Article Text

Abstract
Objectives To determine the incidence of and risk factors for neonatal unit admission, intrapartum stillbirth or neonatal death without admission, and describe outcomes, in babies born in an alongside midwifery unit (AMU).
Design National population-based case-control study.
Method We used the UK Midwifery Study System to identify and collect data about 1041 women who gave birth in AMUs, March 2017 to February 2018, whose babies were admitted to a neonatal unit or died (cases) and 1984 controls from the same AMUs. We used multivariable logistic regression, generating adjusted OR (aOR) with 95% CIs, to investigate maternal and intrapartum factors associated with neonatal admission or mortality.
Results The incidence of neonatal admission or mortality following birth in an AMU was 1.2%, comprising neonatal admission (1.2%) and mortality (0.01%). White ‘other’ ethnicity (aOR=1.28; 95% CI=1.01 to 1.63); nulliparity (aOR=2.09; 95% CI=1.78 to 2.45); ≥2 previous pregnancies ≥24 weeks’ gestation (aOR=1.38; 95% CI=1.10 to 1.74); male sex (aOR=1.46; 95% CI=1.23 to 1.75); maternal pregnancy problem (aOR=1.40; 95% CI=1.03 to 1.90); prolonged (aOR=1.42; 95% CI=1.01 to 2.01) or unrecorded (aOR=1.38; 95% CI=1.05 to 1.81) second stage duration; opiate use (aOR=1.31; 95% CI=1.02 to 1.68); shoulder dystocia (aOR=5.06; 95% CI=3.00 to 8.52); birth weight <2500 g (aOR=4.12; 95% CI=1.97 to 8.60), 4000–4999 g (aOR=1.64; 95% CI=1.25 to 2.14) and ≥4500 g (aOR=2.10; 95% CI=1.17 to 3.76), were independently associated with neonatal admission or mortality. Among babies admitted (n=1038), 18% received intensive care. Nine babies died, six following neonatal admission. Sepsis (52%) and respiratory distress (42%) were the most common discharge diagnoses.
Conclusions The results of this study are in line with other evidence on risk factors for neonatal admission, and reassuring in terms of the quality and safety of care in AMUs.
- epidemiology
- neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
National guidance recommends that women at low risk of complications should have a choice of planned birth setting.
For low-risk women planned midwifery unit birth is as safe for babies and associated with reduced intervention, compared with planned hospital obstetric unit birth.
Neonatal admission following birth in a midwifery unit, where most women are low risk, not induced and give birth vaginally, is a potential ‘near-miss’ event.
What this study adds?
Around 1% of babies born in the UK alongside midwifery units are admitted to neonatal care, are stillborn or die soon after birth without admission.
Few babies had diagnoses or outcomes indicative of serious intrapartum-related adverse outcome.
Risk factors for neonatal admission or mortality identified in our study are known risk factors for adverse neonatal outcome in term infants in other settings.
Introduction
Most babies in high-income countries are born in hospital obstetric units (OU),1 2 but in the UK around 15% of births take place in midwifery-led settings.3 4 Around 80% of these are in alongside midwifery units (AMU), on the same site as an OU. For women at low risk of complications, planned birth in an AMU is associated with less intervention,5 including a 60% reduction in the likelihood of caesarean section, with no difference in neonatal outcomes, compared with planned birth in an OU.6 Most women planning birth in AMUs are at low risk, but around 4% have pre-existing risk factors6 7; many AMUs now explicitly admit women with selected risk factors.8 ,9
National guidance recommends transfer to an OU when complications occur during labour in a midwifery-led setting.10 However, around 40% of adverse perinatal outcomes in births planned in midwifery-led settings occur in births in the planned setting, that is, when no transfer took place.6 Most babies admitted to neonatal care are born in OUs. Neonatal admission, or death without admission, following birth in an AMU, where most women are at low risk of complications, labour spontaneously and give birth vaginally, is a potential indicator of a ‘near-miss’ or adverse outcome event where different management might have made a difference to outcome. Factors associated with term admission and reasons for admission are well-documented,11–15 but there is no evidence about admission following birth in a midwifery-led setting. This study aimed to: (i) determine the incidence of and risk factors for admission to neonatal care, intrapartum stillbirth or neonatal death without admission, in babies born in an AMU and (ii) describe reasons for neonatal admission.
Methods
Study design
We carried out a national, population-based, case-control study.
