Article Text

Abstract
Objective Patient’s work of breathing may vary between different neonatal nasal continuous positive airway pressure (NCPAP) devices. Therefore, we aimed to compare the inspiratory effort of three variable-flow NCPAP delivery systems used in preterm infants.
Design Cross-over study.
Patients/setting From June 2015 to August 2016, 20 preterm infants weighing ≤2500 g requiring NCPAP for mild respiratory distress syndrome were enrolled.
Interventions Each patient was successively supported by three randomly assigned variable-flow NCPAP systems (MedinCNO, Infant Flow and Servo-i) for 20 min while maintaining the same continuous positive airway pressure level as the patient was on before the study period.
Main outcome measures Patients’ inspiratory effort was estimated by calculating the sum of the difference between maximal inspiratory and baseline electrical activity of the diaphragm (∆EAdi) for 30 consecutive breaths, and after normalising this obtained value for the timing of the 30 breaths.
Results Physiological parameters (oxygen saturation measured by pulse oximetry, respiratory rate, heart beat, transcutaneous partial pressure CO2) and oxygen requirements remained identical between the three NCPAP systems. Although a wide variability in inspiratory effort could be observed, there were no statistically significant differences between the three systems for the sum of ∆EAdi for 30 breaths: CNO, 262 (±119) µV; IF, 352 (±262) µV; and SERVO-i, 286 (±126) µV, and the ∆EAdi reported on the timing of 30 breaths (sum ∆EAdi/s): CNO, 6.1 (±2.3) µV/s; IF, 7.9 (±4.9) µV/s; SERVO-i, 7.6 (±3.6) µV/s.
Conclusion In a neonatal population of preterm infants, inspiratory effort is comparable between the three tested modern variable-flow NCPAP devices.
- neonatology
- physiology
- qualitative research
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Imposed work of breathing (iWOB) might vary between constant-flow and variable-flow neonatal nasal continuous positive airway pressure (NCPAP) devices, with a strong advocacy in favour of variable-flow devices.
Newer neonatal ventilators have incorporated variable-flow continuous positive airway pressure, offering with various working principals for flow/pressure generation between devices.
Bench tests have suggested that iWOB might be different between such modern variable-flow devices.
What this study adds?
Measurements in preterm infants could not show any relevant differences in estimated inspiratory effort between three types of modern variable-flow NCPAP devices using various pressure generation principals.
Introduction
Nasal continuous positive airway pressure (NCPAP) has been shown to significantly reduce the need for mechanical ventilation and to increase survival in preterm infants with respiratory distress.1–3 A meta-analysis concluded that compared with prophylactic surfactant, early NCPAP with selective surfactant therapy decreases death or bronchopulomonary dypslasia(BPD).4 Two major categories of NCPAP devices exist in the market: constant-flow and variable-flow devices.5 6 With a continuous-flow NCPAP device, the flow remains constant, while pressure is adjusted by changes in resistance to exhalation (eg, at the expiratory valve of the ventilator circuit if a ventilator-generated continuous positive airway pressure (CPAP) is used). In contrast, the variable-flow NCPAP device keeps airway pressure constant by varying the flow at the airway, proximal to the infant’s nares.7 Variable-flow devices use various principles to modify flow at the nasal interface (with a special nosepiece) or within the ventilator. The CNO (Medin Medical Innovations, Puchheim, Germany) uses a Benveniste gas-jet valve7 that consists of a straight nozzle and a curved tube positioned coaxially, which allows for flow modification. A leak compensation algorithm increases flow rate when a pressure drop at the nosepiece occurs. The Infant Flow (IF) system provides NCPAP by means of a special nose piece using the ‘fluidic flip’ technology, which is based on the Coanda effect; it directs airflow to the infant’s airways during inspiration and away from the nares into the expiratory part of the system during expiration.8–11 This latter concept is used by the Fabian neonatal ventilator in its IF mode (Acutronic Medical Systems AG, Hirzel, Switzerland). The SERVO-i ventilator (Maquet Critical Care, Solna, Sweden) allows for rapid adjustments in the flow rate via the inspiratory valve of the ventilator. Physical modelling5 8 10 and clinical studies12 13 have found that, compared with constant-flow devices, variable-flow devices provide less airway pressure variability and less imposed work of breathing (iWOB). The aim of this study was to identify the potential impact on patient inspiratory effort by three different types of modern variable-flow NCPAP devices, as estimated by the amplitude of the electrical diaphragmatic signal.
