Article Text

Abstract
Objective There is a high incidence of preterm birth in low-income and middle-income countries where healthcare resources are often limited and may influence decision making. We aimed to explore the interplay between resource limitations and resuscitation practices for extremely preterm infants (EPIs) in neonatal intensive care units (NICUs) across the Philippines.
Methods We conducted a national survey of NICUs in the Philippines. Institutions were classified according to sector (private/public), region and level. Respondents were asked about unit capacity, availability of ventilators and surfactant, resuscitation practices and estimated survival rates for EPIs of different gestational ages.
Results Respondents from 103/228 hospitals completed the survey (response rate 45%). Public hospitals reported more commonly experiencing shortages of ventilators than private hospitals (85%vs23%, p<0.001). Surfactant was more likely to be available in city hospitals than regional/district hospitals (p<0.05) and in hospitals classified as Level III/IV than I/II (p<0.05). The financial capacity of parents was a major factor influencing treatment options. Survival rates for EPIs were estimated to be higher in private than public institutions. Resuscitation practice varied; active treatment was generally considered optional for EPIs from 25 weeks’ gestation and usually provided after 27–28 weeks’ gestation.
Conclusion Our survey revealed considerable disparities in NICU resource availability between different types of hospitals in the Philippines. Variation was observed between hospitals as to when resuscitation would be provided for EPIs. National guidelines may generate greater consistency of care yet would need to reflect the variable context for decisions in the Philippines.
- neonatology
- resuscitation
- intensive care
- paediatric practice
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Many professional organisations and societies have developed management guidelines to support clinicians facing decisions about offering or withholding resuscitation for extremely preterm infants. There are no available guidelines that provide specific advice to clinicians in low-income or middle-income country while incorporating considerations of resource constraints. Studies from these settings have shown significant variation in resuscitation practices between and within countries.
What this study adds?
This is the first study to assess both availability of neonatal intensive care unit resources and resuscitation practices of preterm infants across an entire low-income or middle-income country.
Introduction
In many countries, professional organisations have developed guidelines for the perinatal care of extremely preterm infants (EPIs), including when resuscitation should or should not be provided. Most existing guidelines indicate thresholds based on the infant’s gestational age (GA).1 2 A lower threshold marks the gestation before which treatment will not usually be provided. An upper threshold marks the point after which treatment is considered mandatory. Between these ages lies a ‘grey zone’, where active treatment may or may not be provided, and parents’ wishes are important.
Published guidelines stem from high-income countries or international bodies.3–5 However, the vast majority of preterm births globally occur in low-income and middle-income countries (LMICs), where resource limits can affect the provision of medical care.6–10 To our knowledge, there are no published national guidelines for clinicians resuscitating preterm infants in these settings. Several studies have examined practice in individual hospitals or regions in LMICs, indicating variation between and within countries in the GA and birth weight thresholds used for resuscitation.11–18
The aim of this study was to survey neonatologists across an LMIC about resuscitation decisions for EPIs. We aimed to assess whether resuscitation practices varied between sectors of the health system and to identify the influence of resource limitations.
The Philippines is an archipelagic country with a population of 105 million and a gross domestic product (GDP)/capita of US$2989.19 Worldwide, it ranks eighth highest in number of preterm births (350 000/year).6 20 The average neonatal mortality rate is estimated to be 14 per 1000 live births, though there is wide regional variation (it is lower in urban areas but >20/1000 live births in some provinces).21 22 As in many other LMICs, for both private and public facilities, parents are required to pay out of pocket for the care of their infant.23
Methods
Participants
Neonatologists working in neonatal intensive care units (NICU) in the Philippines were contacted through a database provided by the Philippine Pediatric Society. For each hospital, a single neonatologist was identified to respond on their institution’s behalf. In some cases, one clinician was asked to complete the survey more than once, on behalf of multiple hospitals, as they were the only neonatologists working at those institutions. Up to three reminder emails and a single text message were sent to non-responders.
Evaluation instrument
A 34-item SurveyMonkey questionnaire was developed. The survey was written and conducted in English, an official language of the Philippines.24 25 Participation was voluntary, and responses were anonymous. The survey was conducted between January and March 2018.