Cases and controls
We identified and collected data about women who gave birth in an AMU in the UK between 1 March 2017 and 28 February 2018, and whose baby was admitted to a neonatal unit, for at least 4 hours, within 48 hours of birth or before discharge home or who was stillborn or died within 48 hours of birth without admission to neonatal care (cases). We refer to this outcome as ‘neonatal admission or mortality’. Controls were the two women not meeting the case definition who gave birth in the same AMU immediately before each case.
Data collection
We collected data using the UK Midwifery Study System (UKMidSS), a national research infrastructure covering all 123 AMUs in all four countries of the UK. UKMidSS midwife ‘reporters’ in each AMU reported cases, and the number of AMU births, in response to monthly emails, and entered anonymised data directly from medical records using study-specific forms in a secure web-based environment.16
We compared the number of deaths reported for this study with those reported to national perinatal surveillance (MBRRACE-UK)17 in AMU births over the same period. Where this identified potentially ‘missing’ deaths, not reported to UKMidSS, we contacted UKMidSS and MBRRACE-UK reporters in the relevant units to cross-check using MBRRACE-UK and UKMidSS ID numbers (no identifiers were disclosed). Where a previously unreported case was identified, data were collected as described above.
Data
We considered maternal sociodemographic factors; pre-existing clinical characteristics and those arising during pregnancy and intrapartum and birth-related factors, as potential explanatory variables (online supplementary table S1) and collected the neonatal outcomes listed in online supplementary table S2.
Supplemental material
Analysis
We estimated the incidence of neonatal admission or mortality (combined and separately) using the total reported births as the denominator, with 95% CIs.
We described characteristics of cases and controls, and neonatal outcomes for cases. We used unconditional logistic regression to investigate univariable associations between explanatory variables and the primary outcome, and built a multivariable model, calculating unadjusted OR and adjusted OR (aOR) with 95% CI. Conditional logistic regression was not used since cases and controls were ‘convenience matched’ on the basis of time of birth only.18 We used a prespecified conceptual framework approach to multivariable model building, adding variables to the model in stages from distal to proximal (maternal and pre-existing clinical characteristics first, followed by maternal clinical characteristics arising during pregnancy, maternal intrapartum factors and finally, birth-related factors). Variables were considered for inclusion in the model if p<0.05 in the univariable analysis, or if univariable analyses indicated that their association with the outcome was confounded by another variable. The contribution of each variable to the fit of the data to the model was tested for significance using the Wald test, and variables for which p<0.05 were retained in the model. We used robust variance estimation to allow for the clustering of women within units.