Methods
Population
The preterm infants were recruited from the neonatal intensive care unit at University Hospital of Geneva, Switzerland. All parents of eligible preterm infants were approached (if a member of the research team was available to do so). Twenty preterm infants weighing ≤2500 g requiring NCPAP for mild respiratory distress (defined by a respiratory rate of >80 cycles/min; signs of respiratory effort, such as chest retraction; and FiO2 requirement of 25%–40%), but otherwise medically stable, were included in the study after obtaining parents’ consent. Infants were excluded if they had pneumothorax, degenerative neuromuscular disease, bleeding disorders, cardiovascular instability, cyanotic congenital cardiovascular disease, phrenic nerve damage/diaphragm paralysis or oesophageal perforation. Infants deemed ‘too unstable’ by the attending physician in charge were also excluded.
NCPAP devices
The following NCPAP devices were compared:
MedinCNO, with the Medijet interface and the nasal prongs from Medin (Medin Medical Innovations) and the leakage compensation algorithm on.
Fabian ventilator (Acutronic Medical Systems AG), with the IF interface (nasal prongs) and circuit tubing (CareFusion, San Diego, California, USA)
Servo-i ventilator (Maquet Critical Care), with the Miniflow interface and the nasal prongs from Medin (Medin Medical Innovations).
Intervention protocol
The study applied a cross-over design. The patient’s nasogastric feeding tube was replaced by a specific nasogastric feeding tube with miniaturised electrodes (size 6F NAVA catheter, Maquet, Solna, Sweden) to record the electrical activity of the diaphragm (EAdi), positioned according to the manufacturer’s guidelines. All children were placed in supine position. Patients were supported with each of the three devices for 20 min consecutively. The sequence of NCPAP devices was randomly assigned. Before and during the study, the NCPAP level was kept constant. The lowest FiO2 possible was delivered while maintaining an oxygen saturation measured by pulse oximetry (SpO2) of >92%. Vital parameters (respiratory rate and heart beat) were continuously monitored. SpO2 (Oximax NN; Coviden, Elancourt, France) and transcutaneous pCO2 (TcPCO2) (Tina TCM 4/40; Radiometer Medical ApS, Brønshøj, Denmark) were also measured. The EAdi signal was recorded at a sampling rate of 50 Hz and stored (Polybench, Inbiolab, Groningen, the Netherlands). After the study period, each patient was returned back to the device with the same setting used before the study.
Data recording and statistical analysis
Primary outcome was an estimate inspiratory effort, represented by the sum ∆EAdi/s for each breath for 30 consecutive breaths. Two randomly chosen minutes among the last 10 min of each recording were used. Thirty breaths per recording were subsequently analysed. We report the sum of ∆EAdi (ie, the difference between the tonic and the phasic activity for each breath) for 30 breaths. Given the physiological irregular breathing patterns of preterm infants, and in an effort to correct for rapidly changing breathing frequencies and amplitudes, the ratio between the sum of ∆EAdi and the duration of the consecutive 30 breaths (sum ∆EAdi/s) was also calculated. Recorded EAdi signals were analysed using the AcqKnowledge software V.3.7.3 (Biopac Systems, Goleta, California, USA). Data were summarised as frequencies and percentages for categorical variables and as median with IQR (25th–75th percentile) or mean and SD for continuous variables as appropriate. Associations between ∆EAdi, ∆EAdi/s, vital parameters (respiratory rate, heart rate, SpO2 and TcPCO2) and NCPAP devices were tested using Mann-Whitney or Kruskal-Wallis test as appropriate. A linear regression model with mixed effects was used to evaluate the presence of a potential sequence effect. All statistical tests were two-sided and the significance level was 0.05. Analysis were performed using R statistical software V.3.5.0 (the R Foundation for Statistical Computing).
