Article Text

Abstract
Objectives Neonatal intubation is a difficult skill to learn and teach. If an attempt is unsuccessful, the intubator and instructor often cannot explain why. This study aims to review videolaryngoscopy recordings of unsuccessful intubations and explain the reasons why attempts were not successful.
Study design This is a descriptive study examining videolaryngoscopy recordings obtained from a randomised controlled trial that evaluated if neonatal intubation success rates of inexperienced trainees were superior if they used a videolaryngoscope compared with a laryngoscope. All recorded unsuccessful intubations were included and reviewed independently by two reviewers blinded to study group. Their assessment was correlated with the intubator’s perception as reported in a postintubation questionnaire. The Cormack-Lehane classification system was used for objective assessment of laryngeal view.
Results Recordings and questionnaires from 45 unsuccessful intubations were included (15 intervention and 30 control). The most common reasons for an unsuccessful attempt were oesophageal intubation and failure to recognise the anatomy. In 36 (80%) of intubations, an intubatable view was achieved but was then either lost, not recognised or there was an apparent inability to correctly direct the endotracheal tube. Suctioning was commonly performed but rarely improved the view.
Conclusions Lack of intubation success was most commonly due to failure to recognise midline anatomical structures. Trainees need to be taught to recognise the uvula and epiglottis and use these landmarks to guide intubation. Excessive secretions are rarely a factor in elective and premedicated intubations, and routine suctioning should be discouraged. Better blade design may make it easier to direct the tube through the vocal cords.
- intubation
- neonate
- medical education
- videolarygoscopy
Statistics from Altmetric.com
What is already known on this topic?
Intubation is a difficult skill to learn and teach.
Endotracheal intubation is a mandatory skill for neonatal trainees.
Currently, if an attempt is unsuccessful, the intubator and their supervisor often do not know why.
What this study adds?
Lack of success was most commonly due to failure to recognise anatomical structures.
Excessive secretions in elective intubations are rarely a factor and routine suctioning should be discouraged.
Introduction
Endotracheal intubation is a life-saving procedure in the neonatal intensive care unit (NICU). It is a mandatory competency for general paediatric trainees by the Royal College of Paediatrics and Child Health.1 Intubation skills are difficult to acquire. Reported success rates of intubators are between 20% and 73% and inexperienced intubators have the lowest success rates.2–9 Increased reliance on non-invasive ventilation and discontinuation of routine intubation of infants born through meconium-stained liquor has led to a reduction in the number of neonates being intubated. This, coupled with increasing numbers of trainees and reduction in trainee working hours, increases the difficulty of achieving proficiency. Success rates also appear to be falling. Three recent studies report success in less than 25% of attempts.2 3 5 Endotracheal intubation is associated with a high rate of complications. In a prospective study, adverse events occurred in 39% of intubations and serious adverse events in 9%.10
Neonatal intubation is generally taught using an apprenticeship model where the trainee observes and then later attempts the procedure while supervised. One of the challenges is that the trainer is not able to share the trainee’s view during laryngoscopy. Therefore if an attempt is unsuccessful, it is often difficult for the trainer to understand why and to provide constructive feedback. Videolaryngoscopy allows the intubator and the trainer to share the view, and has been shown in a recent randomised controlled trial (RCT) to improve intubation success rates.11 Recording images also allows for review after an attempt.
The objectives of this study were to review videolaryngoscopy recordings of unsuccessful intubations and identify why the attempt failed, and also to compare this with the reasons reported by the intubators.
Methods
Settings and practice
This is a descriptive study using data obtained from an RCT evaluating videolaryngoscopy for neonatal intubation.11 The study was conducted from February 2013 to May 2014 at the Royal Women’s Hospital, Melbourne, Australia, a tertiary perinatal centre with ∼7500 births and 300 infants with birth weights less than 1500 g admitted annually to the NICU. Included intubations were those performed orally on infants without facial or airway anomalies by a paediatric trainee with less than 6 months of tertiary neonatal experience. Premedication with fentanyl, atropine and suxamethonium was used for elective intubations and the use of a stylet was routine. The attending clinician, not in the research team, decided what intubations could be performed by trainees with limited experience. The primary outcome was the first attempt intubation success rate.