In a post hoc analysis, we compared the highest level of care received and reasons for admission in centres where the number of cases reported or the incidence of admission was at or above the 95th centile, with other centres, using the χ2 test.
Our approach to handling missing data, and sample size and power calculations are presented in online supplementary box S1.
We used Stata V.15SE for all analyses.19
Results
Response and incidence
All 123 AMUs in the UK participated (100% of eligible units), with a 99.8% response to monthly report requests.
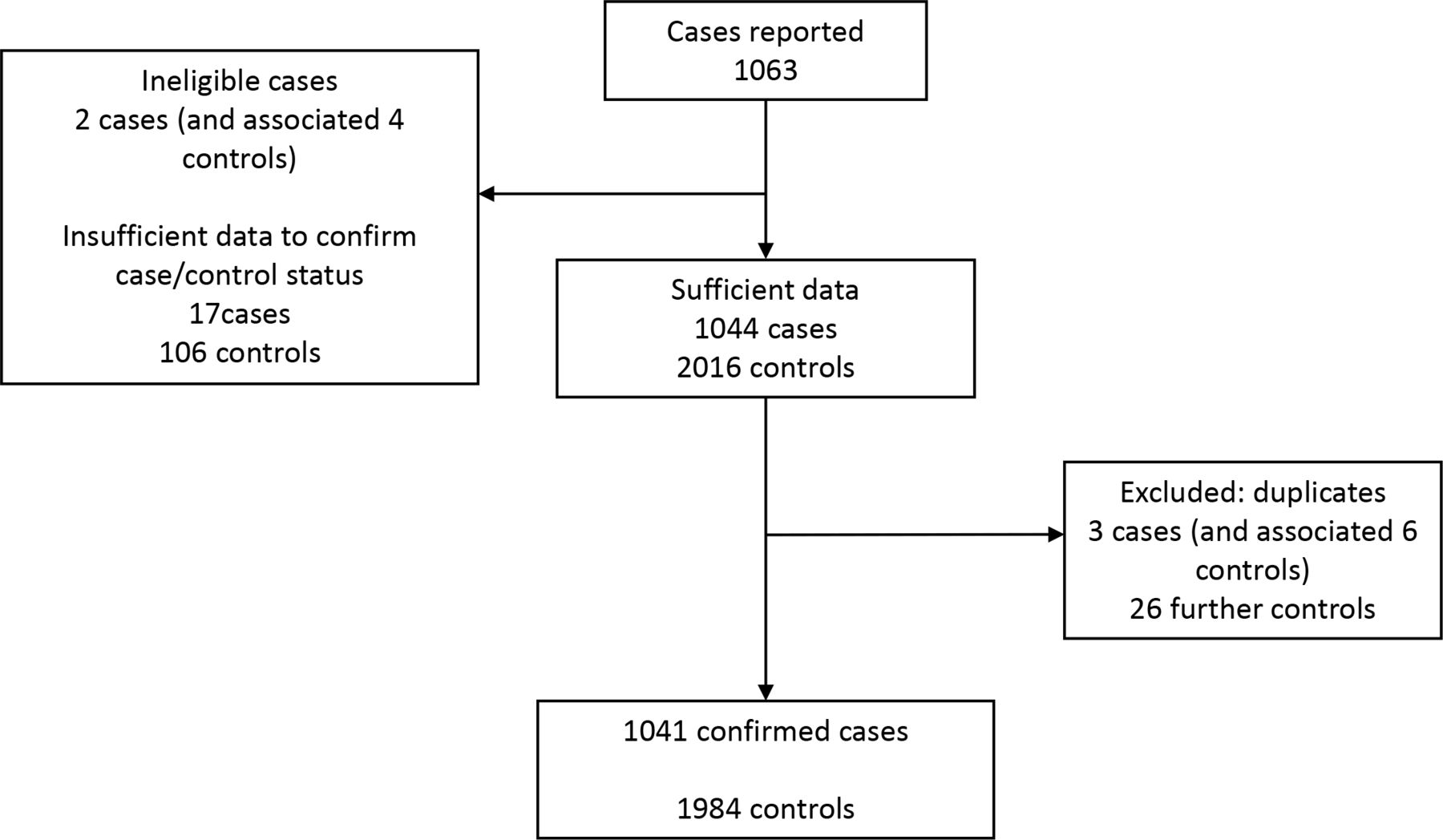
In total, 1063 cases were reported (figure 1). There were 1041 confirmed cases, and 1984 controls, from a total of 87 102 women giving birth in AMUs. Among the 1041 cases, two women had an intrapartum stillbirth and one woman’s baby died after birth without admission to neonatal care. Six of the 1038 surviving babies admitted to neonatal care subsequently died. The incidence of neonatal admission or mortality following birth in an AMU was 1.2% (95% CI 1.1 to 1.3), comprising neonatal admission (1.2%) and mortality (0.01%).
{kind=link}
Reported and confirmed cases and controls with reasons for exclusion.
Overall, 110 out of 123 (85.4%) AMUs in the UK reported at least one confirmed case during the study period. The incidence of neonatal admission or mortality in each AMU ranged from 0% to 4.2% (median 1.0%; IQR 0.5%–1.6%).
Univariable analysis
Among sociodemographic and pre-existing clinical characteristics of women, ethnicity, parity and previous pregnancy problems were statistically significantly associated with neonatal admission or mortality (table 1). Clinical characteristics arising during pregnancy that were statistically significantly associated with neonatal admission or mortality were: current pregnancy fetal problem and sex of the baby (table 1). Details of medical risk factors, and pregnancy problems are shown in online supplemental tables S3 and S4.
Sociodemographic, pre-existing and pregnancy-related clinical characteristics of women
Labour-related factors significantly associated with neonatal admission or mortality were: fetal complication at the start of labour care, stage of labour at admission, prolonged second stage of labour, immersion in water, opiates for pain relief, fetal heart rate concerns or other fetal complications identified during labour and consulting an obstetrician for fetal compromise (table 2). Details of complications are shown in online supplemental tables S5–S7. All four birth-related factors: shoulder dystocia, birth weight, birth in water and mode of birth were statistically significantly associated with neonatal admission or mortality (table 2).
Labour and birth-related factors
Multivariable analysis: factors associated with neonatal admission or mortality
Multivariable analysis identified white ‘other’ ethnicity; nulliparity; two or more previous pregnancies ≥24 weeks’ gestation; male sex; maternal current pregnancy problem (most common group B streptococcus (GBS) and body mass index (BMI)) >35 kg/m2, see online supplemental table S2); prolonged or unrecorded duration of second stage of labour; opiates during labour; shoulder dystocia and birth weight <2500 g, 4000–4999 g and ≥4500 g, as independently associated with neonatal admission or mortality (table 3).
