Article Text

Abstract
Background Systemic corticosteroids as the frontline treatment of respiratory distress syndrome (RDS) in preterm infants are associated with adverse effects on growth and neurodevelopmental outcome, but the pulmonary administration of steroids may help prevent the development of bronchopulmonary dysplasia (BPD) without these side effects.
Objectives To evaluate the efficacy and safety of pulmonary application of corticosteroids in preterm infants with RDS.
Methods MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, ClinicalTrials.gov, the WHO’s International Clinical Trials Registry and grey literature were searched with no restriction on date and language of publication from inception to May 2016. Using a random-effect model, we pooled data from randomised controlled trials (RCTs) comparing inhaled or endotracheal corticosteroids with the standard of care, placebo or no other intervention in preterm infants with RDS.
Results We identified 873 potential citations and included 12 unique RCTs. Pulmonary corticosteroid therapy was associated with a significant reduction in the composite outcome of BPD or death (relative risk (RR) 0.85, 95% CI 0.76 to 0.96). Pulmonary application of corticosteroids significantly reduced the incidence of patent ductus arteriosus (PDA) (RR 0.82, 95% CI 0.74 to 0.92) and pneumonia (RR 0.57, 95% CI 0.35 to 0.92). There was no evidence of a significant difference regarding the risk of neurodevelopmental impairment or other side effects.
Conclusions Pulmonary administration of corticosteroids reduces the incidence of BPD or death, pneumonia, PDA without causing any major side effects in preterm infants with RDS.
- bronchopulmonary dysplasia
- corticosteroid
- preterm infants
- pulmonary application
- respiratory distress syndrome
Statistics from Altmetric.com
- bronchopulmonary dysplasia
- corticosteroid
- preterm infants
- pulmonary application
- respiratory distress syndrome
What is already known on this topic?
Several treatments have been evaluated to prevent bronchopulmonary dysplasia (BPD) in preterm infants with respiratory distress syndrome (RDS).
Systemic corticosteroids as the frontline treatment are associated with adverse effects on growth and neurodevelopmental outcome.
Pulmonary administration of steroids may help prevent the development of BPD without these side effects.
What does this study add?
Pulmonary administration of corticosteroids could significantly reduce the risk of bronchopulmonary dysplasia or death, pneumonia and patent ductus arteriosus.
No major side effects were found in preterm infants with RDS.
Introduction
Preterm birth, defined as childbirth occurring before completed 37 weeks gestational age (GA),1 is reported in 11.1% of all births; or almost 15 million births per year worldwide.2 Nearly 1 million deaths in 2015 were caused by preterm birth complications including respiratory distress syndrome (RDS).3 Eight to 35% of RDS survivors develop BPD, defined as oxygen dependency at 36 weeks postmenstrual age or 28 days postnatal age.4–9 BPD is a common complication in 50% of extremely preterm neonates and is caused by ongoing lung injury and simultaneous repair.10 11 Prenatal and postnatal infections, prolonged mechanical ventilation, supplemental oxygen and poor nutrition also contribute to lung fibrosis and arrested lung development in infants with BPD.11 12 BPD is one of the leading causes of morbidity and mortality in preterm infants and is associated with neurodevelopmental impairment and respiratory problems later in life.13 14
Management consists of respiratory support using oxygen supplementation, ventilation, application of surfactant and administration of systematic corticosteroids, which were widely used in the past.15–17Among systematic corticosteroids, dexamethasone with dosing ranging from 0.1 to 0.5 mg/kg/day and duration ranging from 3 to 42 days was considered as the most potent one.18 Betamethasone, a stereoisomer of dexamethasone has been administered at similar doses and was as effective as dexamethasone.19 With similar genomic effects but less potent than these two synthetic steroids, hydrocortisone was used as a natural hormone for BPD.18
Systematic corticosteroids possessed strong anti-inflammatory properties20 and improved pulmonary compliance and resistance as well as gas exchange.21 This improvement facilitated the removal of the infant from ventilation and reduced the risk of BPD but caused serious short-term and long-term adverse effects including hypertension, hyperglycaemia, intestinal perforation, impaired growth and cerebral cortical matter.22 23 Immune suppression and the associated risk of infection, together with protein catabolism were implicated in the pathogenesis of these side effects.24–26
In recent years, use of steroids for the prevention of BPD has resurfaced as a therapeutic strategy, but following the development of local (pulmonary) application strategies to prevent the adverse effects of systemic exposure.27 The modalities are (1) inhalation and (2) intratracheal instillation. Beclomethasone comes as the most commonly used inhalational steroid. Budesonide and fluticasone have been also administered as topical corticosteroids.19 Budesonide was recently evaluated as intratracheal instillation with or without surfactant as a vehicle. However, the efficacy and safety of corticosteroids administered in preterm infants via these modalities are not well established.