The survey was structured in three main parts. The first requested information on the characteristics of the hospital including numbers of overall and preterm births. The second focused on availability of resources including number of beds, mechanical ventilators and surfactant. The third requested information about hospital policies and practice relating to resuscitation of EPIs. Respondents were asked how often resuscitation would be provided for infants born at a given gestation.
Questions consisted of Likert scale responses, yes/no, multiple choices and open-ended questions. For questions asking the frequencies of particular occurrences, ‘never’ and ‘rarely’ responses were grouped into a single category, as were ‘often’ and ‘almost always’ in our analysis. Clinicians were also asked about factors influencing decision making.14
Lastly, the survey asked for sociodemographic information from respondents including level of experience, religion and level of religiosity.
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences (SPSS) v25.0.26 Bivariate analyses to assess association between categorical outcomes were performed using Fisher’s exact test. Mann-Whitney U and Kruskal-Wallis tests were used for assessing differences between continuous variables. We analysed separately survival estimates for Level III/IV hospitals, as these would have most experience of caring for EPIs.
We assessed the frequency by which each institution would initiate resuscitation for infants of a given GA. We performed a post hoc analysis using Fisher’s exact test to assess if responses differed between different types of institutions at either 23/24 weeks’ gestation or 27/28 weeks’ gestation.
Results
Participants
Of the 228 hospitals providing neonatal care in the Philippines, we received 103 responses, yielding an overall response rate of 45%. Responses were submitted by 83 different neonatologists (14 entered data for more than one hospital). Most responses were from city hospitals, and approximately two-thirds were from private hospitals (table 1). The majority of respondents (75%) had more than 10 years’ experience of working in NICU.
Hospital and respondent characteristics
Births and resource availability
Respondents from higher level hospitals reported a larger number of beds and ventilators (online supplementary appendix 1). Compared with private hospitals, public hospitals reported a significantly higher number of births and preterm births, a larger number of beds but a lower number of ventilators per 100 preterm births.
Supplemental material
Most hospitals reported experiences of limitations in available ventilators at least some of the time (table 2). While 32% of private hospitals reported being ‘often’ or ‘always’ at full capacity for ventilators, this was reported by 85% of public hospitals (p<0.001).
Frequency of resource limitations in newborn intensive care: mechanical ventilation and surfactant administration
Forty-one per cent of hospitals reported that surfactant for respiratory distress syndrome was available only if parents or a charity were able to pay for it. Surfactant was more likely to be ‘always’ available in higher level hospitals (p<0.05) and more often available in city hospitals than provincial/district hospitals (p<0.05).
The most common responses to ventilator shortages were for the family to rent a ventilator, to attempt hand-ventilation, or to transfer the infant to another facility (table 3). Most hospitals reported no specific limitations on which preterm infants receive surfactant. Of the hospitals that did report a limiting factor, most cited the family’s financial capacity.
Responses of hospitals to limitations in availability of mechanical ventilators or surfactant
Costs of care
The median reported costs to parents for different services are shown in online supplementary appendix 2. The costs of daily NICU care, ventilator rental and surfactant administration were significantly higher in private hospitals.