Results
Twenty preterm infants weighing <2500 g and requiring NCPAP for mild respiratory distress between June 2015 and August 2016 participated in the study. Demographic characteristics of the study population are presented in table 1. No significant changes in vital parameters were noted among the three devices as shown in table 2. ∆EAdi (mean and SD) for 30 consecutive breaths were 262 (±119) µV for CNO, 352 (±262) µV for IF and 286 (±126) µV for SERVO-i (p=0.7). ∆EAdi/s were 6.1 (±2.3) µV/s for CNO, 7.9 (±4.9) µV/s for IF and 7.6 (±3.6) µV/s for SERVO-i, respectively (p=0.39) (shown in figure 1 and table 3). No NCPAP device sequence effect was detected (p=0.51).
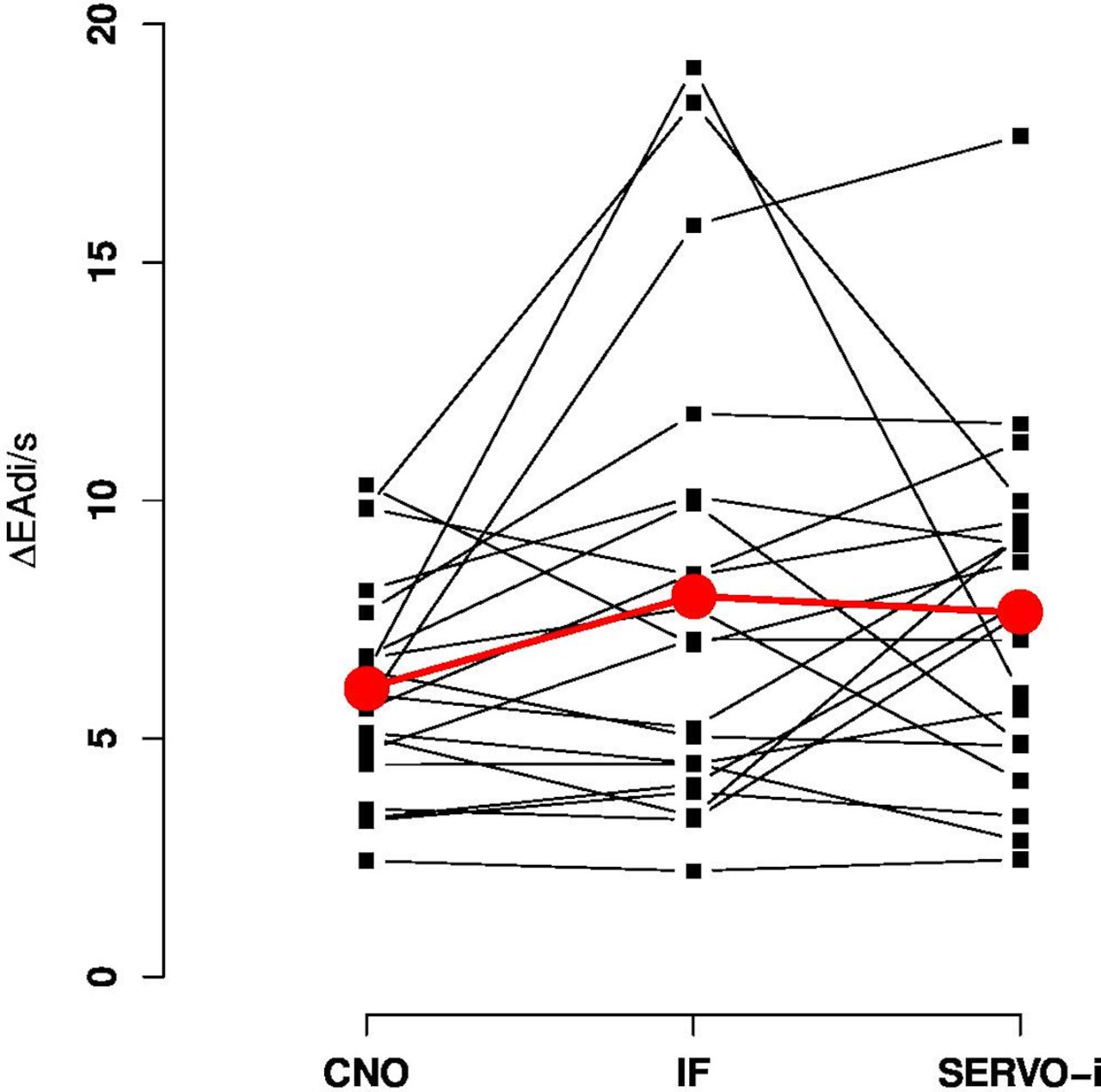
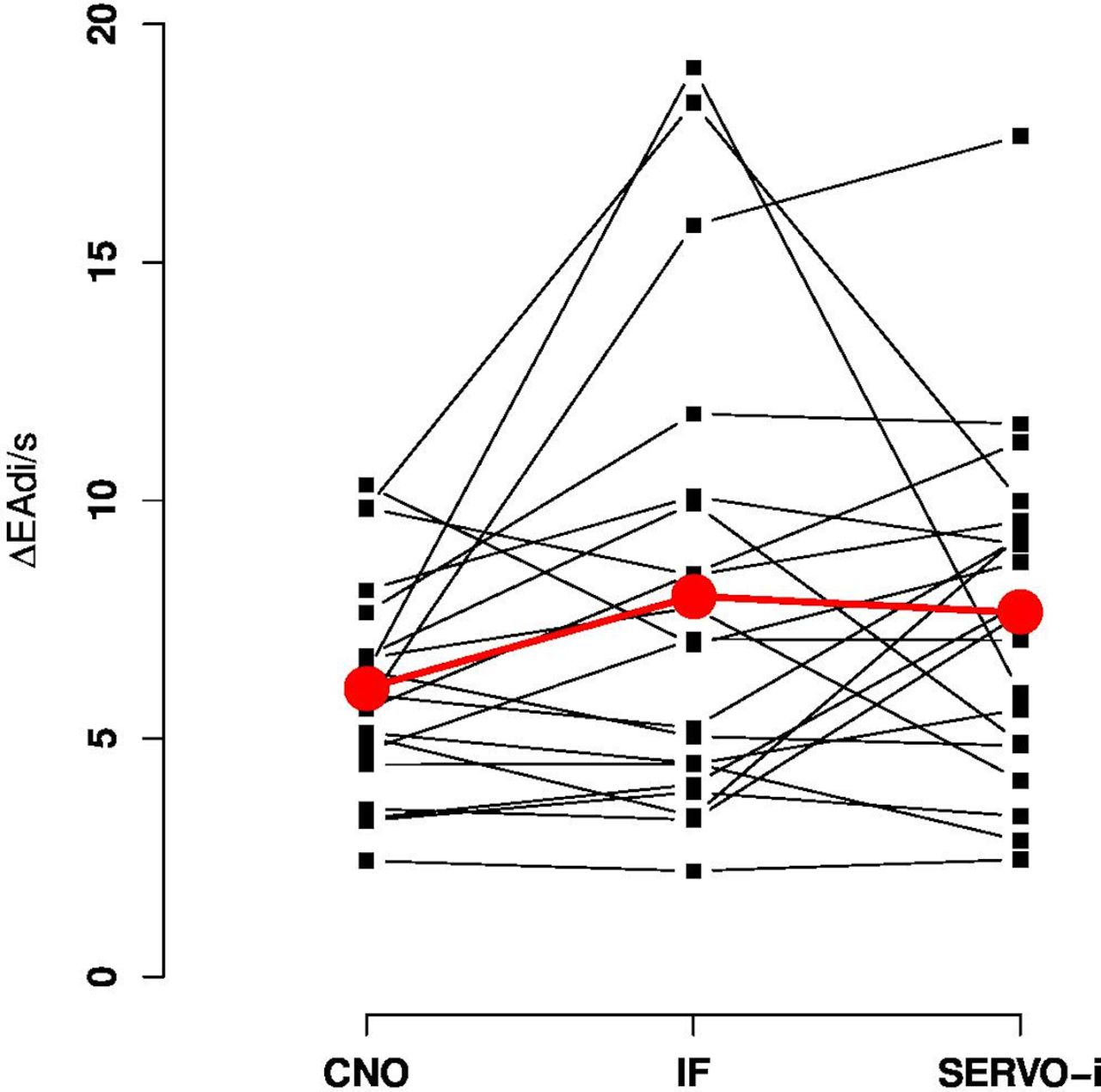{kind=link}
Graphical representation of the sum ∆EAdi/s for each ventilator. Black squares represent individual data and red points the mean. The sum ∆EAdi/s for the three CPAPs and for the same patient are joined by a black line. CPAP, continuous positive airway pressure; EAdi, electrical activity of the diaphragm, IF, Infant Flow.