We conducted a systematic review to identify, critically appraise and meta-analyse data from randomised controlled trials (RCTs) comparing the pulmonary application of corticosteroids (inhaled or intratracheal instillation) with standard treatment, placebo or no intervention in preterm infants with established clinical and radiologic evidence of RDS.
Methods
We used an a priori protocol (CRD42016042985) and conducted this systematic review in accordance with the Methodological Expectations of Cochrane Intervention Reviews (MECIR) guidelines28 and reported as per the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.29
Eligibility criteria
We included RCTs evaluating preterm infants (GA <37 weeks irrespective of their birth weight) diagnosed with established RDS (using clinical, radiological or author-defined evidence). Corticosteroids were to be administered locally to the respiratory tract at any postnatal age, dose, timing or frequency compared with standard treatment (oxygen therapy and/or surfactant), placebo or no other intervention. The main a priori exclusion criteria were trials that exclusively evaluated infants with congenital anomalies or lethal cardiopulmonary disorders which are the leading cause of infant mortality30 and can distort the apparent treatment effect. We also excluded studies with cross-over, cluster or quasi-RCTs, non-randomised trials and observational studies including cohort and case-control studies. We chose RCTs since they are known as the best design to obtain unbiased estimates of treatment effect by controlling for both known and unknown confounders affecting the outcome.31
The primary efficacy outcomes were the incidence of BPD, all-cause mortality reported at the longest follow-up and the composite outcome of BPD or death. Since the criteria to define BPD still lack uniformity, we reported the composite outcome for both the earliest clinical definition of BPD as oxygen dependency at 28 days and the modified one as the need for oxygen therapy at 36 weeks corrected GA.32 To prevent misclassification in further analysis, we just focused on the second definition.
Secondary efficacy outcomes were pulmonary function tests, hospital lengths of stay and duration of mechanical ventilation. Safety outcomes were adverse effects including growth and neurodevelopmental impairment, retinopathy of prematurity, brain injury including intraventricular/periventricular haemorrhage, necrotising enterocolitis, patent ductus arteriosus (PDA), hormonal axis depression, clinical sepsis and other infections.
Search strategy and study selection
We searched MEDLINE (Ovid), EMBASE (Ovid), Global Health Conferences (Ovid), International Pharmaceutical Abstracts (Ovid) and The Cochrane Central Register of Controlled Trials (CENTRAL—Wiley) from inception to May 2016. Individualised search strategies were used for each database without any date or language limits. The MEDLINE and EMBASE search strategies are presented in online supplementary appendix 1. To identify ongoing trials, we searched ClinicalTrials.gov and the WHO’s International Clinical Trials Registry. Conference abstracts were searched in Web of Science Core Collection—Conference Proceedings. Reference lists of relevant narrative and systematic reviews and included trials were hand-searched for relevant citations. Reference management and citation screening were performed using EndNote (V.X7).33 Using a two-step process for study selection, two of three reviewers (MD, BC, GJ) independently screened title and abstract of each citation to determine whether a study met the broad inclusion criteria. The full-text of all relevant citations were retrieved for formal review. Two reviewers (MD, GJ) independently assessed the full-text reports. Conflicts were resolved by discussion between reviewers.