Supplemental material
Survival rates
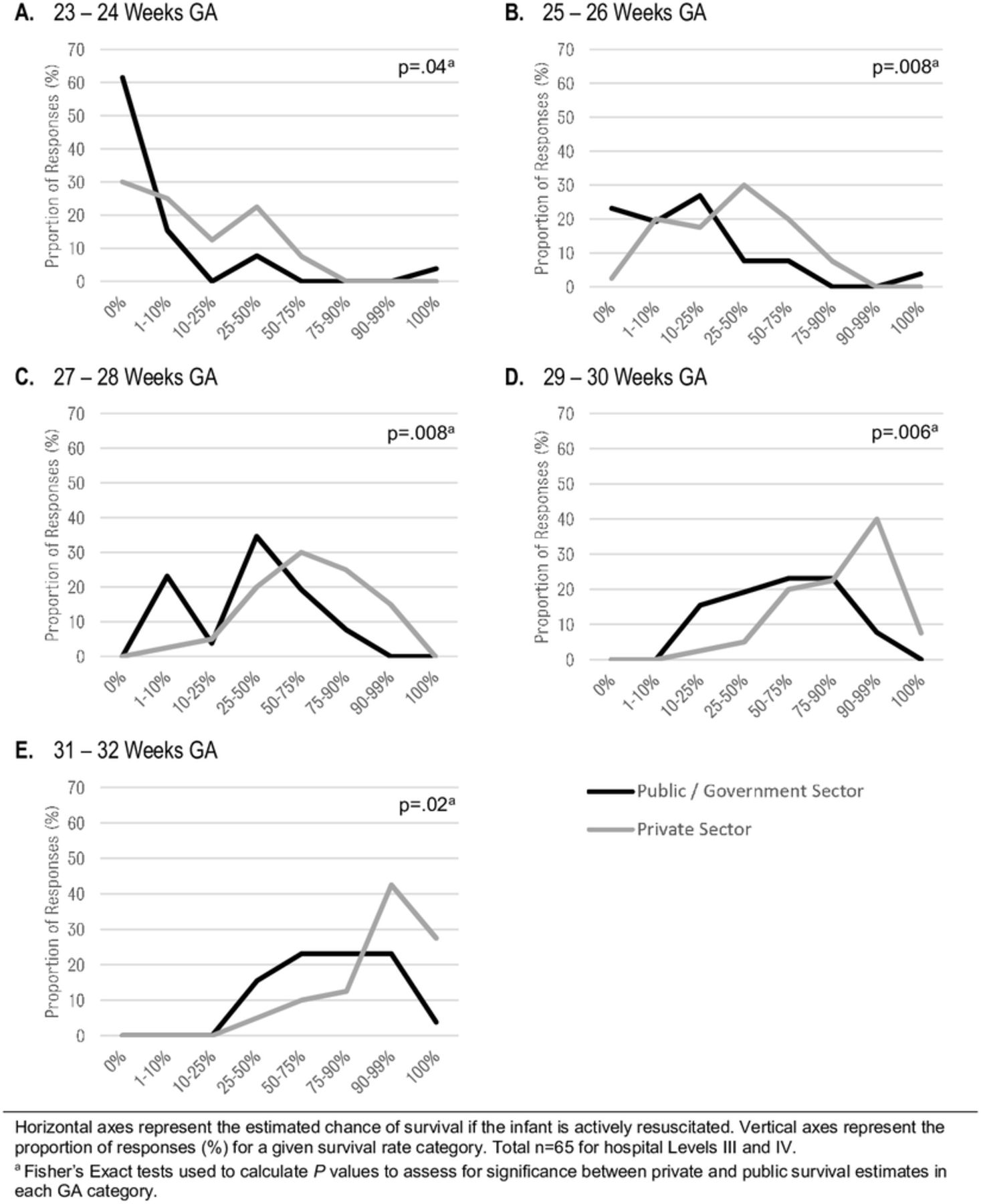
The estimated rate of survival for preterm infants increased with GA (figure 1), though there was wide variation in the estimates. Respondents consistently estimated higher survival rates for preterm infants cared for in private institutions than in public hospitals. City hospitals reported higher estimated survival than district/provincial hospitals at all gestations except at 23–24 weeks’ GA (online supplementary appendix 3).
