission temperature >37.5°C; and misses up to 35% of infants with rectal hyperthermia. In the past, this was less relevant as most infants were hypothermic on admission and few had temperatures >37.5°C.19–21 Due to improved awareness and more effective warming strategies the number of infants with high temperatures on admission is increasing.1 14 22 23 Compared with hypothermia, less is known about the long-term consequences of hyperthermia after birth in preterm newborns. Hyperthermia in asphyxiated term infants is associated with adverse neurodevelopmental outcomes.24 25 In their study of >9000 infants <33 weeks, the Canadian Neonatal Network demonstrated a U-shaped relationship between admission temperature and adverse neonatal outcomes. Both hypothermia and hyperthermia were associated with higher rates of complications of prematurity; complications were lowest at admission temperatures ranging from 36.5°C to 37.2°C.4 The newborn resuscitation guidelines emphasise the importance of maintaining normothermia and avoiding hyperthermia.15 16
The mean rectal-axillary temperature difference of 0.1°C that we observed is less than the mean difference reported in previous studies (0.17°C,10 0.27°C,12 0.16°C13 and 0.7°C26). This may be because the infants in our study were a more homogenous group; they were all preterm and their temperatures were measured at the same time point. One study included infants up to 6 months of age in hospital and at home,26 others monitored temperature at different times during infant’s NICU admission13 and some analysed term and preterm infants together.10 12 Results of the subgroup analysis in preterm infants in one study suggest that the correlation between rectal and axillary temperatures is closer in preterm infants than in larger term infants.13 There is also evidence that this correlation is strongest in the days closest to birth and weakens as infants mature.27 28
Few studies report data on very preterm newborns on admission to the NICU. One of the strengths of our study is that we report prospective data in a relatively homogenous, reasonably large group of preterm newborns at the same point in time. We measured the rectal and axillary temperatures for each infant using the same thermometer in immediate succession. No interventions were carried out between readings to adjust the infant’s temperature so it is unlikely that changes in body temperature were responsible for the differences in temperature readings.
There are a number of limitations to our study. Although we used the same thermometer to measure the rectal and axillary temperatures, different nurses with varying degrees of experience carried out measurements in different infants. However, the thermometers and the techniques used were the same as are routine in clinical care and the manufacturer’s instructions were followed. There are a number of potential problems with temperature readings at both sites and error can occur depending on the placement of the probe. At the axilla temperature readings may differ depending on adequate closure of the axillary fold, blood flow to the axillary region and potentially activation of non-shivering thermogenesis.27 28 Rectal temperature readings may also vary depending on the depth of insertion of the probe and whether faeces are present. We performed additional subgroup analysis to examine the sensitivity and PPV of axillary temperature for rectal temperature in infants in the ‘PB’ group, ‘EM’ group and for infants <28 weeks’ gestation. A similar positive linear correlation was observed between axillary and rectal temperature readings in the subgroups but the numbers were too small to report sensitivity and PPV meaningfully. The additional analysis, with its small numbers, did not suggest that in certain circumstances (ie, in a bag and on a mattress, or only in a bag, or <28 weeks) axillary temperature is more accurate.
There is sometimes a reluctance to carry out rectal temperature measurements in newborn infants because it is deemed to be invasive, and in the past was associated with rectal perforation. The risk of rectal injury caused by rectal temperature measurement is extremely small26 and most of the published case reports of rectal injury refer to mercury-in-glass thermometers that are no longer used. Mercury thermometers have been replaced by plastic, digital thermometers with narrow, smooth probes that only take 30 s to read and are less likely to break or cause trauma. A potential benefit of taking rectal temperature, in addition to being more accurate, is the early identification of anal patency.
Conclusion
Paired rectal and axillary temperature measurements in preterm newborns on NICU admission may vary significantly. Axillary temperature was sensitive at detecting rectal hypothermia but not hyperthermia. Axillary temperature may not be an accurate proxy for rectal temperature measurement in all preterm newborns on admission to the NICU.
Data availability statement
Data are available on reasonable request to LKMC. The identified clinical data are held on password-protected computers at the National Maternity Hospital, Dublin.
Ethics statements
Ethics approval
The trial was approved by the NMH Research and Ethics Committee and written informed consent was obtained from a parent or guardian before delivery.
Acknowledgments
We thank Ricardo Segurado, consultant biostatistician, at the Centre for Support and Training in Analysis and Research (CSTAR), University College Dublin, for his help with the statistical analysis of our data. We also offer sincere thanks to the families of all babies who participated in our study.
References
Footnotes
Twitter @Lisa
Contributors Conception and design of the work: LKMC, CPFOD. Data collection: LKMC. Data analysis and interpretation: LKMC, CPFOD with statistical analysis support from CSTAR. Drafting the article: LKMC. Critical revision of the article: LKMC, CPFOD. Final approval of the version to be published: LKMC, CPFOD. Study supervision: CPFOD.
Funding This work was supported by the National Children’s Research Centre, Crumlin, Dublin, Ireland.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.