Supplemental material
Data extraction and management
We used a standardised, piloted data extraction form. Reviewers (MD, GJ) extracted data independently, using a standardised form, with conflicts resolved through consensus. Table 1 illustrates the baseline data extracted from each trial.
Baseline characteristics of included studies
Quality assessment
We assessed the risk of bias of the included trials using the Cochrane Risk of Bias Tool.34 35 As illustrated in online supplementary appendix 2, this tool consists of six domains and a categorisation of the overall risk of bias. We judged each separate domain as ‘low risk’, ‘unclear risk’ or ‘high risk’. If one or more individual domains were assessed as having a ‘high risk’ of bias, the trial received the same classification; similarly, for ‘unclear risk’.
Supplemental material
Data analysis
We analysed the data from included studies using RevMan (V.5.3.5).36 Meta-analyses were performed using random effects. We used the Mantel-Hanzel models for binary outcomes and inverse variance for continuous outcomes. We expressed pooled continuous data as mean difference (MD) and dichotomous data as a relative risk (RR), with 95% CIs. We quantified heterogeneity-related variability by using the I2 statistic.
Subgroup analyses
We performed subgroup analyses based on route (inhalation vs intratracheal instillation with or without a vehicle), timing of administration (early vs late), type of corticosteroid, type of comparator (surfactant vs placebo vs normal saline) and location of study (North America vs elsewhere); methodological quality (low vs unclear risk of bias) and publication status (full-text or conference proceedings vs not published).
Results
Of 873 citations, available for review, we retrieved and reviewed full-text reports for 92 potentially eligible trials. Of these, we included 12 primary trials in this systematic review (figure 1). Three studies were multicentre trials.37–39 Three trials were published in Italian,40 Mandarin41 or Korean,42 while the others were published in English. Infants were recruited between the first 4 hours and the 14th day of postnatal age. The GA of enrolled infants ranged from 26 to 34 weeks, and the birth weight ranged from 801 to 1591 g. The details of the study intervention varied among studies (table 1). The duration of intervention ranged from 1 day to 35 days with a maximum follow-up duration of 3 years. All trials administered corticosteroids for the prevention of BPD either in the first 24 hours of life37 38 43–46 or later.39 47–50 Type of corticosteroid used for intervention also varied among trials as follows: budesonide (six trials),37 41 46 47 51 52 fluticasone propionate (two trials),53 54 beclomethasone (three trials)48 54 and dexamethasone (one trial).55 In eight trials, corticosteroids were administered by inhalation,43 47 51 53–55 and in four trials,37 41 46 52 they were given to infants via the endotracheal route. Three trials37 41 46 used an animal-derived surfactant in the control group, two studies used normal saline52 55 and seven studies used placebo47 48 51 53 54 as comparators. Timing of BPD assessment differed across studies. One trial reported BPD at 28 days of age,48 four trials reported this outcome at 36 weeks of postmenstrual/postconceptional age37 38 45 46 and three trials used both timing frames for the diagnosis of BPD.39 43 50 Mortality rate was reported at 28 days of age (two trials),39 48 36 weeks of postnatal age (six trials)37–39 45 46 50 and before discharge (one trial).43 One trial was adjudicated to be at low risk of bias,51 and the others were judged to be at unclear risk of bias37 41 46 47 52–55 (see online supplementary appendix 2).