Supplemental material
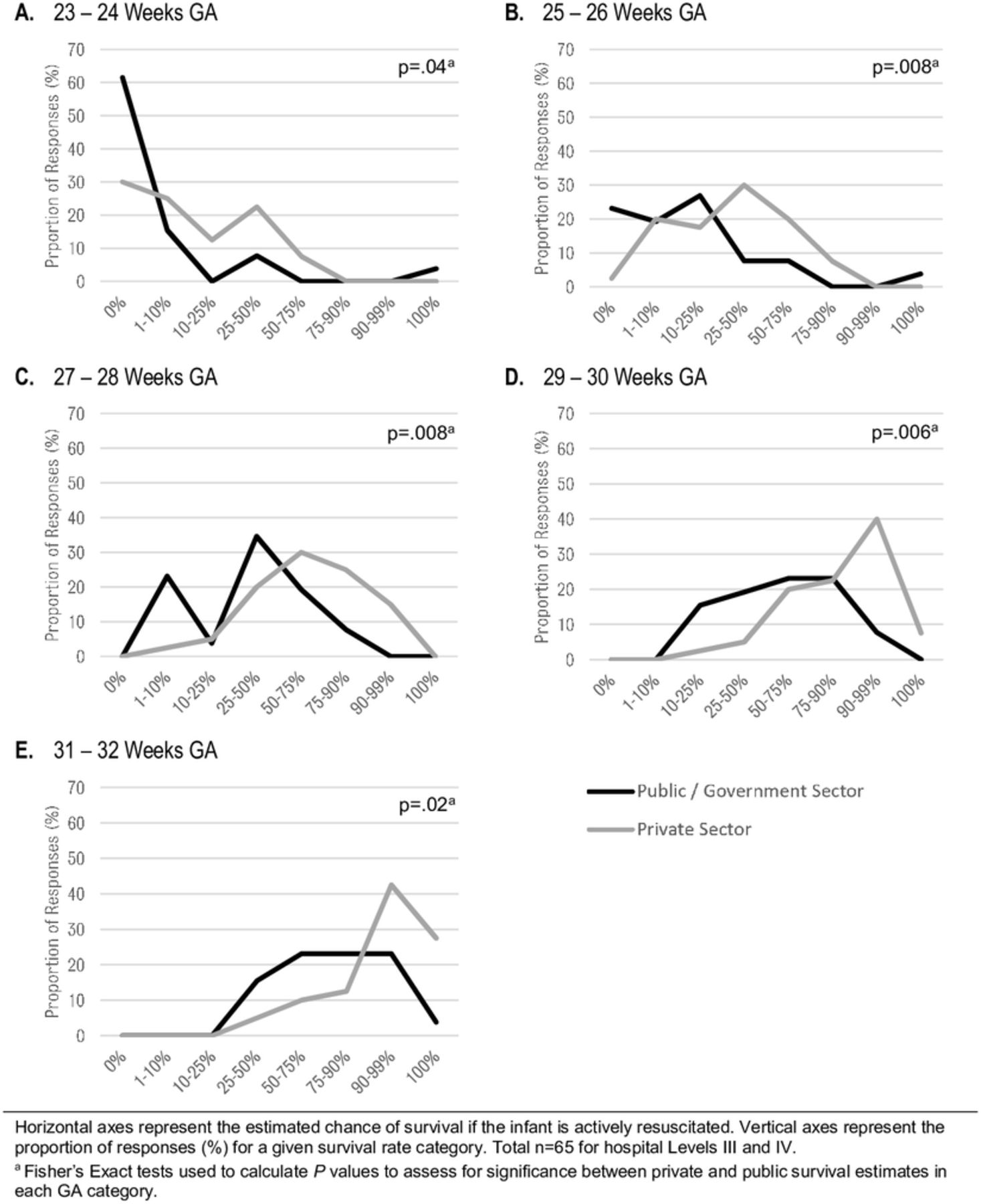
Estimated survival rates (if actively treated) at different GA categories in Level III and IV hospitals. GA, gestational age.