Factors associated with neonatal admission or mortality
Neonatal outcomes
Around three-quarters (78%) of the cases admitted to neonatal care were admitted from the birth room, rather than from the postnatal ward (table 4). Less than half (43%) received any neonatal resuscitation and in around 80% of those this comprised stimulation/positioning, inflation breaths and oxygen/ventilation breaths only. Among cases who were resuscitated, 17% were intubated and 2% received neonatal resuscitation drugs. Around one in five cases (18%) who were admitted to neonatal care received intensive care. The most common reasons for admission were respiratory problems and suspected infection, and this was reflected in diagnoses on discharge.
Neonatal outcomes
Centres with high numbers of cases
Compared with other centres, in centres with more cases or higher incidence, a higher proportion of babies received special care as the highest level of neonatal care (64% vs 48%, p<0.001), fewer babies were admitted because of respiratory problems (60% vs 73%, p<0.0001) and more babies were admitted with suspected infection (52% vs 40%, p=0.001) (online supplemental table S8).
Discussion
Around 1% of babies born in UK AMUs during the study period were admitted to neonatal care, stillborn or died within 48 hours of birth without admission. Less than half of the babies admitted to neonatal care required resuscitation and in around 80% of those this comprised stimulation/positioning, inflation breaths and oxygen/ventilation breaths only. The most common reasons for admission were respiratory problems and suspected infection; this was reflected in discharge diagnoses. We found significant variation between units in rates and reasons for admission.
National statistics show that the overall incidence of neonatal admission in term babies is around 6%1 and the incidence of intrapartum-related stillbirth or neonatal death at term is 0.28 per 1000 total births.20 The lower incidence of these outcomes found in our study reflects the predominantly ‘low risk’ characteristics of the study population.
Babies of women with identified maternal pregnancy complications were 1.4 times more likely to be admitted to neonatal care. In line with other evidence,7 the most common of these complications were GBS colonisation and BMI >35 kg/m2. National guidance advises that women with a BMI >35 kg/m2, and those with GBS for whom antibiotics in labour would be recommended, should be advised to plan birth in an OU rather than a midwifery-led setting, the latter group so they can receive intrapartum antibiotic prophylaxis.10 21 Almost half of UK midwifery units now report admitting women who require antibiotics for GBS9 and admission of women with a BMI >35 kg/m2 is also widespread.8 ‘Higher risk’ women in AMUs are more likely to be transferred before birth than women at ‘low risk’ of complications, but around 70% of ‘higher risk’ women admitted to AMUs give birth there without transfer.7 Planned birth in an AMU is associated with a significant reduction in the likelihood of having a Caesarean section compared with planned OU birth,6 and there is evidence of good outcomes for women with higher BMI in AMUs.8 Individual care plans are recommended for women at ‘higher risk’ of complications who plan to give birth outside an OU.10
Even in term appropriately grown babies, boys are more likely than girls to have lower Apgar scores, need neonatal resuscitation, develop respiratory problems and be admitted for neonatal care.22 Our finding, that boys were almost 1.5 times more likely than girls to be admitted for neonatal care, in a population in which 99% of women had a spontaneous vaginal birth, suggest that these differences are not explained by an increased risk of instrumental or operative birth,22 and are independent of birth weight.
Evidence about the duration of labour and neonatal outcomes is mixed,23 but recent studies point to an increased risk of adverse neonatal outcomes with prolonged second stage of labour.15 24 25 We found that the likelihood of neonatal admission or mortality was 1.4 times higher when the second stage of labour was ‘possibly prolonged’.10 Given available data it was not possible to determine why these women were not transferred to an OU, as national guidance recommends, nor whether the outcome for the baby would have been different had transfer taken place. For some women, for example, free text comments indicated that when concerns were identified late in labour an obstetrician attended the AMU to expedite birth, in preference to transfer, but available data did not permit further investigation. This might also explain at least some of the 31 instrumental births in an AMU in our study. Free text comments also indicated that, for some women, fetal concerns such as significant meconium and fetal heart decelerations were only identified in advanced labour or close to the time of birth. This might explain why these woman were not transferred, as recommended by national guidance,10 however the extent to which this also explained the lack of consultation with an obstetrician, seen in several cases, was not clear.
Opioids are widely used for pain relief in labour,26 but are associated with neonatal respiratory depression.27 28 In line with other studies,15 29 we found that the likelihood of neonatal admission or mortality was 1.3 times higher in babies of women who used opioids for pain relief in labour.