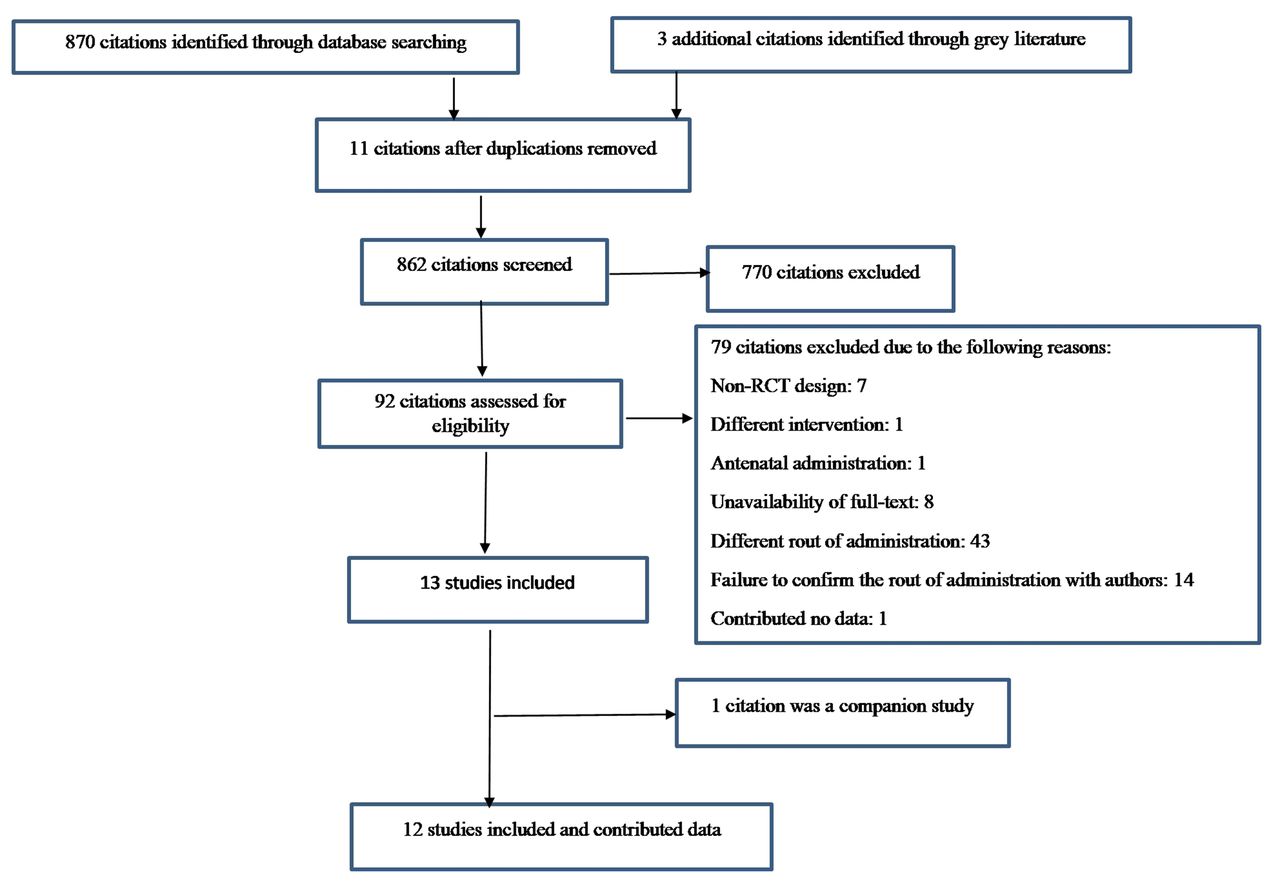
Preferred Reporting Items for Systematic Reviews and Meta-analysis flow chart depicting the selection process of included studies. RCT, randomised controlled trial.