Study intervention
All intubations were performed using a videolaryngoscope (LaryFlex, Acutronic, Hirzel, Switzerland). This is a modified traditional Miller laryngoscope that contains a fibreoptic cable whose tip replaces the bulb and transmits images from the blade tip to a nearby monitor. To enable recording, a MacBook Pro was connected to the videolaryngoscope and video images were recorded with VideoGlide for Mac (EchoFX, Duluth, Georgia, USA). It took a few minutes to enable recording, so if there were time constraints, this step was left out. Intubations in the delivery room were not recorded.
The trainee performed direct laryngoscopy and did not look at the video screen. Intubations were randomised to the video screen being visible to the instructor (intervention group) or covered (control group). The supervisor guided the intubations in a standardised way; this included helping to optimise the position of the infant.11 The view on the screen was similar to the direct view, differing only in being wider and magnified. A senior clinician who was not a member of the research team determined when to stop the intubation attempt, based on preset clinical criteria. Each intubation was followed by debriefing and feedback. The trainees also completed a questionnaire that included a list of reasons for unsuccessful intubation that had been compiled by the authors (JEOS, COFK, MT, PGD). The questionnaire was piloted before the RCT on neonatal trainees not participating in the trial and adjusted following their feedback. The reasons for unsuccessful attempts listed on the questionnaire used during the RCT included the following: (1) an inability to advance the laryngoscope beyond the lips, tongue or oral cavity; (2) an inability to visualise the vocal cords; (3) too many secretions or inadequate suction; (4) a poorly positioned infant; (5) the oesophagus was intubated; (6) the infant became clinically unstable and therefore the procedure was abandoned; and (7) other reasons. More than one reason could be selected if appropriate.
Analysis of videolaryngoscopy recordings
Videos of unsuccessful intubations were included in this study. As delivery room intubations were not recorded, all intubations in this study were elective and premedicated. Both intervention and control videos are included but described separately. The control videos are representative of a real-world situation. The intervention videos are presented to explore whether using this technique changed the reasons why an attempt was unsuccessful. Only the first intubation attempt was included in this study.
Two reviewers (JEOS and PL) independently reviewed all the videos blinded to study group. Before assessing the videos, the reviewers developed a list of potential reasons for failure of intubation. The agreed list included the following: (1) an inability to advance the laryngoscope beyond the oral cavity, (2) successfully advancing beyond the oral cavity but unable to achieve an intubatable view, (3) excessive secretions, (4) oesophageal intubation, (5) failure to or delay in recognising the vocal cords, (6) inability to correctly direct the ETT despite having an intubatable view and (7) successful intubation followed by accidental extubation. As the infant’s position and clinical condition could not be seen on the recordings, these were not included. The reasons did not need to be mutually exclusive. Failure to or delay in recognising the vocal cords was defined as the trainee obtaining an intubatable view but either not attempting to place the ETT or attempted placement delayed 15 s or more. Inability to direct the ETT was used to describe when an intubatable view was obtained and the operator repeatedly attempted to pass the ETT but could not direct it through the vocal cords. Excessive secretions were listed as a reason when secretions blocked the view and were not cleared by the resident. When the operator performed suction but clearly had the laryngoscope misplaced, secretions were not felt to be contributory. It was possible that more than one reason contributed to failure of the attempt. Interobserver agreement between the two reviewers was assessed. Discrepancies were resolved by discussion. The final reviewers’ decision was compared with the trainee’s perception as reported in the postintubation questionnaire.
To objectively describe the view of the infant’s airway, the reviewers also graded the best view of the infant’s larynx achieved and the view visible during the endotracheal tube insertion using the Cormack-Lehane (C-L) classification system.12 This system was described in 1984 as a way of simulating potential scenarios that trainee anaesthetists might face. Grade 1 describes a full view of the glottis being achievable. Grade 2 refers to a partial glottic view being visible. Grade 3 is when the epiglottis but not the glottic opening can be seen, and grade 4 is when neither glottis nor epiglottis is seen. This classification system for assessment of laryngeal view was used as this system was designed for beginners,13 simple to use and used commonly in paediatric research.14 For the purposes of this study, an intubatable view was defined as a C-L grade 1 or 2 view during the intubation attempt. Infants with facial or airway anomalies were excluded; therefore, it is reasonable to expect that an experienced intubator would have achieved an intubatable view in all of these infants.