Initiating and limiting resuscitation for EPIs
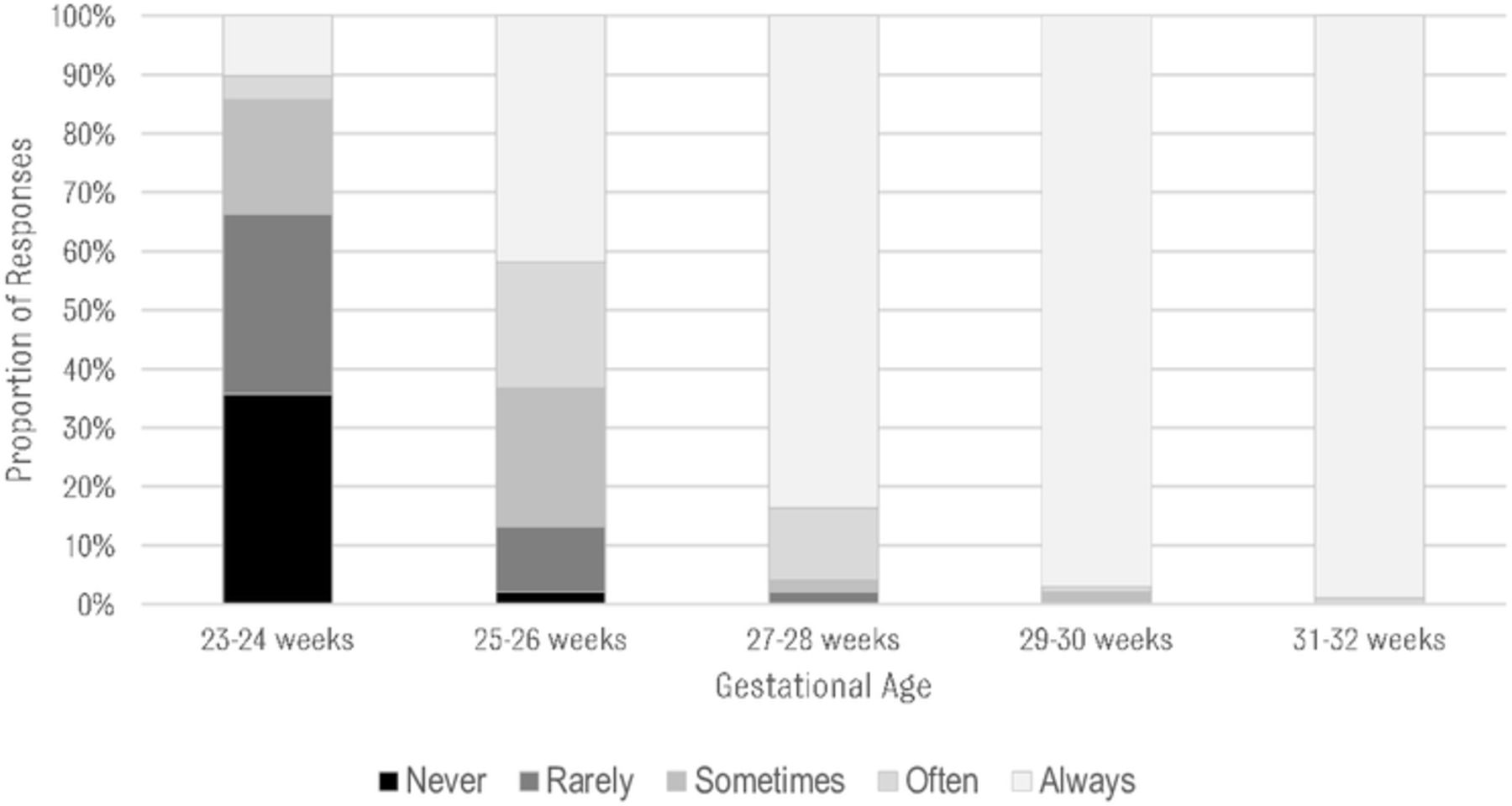
A majority of respondents reported using the American Academy of Pediatrics Neonatal Resuscitation Program (NRP) guidelines (online supplementary appendix 4).27 Fourteen hospitals reported using a local guideline developed by their department or institution. When asked about resuscitation at 23–24 weeks’ GA, 14% indicated that at their institution infants would ‘always’ or ‘often’ be resuscitated, while 66% indicated that resuscitation would ‘never’ or ‘rarely’ be initiated (figure 2). There was no significant difference between sectors, region or hospital level in the frequency of resuscitating at 23/24 weeks’ gestation (online supplementary appendix 5A). At 25–26 weeks’ gestation, 41% of hospitals would ‘always’ resuscitate, while 21% would ‘often’, and 23% would ‘sometimes’ resuscitate.