Primary efficacy outcomes and subgroup analysis
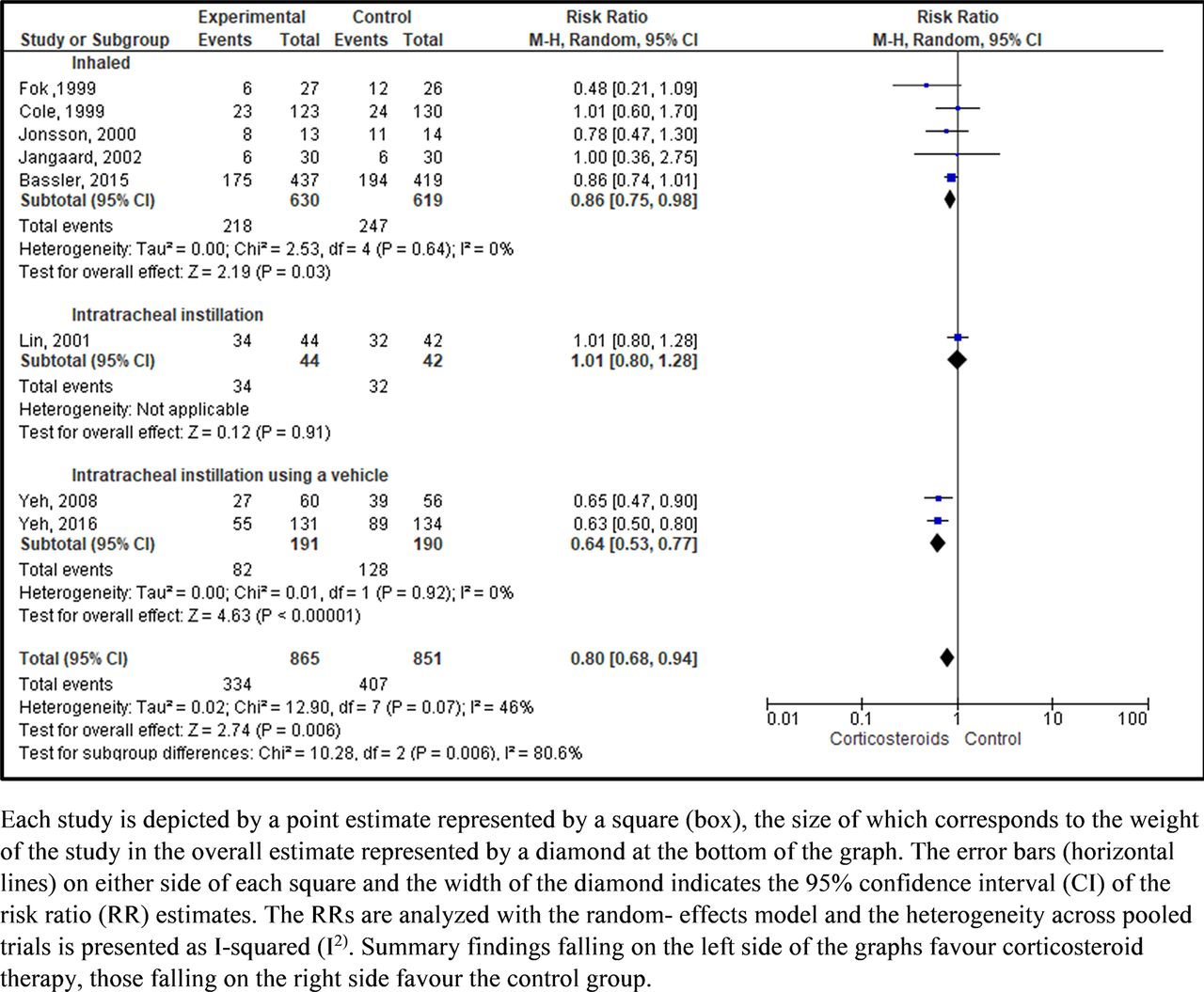
Pulmonary application of corticosteroids was associated with a significant reduction in the composite outcome of death or BPD (RR 0.85; 95% CI 0.76 to 0.96). This reduction remained significant and was greater when BPD was assessed at 36 weeks of postmenstrual GA (RR 0.80, 95% CI 0.68 to 0.94; I246%; 8 trials) compared with 28 days of age (RR 0.96, 95 % CI 0.86 to 1.07; I20%; 5 trials) (figure 2). Meta-analysis of trials which assessed BPD at 36 weeks of postmenstrual age showed greater reduction in the composite outcome when corticosteroids were administered endotracheally using surfactant as a vehicle (RR 0.64, 95% CI 0.53 to 0.77; I20%; 2 trials, 381 infants) compared with inhaled administration (RR 0.86, 95% CI 0.75 to 0.98; I20%; 5 trials, 1249 infants) (figure 3). In contrast, direct instillation of corticosteroids without surfactant in one trial increased the incidence of death or BPD by 1% (RR 1.01, 95 CI% 0.80 to 1.28; 86 infants). The pooled data from these trials also showed a significant reduction in the incidence of BPD or death in infants exposed to budesonide (RR 0.79, 95% CI 0.65 to 0.95; I262%; 5 trails; 1350 infants) compared with beclomethasone (RR 1.01, 95% CI 0.64 to 1.60; I20%; 2 trials, 313 infants) and fluticasone (RR 0.48, 95% CI 0.21 to 1.09; 1 trail, 53 infants) (figure 4).

Bronchopulmonary dysplasia or death assessed at different timing frames.

Bronchopulmonary dysplasia or death at 36 weeks of postnatal age associated with different routes of pulmonary corticosteroid therapy among included trials.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bronchopulmonary dysplasia or death at 36 weeks of postnatal age associated with different types of pulmonary corticosteroid therapy among included trials.