Data analysis and statistics
Descriptive statistics for population characteristics are presented. Categorical variables are presented as proportions and 95% CIs, while numerical variables are presented as mean (SD) for normally distributed data or median (IQR) for skewed data. Fisher’s exact test, Student’s t-test and Mann-Whitney U test were used as appropriate. p Values of <0.05 were considered statistically significant.
Outcome for agreement between the trainee and the reviewer was nominal (yes/no agreement). Interobserver variability was determined using nominal kappa statistics with bootstrapped bias and corrected 95% CIs. Kappa values can be classified as follows: below 0=poor, 0–0.20=slight, 0.21–0.4=fair, 0.41–0.6=moderate, 0.61–0.8=substantial and 0.81–1=almost perfect. The STROBE checklist for reporting observational studies was used.
Results
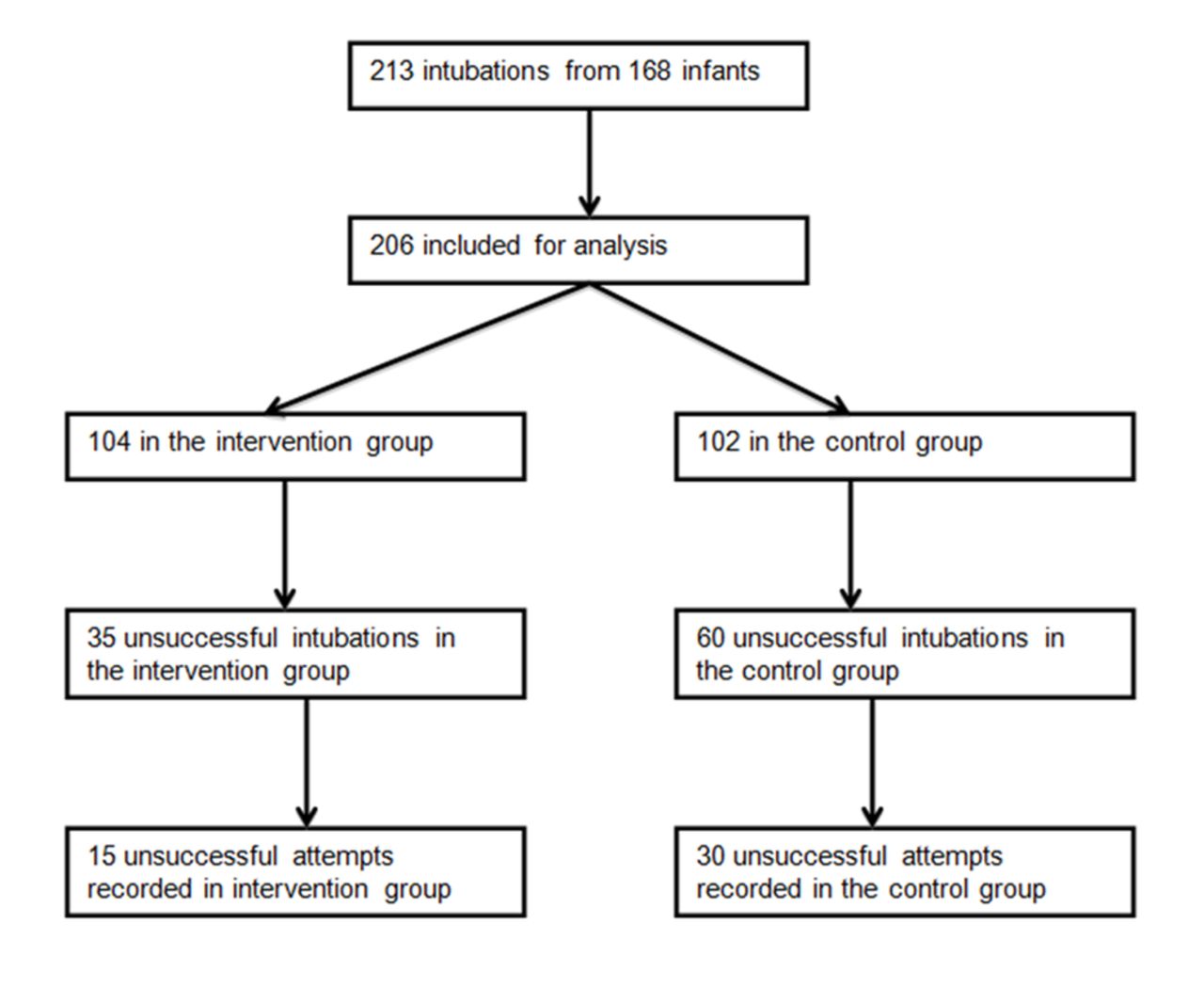
Intubations were performed by 36 trainees who performed a median of 7 each (range 2–11). Questionnaires were completed after all intubations (100% response rate). Forty-five unsuccessful intubations were recorded and included in this study: 30 control and 15 intervention (figure 1). All included intubations were premedicated and elective intubations. Baseline characteristics of infants and trainees are presented in table 1.
{kind=link}
Study flow diagram.
Baseline characteristics of the study population
The results are described in table 2, and the best view classification and classification while attempting to pass ETT are described in table 3. In the control group, an intubatable view was achieved in 23 attempts (77%). A further three (10%) achieved a view of the epiglottis but apparently did not recognise it as a landmark to help find the vocal cords. One trainee (4%) lost the view when trying to insert the ETT (see online supplementary video 1), and in another eight (35%) attempts the grade of the view obtained worsened when the trainees’ attention was directed at passing the ETT (table 3). In nine attempts (30%) the trainee had no or delayed recognition that they had a view of the larynx; in four of these attempts, there was no effort to pass the