Our study confirms low (<2500 g) and high (>4000 g) birth weight as independent risk factors for adverse neonatal outcome.29–32 Fetal macrosomia is a risk factor for shoulder dystocia.33 34 Almost half of the cases with shoulder dystocia in our study had a birth weight >4000 g, but shoulder dystocia was associated with a fivefold increase in the likelihood of neonatal admission after adjusting for birth weight. Shoulder dystocia is a risk factor for birth trauma injuries,35 but in our study only a small proportion of the babies with documented shoulder dystocia had a discharge diagnosis of birth injury.
Finally, there are national initiatives aimed at reducing unnecessary neonatal admissions, avoiding separation of mother and baby, and standardising admission criteria,13 36 and some evidence that the provision of transitional care is increasing.4 Our study provides further evidence of variation in local neonatal unit admission policies,14 with significant variation between units in admission rates and reasons for admission.
This was a national population-based study, which reduces the risk of bias associated with local, hospital-based studies. All eligible units participated, with over 99% response to monthly report requests and complete data returned for over 95% of reported cases, reducing the possibility of selection bias. There are nevertheless some potential limitations. We aimed to identify all women whose baby was admitted to neonatal care or who died following birth in an AMU. We checked against deaths reported to MBRRACE-UK, so are confident that we are unlikely to have missed deaths, but had no other sources of data against which to validate other reported cases, so it is possible that we may have missed some admissions. We were dependent on anonymised routine data from medical records so did not have data on a number of factors of interest, including, for example, staffing levels, time of day, day of the week or whether there was an agreed plan for care of the woman in an AMU in the presence of risk factors.
Conclusions
The results of this study are broadly reassuring and in line with existing evidence about the quality and safety of care in AMUs. Relatively few babies had diagnoses of suspected asphyxia or meconium aspiration, which might be indicative of serious intrapartum-related adverse outcome. Many of the factors we identified as associated with neonatal admission or mortality are known risk factors for adverse neonatal outcome in term infants in other settings. Midwives should continue to practice in line with national guidance in relation to the management of risk factors and emerging complications in women labouring in AMUs.
Acknowledgments
The authors would like to thank all the UKMidSS reporting midwives across the UK who responded to monthly report requests and entered data, and the MBRRACE-UK reporters who helped identify potentially ‘missing’ cases. The authors would also like to thank UKMidSS Research Midwives Paula Jenkins and Ginny Mounce for their contribution to managing data collection and supporting UKMidSS reporters.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @RachelRowe3, @Marianfknight
Collaborators The UKMidSS Steering Group (in addition to RR, AS, MK and JJK): Mervi Jokinen (Chair), Royal College of Midwives; Catherine Williams (Vice Chair), Lay member; Meena Bhatia (from June 2019), Oxford University Hospitals NHS Foundation Trust; Jan Butler (until December 2018), Cambridge University Hospitals NHS Foundation Trust; Philippa Cox (from February 2019), Homerton University Hospital NHS Foundation Trust; Abi Holmes, Cardiff & Vale University Health Board; Karen Joash (from June 2019), Imperial College Healthcare NHS Trust; Eddie Morris, Royal College of Obstetricians and Gynaecologists; Jackie O’ Neill (from February 2019), Northern Health and Social Care Trust; Dharmintra Pasupathy (until February 2020), Guy’s and St Thomas’ NHS Foundation Trust; Rachel Plachcinski, lay member; Jane Rogers, University Hospitals Southampton NHS Foundation Trust; Julia Sanders, Cardiff and Vale University Health Boards; Anna Temke (February–December 2019), South Tees Hospitals NHS Foundation Trust; Phyllis Winters (until June 2019), NHS Tayside.
Contributors RR conceived the study and developed the protocol with input from JJK and MK. RR managed data collection, wrote the analysis plan and carried out analysis with input from JJK, MK, AS and the UKMidSS Steering Group. RR drafted the manuscript with input from all authors. All authors were involved in interpretation of data, review and revision of the draft manuscript and approval of the final version.
Funding This paper presents independent research arising from a National Institute for Health Research (NIHR) Post Doctoral Fellowship awarded to Rachel Rowe (PDF-2014-07-006). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Competing interests RR, MK and JJK report grants from the National Institute for Health Research (NIHR) during the conduct of this study. AS has nothing to disclose.
Patient consent for publication Not required.
Ethics approval UKMidSS and this study received ethics approval from the National Research Ethics Service (NRES) Committee South West—Frenchay (REC ref. 15/SW/0166) in May 2015.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Requests for access to the dataset underlying our findings will be considered by the National Perinatal Epidemiology Unit Data Sharing Committee and should be address to the Director, Jennifer Kurinczuk, jenny.kurinczuk@npeu.ox.ac.uk in the first instance.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.