Pulmonary application of corticosteroids had no effect on the incidence of death from all causes at 36 weeks of postnatal age (RR 0.99; 95% CI 0.75 to 1.30; I2 18%; 6 trials; 1636 infants) (see online supplementary appendix 3). The longest follow-up for short-term mortality was 35 days with a median of 17.5 days after birth. The infants in the treatment group also had 27% reduction in the incidence of BPD at 36 weeks of postnatal age compared with the control group (RR 0.73, 95% CI 0.61 to 0.86; I2 12%; 6 trials; 1663 infants) (see online supplementary appendix 4).
Supplemental material
![[SP3.jpg]](https://fn.bmj.com/content/fetalneonatal/104/2/F137/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
Supplemental material
![[SP4.jpg]](https://fn.bmj.com/content/fetalneonatal/104/2/F137/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
Finally, the observed differences among subgroups on the timing of administration, type of corticosteroid, type of comparator, route of administration, publication status, the risk of bias and trial geography were not statistically significant (see online supplementary appendix 5).
Supplemental material
Secondary efficacy outcomes
The pooled data from trials demonstrated no evidence of significant reduction in the value of fraction of inspired oxygen (FIO2) levels,41 47 48 55 the infants’ blood PaO2 of carbon dioxide (PCO2) at latest measurement41 47 52 and the duration of mechanical ventilation48 in the treatment group compared with control group. Mean air pressure55 and PaO2 of oxygen (PO2)41 as indicators of pulmonary function and duration of hospitalisation46 were reported in single trials (see online supplementary appendix 6).
Safety outcomes
Among five studies enrolling 1320 infants, we observed a significant reduction in the risk of PDA in those treated with pulmonary corticosteroids compared with the control group (RR 0.82, 95% CI 0.74 to 0.92; I2 31%).
Additionally, pooled data from three studies37 41 48 enrolling 324 infants demonstrated a reduction in the risk of developing pneumonia in those treated with corticosteroid compared with control group (RR 0.57, 95% CI 0.35 to 0.92; I2 0%).