ETT, and in the other five the attempt was delayed and unsure (see online supplementary video 2). There were 14 (47%) oesophageal intubations (see online supplementary video 3); 9 of these were despite an intubatable view. In 10 (33%) attempts it was apparent that the trainee was trying to direct the ETT towards the vocal cords but was unable to direct the ETT through the cords (see online supplementary video 4). During eight (27%) attempts, the infant’s tongue was to the right of the laryngoscope blade and may have been an obstacle to inserting the ETT. However, in only three of these attempts did the trainee report that they could not direct the tube. Suctioning was performed in 11 control intubations. However in nine (82%), excessive secretions were not apparent and suctioning did not improve the view. The duration of suctioning ranged from 3 to 16 s (mean 8 s). One (3%) intubation attempt was successful but then accidentally dislodged while securing the tube.
Supplementary file 1
Supplementary file 2
Supplementary file 3
Supplementary file 4
Comparison of unsuccessful intubations factors between the control group and the intervention group
Cormack-Lehane classification system for assessment of laryngeal view
In 86% of the intervention group attempts, an intubatable view was achieved. No trainee lost the view while inserting the tube, and in two (13%) attempts the grade of the view worsened when trying to insert the tube (table 3). Inability to direct the ETT was the most commonly reported reason for attempt failure and seen in 60% of attempts. During three attempts, suction was performed; in two of these, excessive secretions were blocking the view.
In the majority of the videos, there is substantial (60%–80%) or almost perfect (>80%) inter-rater agreement between the two investigators and between the investigators and the trainees (table 4). Trainees correctly identified when they could not advance beyond the oral cavity (kappa 1.0), could not achieve an intubatable view (kappa 1.0) or were hampered by excessive secretions (kappa 1.0). Trainees were less certain when they had intubated the oesophagus (kappa 0.60 (95% CI 0.36 to 0.85)).