Supplemental material
Supplemental material
{kind=link}
{kind=link}
Frequency of initiating resuscitation for a given gestational age.
At 27–28 weeks’ GA, 84% of respondents indicated that they would always resuscitate (figure 2). The reported reasons for non-resuscitation in this group are listed in online supplementary appendix 5B.
Resuscitation was almost always provided at higher GAs (97% and 99% in the 29–30 and 31–32 weeks’ GA groups, respectively).
The most frequently cited reason influencing clinicians’ decision to limit resuscitation was ‘respecting parents’ wishes’ followed by ‘probability of infant death’ and ‘clinician’s morals’ (online supplementary appendix 6).
Supplemental material
Most respondents reported also using birth weight as a threshold for initiating resuscitation if the GA were uncertain (online supplementary appendix 7). The median birth weight threshold reported was 500 g (range of 400–800 g).
Supplemental material
No significant associations between willingness to offer resuscitation and participant characteristics were observed.
Discussion
To our knowledge, this is the first study to report the availability of NICU resources and resuscitation practice for EPIs across multiple hospital sectors in an LMIC. We found large disparities between hospitals across the Philippines in the availability of NICU resources. Furthermore, we found that the financial capacity of parents influenced treatment limitation decisions and played a major role in the response to resource limitations. Our study indicated that resuscitation would generally be considered from 25 weeks’ gestation in the Philippines and would usually be provided from 27 to 28 weeks’ gestation, though, in the absence of national guidance, there was large variation in when resuscitation or non-resuscitation would be considered. We did not observe disparities in resuscitation practices between different types of hospitals; however, our results suggested that outcomes for EPIs may differ between sectors; respondents provided higher survival estimates for EPIs in private versus public hospitals.
Resource limitations
The number of NICU ventilators per 100 preterm births (a metric we devised for assessing resource capacity) showed striking differences between the private and public sector. The reported differences in availability of neonatal beds, ventilators and surfactant were generally consistent with the intuitive assumption that large, private, urban centres would be better resourced than small, public, rural centres, respectively.
Hospitals reported wide-ranging courses of action taken in the face of resource limitations. When ventilators are at full capacity, the most commonly cited course of action was for the family to rent a ventilator, which may not be possible for poor families. It is possible that in such cases, hospitals resort to other cited responses such as hand ventilation, or attempt to identify a source of charitable funding for the family.28 Approximately one-third (35%) of respondents cited financial capacity of the family as a limiting factor in the provision of surfactant. The reported cost of a single dose of surfactant represents approximately 9% of the average per capita annual income in the Philippines.19 For some families, incurring the costs associated with extreme prematurity may lead to financial catastrophe.
Previous studies in other LMICs have documented the financial capacity of parents as a limiting factor in resuscitation of their preterm infant. Qualitative studies from neonatal units in India have reported that families’ motivations for withdrawing treatment were often based on costs, and that clinicians would only resuscitate EPIs if the family was willing to pay the entire bill themselves.16 29
We found differing estimated survival rates between different hospital types. Rates were significantly lower in public hospitals compared with private hospitals for all GA bands (figure 1). Lower survival rates in public hospitals might relate to the different number and capacity of ventilators reported in our study (tables 2 and 3). Poorer outcomes might also relate to other factors, including staffing levels, experience, rates of nosocomial infection or overcrowding.25 30 It might also conceivably relate to different risk factors in women presenting to public institutions (eg, reduced antenatal care and fetal growth restriction relating to maternal malnutrition).31 32
Resuscitation
Our survey identified that there is no single widely adopted guideline in the Philippines for resuscitation of EPIs (online supplementary appendix 4). The most commonly cited guideline, reported by 54% of respondents, was a US guideline. The NRP 7th Edition identifies the grey zone for resuscitation between 22 and 24 weeks GA, and does not take into consideration constraints on resources.27 These guidelines may not be easily applicable to the Philippine context, and indeed, local practice seemed to differ from the NRP recommendations. In Philippine hospitals, resuscitation was generally considered to be an option from 25 weeks’ gestation.