The pooled data from trials also did not show any significant difference in groups with respect to short-term changes in weight (MD −1.73, 95% CI −14.04 to 10,58; I2 0%),38 47 50 head circumference (MD 0.07, 95% CI −0.03 to 0.17; I2 0%)38 47 50 and height (MD −0.04, 95% CI 0.18 to 0.10; I2 41%).47 50
Using the same definition for neurodevelopmental impairment, two trials reported this outcome after a follow-up of 2–3 years37 46 indicating that the risk of developing neurodevelopmental impairment in those treated with endotracheal budesonide using surfactant as a vehicle and those in the control group receiving surfactant alone was not significantly different (n=239 infants, RR 1.01, 95% CI 0.68 to 1.52; I2 0%).
No significant difference was observed between treatment and control groups on the following adverse outcomes: retinopathy of prematurity, brain injury including intraventricular/periventricular haemorrhage, necrotising enterocolitis and sepsis (see online supplementary appendix 7). Adverse effects including intestinal perforation, periventricular leukomalacia, hyperglycaemia, hypertension, pneumothorax, hormonal axis depression, gastrointestinal bleeding, oral candidiasis and meningitis were reported by single trials without any significant RR.
Supplemental material
![[SP6.jpg]](https://fn.bmj.com/content/fetalneonatal/104/2/F137/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
Discussion
A variety of systemic reviews has addressed the use of systemic,56 57 or inhaled58–60 corticosteroids or a comparison of both routes of administration22 23 61 62 in the prevention or treatment of BPD. Due to a limited number of included studies, no firm conclusion could be obtained from these reviews. Additionally, there was a significant overlap in ages at the administration of the inhaled corticosteroids.22 23 60 63 For instance, Shah et al conducted a meta-analysis of seven trials including 492 infants that were administered inhaled steroids before the age of 2 weeks, but the primary and secondary outcome variables were only reported in five trials.63 Similarly, Onland et al reported a meta-analysis of eight trials compromising of 232 infants who were administered inhaled corticosteroids after 7 days of age compared with a control group.60 However, both meta-analyses failed to find any significant differences in the incidence of mortality and BPD in infants treated with inhaled corticosteroids compared with those who received placebo. Another meta-analysis of three trials conducted by Shah et al. comparing inhaled and systemic corticosteroids also found no difference in the incidence of mortality and BPD.22 A recently published meta-analysis by Venkatraman et al 64 showed a 43% reduction in BPD without affecting the mortality rate. This study included two trials investigating the endotracheal administration of budesonide in very low birth infants.
Our systematic review included more trials (12) representing 1935 infants and provided the evidence that pulmonary administration of corticosteroids significantly reduced the incidence of BPD and the composite outcome of death or BPD in preterm infants. The difference between routes of administration was significant, with a larger reduction when steroids were administered intratracheally using surfactant as a vehicle37 46 than inhalation.38 39 43 47 50 Even though our results are consistent with the findings of other meta-analyses57 64 65 that showed a significant decrease in the incidence of BPD and a decrease or no change in mortality, ours cannot be compared with some of them57 65 as those reviews included only trials with systemic corticosteroid therapy, which as a different route may be associated with higher rate of adverse effects.
We also found that endotracheal instillation of corticosteroids alone did not significantly affect the incidence of the composite outcome of death or BPD but adding surfactant improved the findings. Surfactant is a surface-active lipoprotein complex (phospholipoprotein) that reduces the surface tension in the lungs to enhance O2/CO2 exchange.15–17 Using surfactant as a vehicle is based on a phenomenon known as the Marangoni Effect, wherein the dragging force created by surface tension gradients between surfactant and airway liquid facilitates drug distribution to the periphery of the lungs.66 Surfactant also re-expands atelectatic areas and leads to effective deposition of corticosteroids even in collapsed areas of lungs.67
Compared with other types of corticosteroids, the lower risk of death or BPD in infants who were exposed to budesonide can be related to the corticosteroids’ effect on the synthesis of lamellar body phosphatidylcholine and increase in surfactant synthesis.68 With antiproliferative properties, corticosteroids can also affect lung fibroblasts, pulmonary vascular and bronchial smooth muscle cells. Moreover, budesonide is shown to increase the production of surfactant proteins gene transcription68 69 and surface active agents.70–72
The pulmonary administration of corticosteroids also demonstrated beneficial effects on the incidence of PDA and pneumonia with no effect on growth, neurodevelopment and short-term mortality. However, well-designed RCTs with a long-term follow-up are needed to record these outcomes at a later age.