Inter-rater agreement
Discussion
This study describes the reasons why neonatal intubation attempts were unsuccessful. These findings can hopefully contribute to improving how intubation is taught. In order to successfully intubate, the intubator has to be able to achieve, recognise and maintain an intubatable view. The majority of the residents did achieve a view, but many of them did not recognise it or struggled to maintain it when their focus moved from laryngoscopy to inserting the ETT. There were other instances where the epiglottis was seen but the scope not advanced further to reveal the vocal cords.
The basis of successful intubation training is to establish an understanding of the anatomy of the infant’s airway. The trainee should be advised to look for midline structures like the uvula and the epiglottis and use them to identify the midline and as landmarks to direct them to the vocal cords. Having images and videos easily available to the trainee may help them better recognise the anatomy. Showing them videos of successful (see online supplementary video 5) and unsuccessful intubations may also be helpful. A small study demonstrated improved skills score and decreased intubation time with prior viewing of smartphone application demonstrating the airway anatomy and intubation procedure.15
Supplementary file 5
Interestingly, in 33% of control and 60% of intervention intubations, despite an intubatable view, the ETT could not be directed in through the vocal cords. There are many possible reasons for this, including laryngoscope blade shape or rotation and the infant’s head position. Optimising head position and blade rotation was part of the agreed proforma that the supervisors used to guide, but assessing if this was achieved was unfortunately not possible using the methodology of this study.11 There is little standardisation in laryngoscope blade design. Miller’s original description was a slightly curved flat blade 10 cm long.16 Some blades have remained true to this original description, whereas others including the one used in this study have a midline trough. Perhaps this trough was added to facilitate feeding the ETT along the blade to the vocal cords. However if the ETT is inserted along the blade, the operator is not able to visualise it passing though the cords and therefore cannot be sure they have placed it correctly. Therefore trainees are taught to feed the ETT in from the side. However in several cases in this study, trainees found the lip of the laryngoscope blade to be an obstacle.
It is common for suction to be used during an intubation attempt. In the majority of occasions where suction was used in this study, it did not lead to an improved view. Suction is time-consuming, may stimulate a vagal response, and at least in elective intubations rarely helps. A small number of intubations were successful, but the tube was dislodged during securing, emphasising the need for particular care during this part of the procedure.
We presented the results of the intervention attempts in order to explore whether having the instructor share the view would change the profile of reasons for extubation failure. A higher percentage achieved an intubatable view; a lower percentage did not recognise the view or did not maintain the view; and a higher percentage had difficulty directing the ETT and less performed suction. However oesophageal intubations were still seen as were a small number of accidental extubations.
Our study has several strengths. It provides insight into an important but underinvestigated problem. Two investigators analysed the videos independently. Both investigators were blinded to the study group while analysing the data. This study was also able to include trainees’ perceptions of events. This use of the C-L classification system gave an objective grading of laryngeal view.
This study has limitations. The sample size is small and made up of elective intubations. All intubations were carried out with one laryngoscope and therefore may yield a different result profile if a different model with a flatter blade was used. It was not possible to comment on the infant’s position or physiological stability.
Conclusion
The majority of unsuccessful intubations performed by inexperienced paediatric trainees were due to oesophageal intubation or failure to recognise the laryngeal airway or structures that can lead to it. Routine suctioning during elective intubations should be discouraged. A proportion of unsuccessful intubations were due to difficulty in directing the endotracheal tube around a laryngoscope blade with a midline trough; improvement of blade design might help in these situations.
References
Footnotes
Contributors JEOS and PL wrote the first draft of the manuscript. All authors are responsible for the reported research. All authors have participated in the concept and design; analysis and interpretation of data; and drafting or revising the manuscript. All authors have approved the manuscript as submitted.
Funding Funded by the Royal Women’s Hospital, Melbourne, Australia. COFK and MT are recipients of National Health and Medical Research Council (NHMRC) Early Career Fellowships Scholarships. PGD is a recipient of an NHMRC Practitioner Fellowship. The study was supported in part by an NHMRC Program Grant No. 384100.
Competing interests None declared.
Ethics approval The Royal Women’s Hospital research and ethics committees approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. Additional text has been added to the Funding statement.