Demographics characteristics of the study population (n=20)
Vital parameters during CNO, IF and SERVO-i
Sum of ∆EAdi/s for CNO, IF, SERVO-i for 30 breaths
Discussion
Our study shows that the three variable-flow NCPAP devices (Servo-i, Fabian and MedinCNO) did not significantly change the estimate of inspiratory effort, as measured by variations in the EAdi signal and vital parameters, in preterm infants with mild respiratory distress. Drevhammar et al 14 suggested in a bench test that the Fabian ventilator in the IF NCPAP mode and the SERVO-i in its NCPAP mode both resulted in better pressure stability compared with other tested devices. In contrast to our study, another bench study from the same group15 confirmed the superiority of the IF system (as used by the Fabian ventilator) on pressure stability and iWOB compared with the Medijet system. The CNO and Medijet are produced by the same manufacturer and share the same functionality and interface. Nonetheless, the more recent CNO device is equipped with a leak compensation algorithm, and we could argue that the leak compensation algorithm in the CNO device might have improved its pressure stability and therefore inspiratory effort compared with the Medijet. We could hypothesise that the lack of a significant difference of the estimate of the inspiratory effort among the three tested devices in our study is related to the presence of a leak compensation algorithm in the newer device by Medin, that is, the CNO device.
Our results showing no relevant clinical differences between various variable-flow NCPAP systems are consistent with a previous study from Courtney et al.16 These authors could not find any difference in work of breathing when comparing two variable-flow CPAP devices: Infant Flow (EME) and Arabella1 (by Hamilton Medical).
This study has some limitations. First, our population was represented by 4-week-old premature infants who were already on NCPAP before the study. Our results might therefore not be applicable to preterm infants immediately after birth when respiratory distress syndrome is usually more pronounced. Nonetheless, we chose not to test the devices soon after birth as it would be in contrast with minimal handling practice of severely ill preterm infants during the first hours of life. Second, the lack of a significant difference in inspiratory effort does not automatically translate into equivalent short-term or long-term clinical outcomes. Third, a new version of the Getinge ventilator, the Servo-n, is now available in the market. This ventilator is specifically designed for neonatal and paediatric patients. The only difference between the ventilator that has been tested in our study (Servo-i Universal V.7.0 in the paediatric/neonatal mode) and the new Servo-n is maximum flow for leak compensation, that is, 15 L/min vs 20 L/min, respectively. We believe that this small modification could not significantly impact our results. Moreover, the MedinCNO and the Fabian in its IF mode are characterised by a much smaller maximal flow for leak compensation. To the best of our knowledge, those ventilators have not been modified in the meantime. Lastly, the gold standard measure for inspiratory effort is oesophageal pressure measured by means of a balloon catheter.17 However, reliable and reproducible oesophageal pressure measures are very difficult to obtain regardless of the method used, especially in children.18 Nevertheless, ∆EAdi seems to be highly correlated to oesophageal pressure changes in critically ill children and can therefore be used as a surrogate measure of the inspiratory effort.19
Conclusion
Our study shows that the mechanism of airway-pressure generation of three distinct latest-generation variable-flow NCPAP devices have no significant impact on a preterm infant’s inspiratory effort or vital parameters. Future studies are warranted to confirm our findings in preterm infants soon after birth and to explore the potential association between inspiratory effort during NCAP therapy and clinical outcomes.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Ethics approval
The protocol was approved by the ethics committee of the University Hospital of Geneva (number 14–171). Informed parental consent was obtained prior to enrolling the preterm infants into the study.
Footnotes
Contributors Literature search: AB. Study design: PCR and AB. Data collection: AB, AM and CFC. Data analysis and interpretation: AB, PCR, AM, CFC, AP and CC. Manuscript preparation: AB. Review of manuscript: AB, AM, CFC, CC, AP and PCR. Final approval of the version to be published was approved by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.