Our analysis is unique as it added a single very large trial that includes 66% more infants than all the studies above together and considered no limitation for a) the age of the infant being studied in trials by including preterm infants from birth onwards, b) severity of the condition and c) routes of pulmonary administration of corticosteroids. Accordingly, this systematic review provides useful practical information considering the role of pulmonary corticosteroids for preterm infants at risk of BPD with a large sample size of infants (n=1935) and by considering both routes of administration, inhaled and endotracheal with or without using surfactant as a vehicle.
Additionally, this study is a comprehensive review including multiple electronic database searches, hand searching of grey literature and bibliographies of included studies and forward searching. Furthermore, in case of inadequate reporting of data or presentation of data in a different format, we could reach the authors, all responding and providing additional data. This review also provided a high quality of evidence as none of the included trials was at high risk of bias and all were free of reporting and other sources of bias. We also used a priori protocol which was prepared according to the PRISMA-P guideline of 2015.73 We conducted the review by MECIR guidelines28 and reported the results following PRISMA guidelines for systematic review and meta-analysis.29
There are limitations of this systematic review that merit discussion. First, in most trials, the duration of post-treatment assessment was short (2–14 days). Only two trials reported neurologic outcomes,37 46 and other trials failed to follow-up enrolled preterm infants. To ensure that corticosteroids have a sustained benefit, evaluating long-term adverse effects is of high importance. Second, secondary outcomes of corticosteroid therapy could not be sufficiently assessed in this review because mean air pressure and PO2 as indicators of respiratory function and duration of hospitalisation were reported by single trials; therefore, they could not be included in the meta-analysis. Finally, the included studies were published between 1992 and 2017, and significant changes in the management of preterm infants with RDS have taken place over three decades. Due to these concerns, the generalisability of the findings and our ability to make treatment recommendations regarding the application of inhaled or endotracheal corticosteroids in the current era of RDS management is limited. To address these limitations, a large RCT is needed to evaluate the risk-benefit ratio of pulmonary corticosteroid therapy. We also could not assess publication bias due to a limited number of included studies for desired outcomes.
Conclusion
Pulmonary administration of corticosteroid therapy significantly decreases the risk of BPD alone and the composite outcome of death or BPD in preterm infants with RDS. Direct intratracheal instillation of corticosteroids using surfactant as a vehicle is significantly more effective than inhaled corticosteroids to treat preterm infants with RDS. The pulmonary application of corticosteroids also has beneficial effects on pneumonia and PDA with no effect on growth, neurodevelopment and short-term mortality, which warrants further evaluation with longer follow-up.
References
Footnotes
Contributors GWt' proposed the topic. MD and M-LL designed the search strategy. MD, GWt’J and BFC reviewed the citations and extracted the data. AMA-S and RZ checked the methodology. MD analysed the data and prepared the first draft of the manuscript. All authors were involved in revising the manuscript and approved the final version.
Funding No funding was specifically obtained for this systematic review.
Competing interests MD’s salary is supported by GW’tJ’s Establishment Grant from the University of Manitoba and the Children’s Hospital Research Foundation of Manitoba. RZ is the recipient of a Canadian Institutes of Health Research (CIHR) New Investigator salary award.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Presented at This research was presented in the 33rd International Conference on Pharmacoepidemiology and Therapeutic Risk Management, Montreal, Canada, 26–30 August 2017. MD also received poster award in the 13th Annual Child Health Research Days, Winnipeg, Canada, 3–5 October 2017.
Linked Articles
- Fantoms