Thresholds reported in several other LMICs resemble our findings. Resuscitation is generally only considered beyond 25 weeks GA in South Africa, Lebanon and Malaysia.12 14 17 In contrast, studies from elsewhere report thresholds at later GAs: 26 weeks in El Salvador, 28 weeks in India and 31 weeks in Mongolia.13 15 29
As expected, in the absence of national guidelines, we found significant variations between institutions. Particularly at lower GA (23–26 weeks), we found a striking degree of heterogeneity, with some centres reporting that they would never or rarely resuscitate, while others reported usually or always providing resuscitation. Practice appeared more consistent for infants on reaching the 29–30 weeks’ GA band. At 27–28 weeks, some centres cited parents’ inability to pay as a reason to withhold treatment, while others indicated that this was based on anticipated poor outcome.
The divergence of practice seen across institutions could be due to differences in resource capacity. However, we did not observe differences in the reported rate of resuscitation between the different hospital types.
The spectrum of approaches (resuscitation offered for some infants at 23 weeks and withheld for some infants at 28 weeks) may represent a wide grey zone in which resuscitation is provided predominantly according to parental wishes. Approximately 2/3 of respondents reported that ‘parents’ wishes’ and ‘financial cost (for family)’ often or always affected decisions to limit resuscitation (online supplementary appendix 6). This contrasts starkly with an earlier survey of clinicians in six Pacific countries. In that study, only 26% of clinicians in Malaysia and 1% of clinicians in Japan reported ‘financial cost (for family)’ to often or always affect decisions to limit resuscitation.14 Of concern, our study suggested a higher prevalence of litigation fear influencing resuscitation decisions (29%) compared with other Pacific rim countries.
Limitations
We had modest response rates, which may affect the generalisability of our results, though the proportion of private and public hospital respondents in our study was close to the nationwide ratio. We had a higher proportion of level III/IV hospitals than the nationwide distribution (approximately 25%), yet many level I/II hospitals lack newborn care services and were not invited to participate in our study.23
Each hospital’s response was restricted to the views of one neonatologist responding on its behalf. Respondents may have answered some questions according to their own practice, which in the absence of clear guidelines may differ from their colleagues. We relied on participant’s reporting of outcomes (ie, estimated survival rate), yet such recollections or impressions of outcomes may be inaccurate or biased. We were not able to verify the accuracy of such estimates due to a general lack of evidence on outcomes for EPIs in the Philippines.
Conclusion
Our study provides valuable insights into the challenges of neonatal care in an LMIC. Philippine paediatricians are endeavouring to provide the same level of care that is available in developed countries; however, resource scarcity and the costs of treatment appear to be critical to decisions in a way that they are not in more well-resourced health systems. National guidelines would potentially generate greater consistency of care for preterm infants. However, they would need to reflect the context of decision making in a LMIC. The Philippine Society of Newborn Medicine is currently in the process of developing a national consensus guideline.
One challenge in establishing guidelines is the need for locally relevant data on the outcomes of treatment. The short-term and long-term outcomes of infants resuscitated at different GAs and birth weights in the Philippines would be highly useful, yet such data are currently lacking.
Finally, the perceived difference in outcome for EPIs between private and public institutions and the large out-of-pocket costs for families (a problem likely shared with other LMICs), points to the need for ethical attention to the structure and extent of funding for children’s healthcare in the Philippines.
Supplemental material
References
Footnotes
Contributors DH designed the survey, collected and analysed data, drafted the initial manuscript and reviewed and revised the manuscript. MEV-U contributed to the design of the survey and helped to evaluate, revise and edit the manuscript. MKM assisted with the collection of data and helped to evaluate, revise and edit the manuscript. DW conceived of the study, supervised and coordinated the design of the study and helped to evaluate, revise and edit the manuscript.
Funding DW was supported for this work by a grant from the Wellcome trust WT106587/Z/14/Z.
Competing interests None declared.
Ethics approval This study was approved by the University of the Philippines Ethical Review Board (UPMREB2017-335-01) and the University of Oxford Research Ethics Committee (R51548/RE001).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data relevant to the study are included in the article or uploaded as supplementary information.
Patient consent for publication Not required.