Article Text

Abstract
Objective Upper airway distention during mask ventilation could reduce gas volumes entering the lung compared with ventilation via an endotracheal tube. Therefore, respiratory tract volumes were measured in lambs and tidal volumes were compared in preterm infants before and after intubation. Design: In seven preterm lambs, volumes of the airways (oropharynx, trachea, lungs) were assessed. In 10 preterm infants, delta pressures, tidal volumes and leak were measured during ventilation 2 min before (mask ventilation) and 2 min after intubation (endotracheal ventilation). Inflations coinciding with breaths were excluded.
Outcome measures Amount of upper airway distention in lambs and differences in inspiratory and expiratory tidal volume before and after intubation.
Results In lambs, the combined trachea and oropharynx contributed to 14 (12–21) % (median (IQR), whereas the oropharynx contributed to 9 (7–10) % of the total tidal volume measured at the mouth. In preterm infants, inspiratory (11.1 (7.9–22.6) mL/kg vs 5.8 (3.9–9.6) mL/kg (p=0.01)) and expiratory (8.3 (6.8–15.4) mL/kg vs 4.9 (3.9–9.6) mL/kg (p=0.02)) tidal volumes were significantly larger during mask ventilation compared with endotracheal ventilation. Leak was 18.7 (3.3–28.7) % before versus 0 (0–2.3) % after intubation (p<0.0001). Delta pressure was 23.7 (20.8–25.6) cm H2O before versus 24.8 (20.8–26.0) cm H2O after intubation (p>0.05). During mask ventilation, expiratory tidal volume increased from 10.0 (5.4–15.6) mL/kg to 11.3 (7.6–17.0) mL/kg (p=0.01), but remained unchanged during endotracheal ventilation.
Conclusions During neonatal mask ventilation, distention of the upper respiratory tract contributes to the tidal volumes measured and should be taken into account when targeting tidal volumes during mask ventilation.
- tidal volume
- face mask ventilation
- endotracheal ventilation
- neonate
Statistics from Altmetric.com
What is already known on this topic
-
A tidal volume range of 4–8 mL/kg is recommended for newborn ventilation. However, there is little evidence that this is safe in preterm infants.
-
Inappropriate tidal volumes given at birth increase the risk of lung and brain injury.
What this study adds
-
During positive pressure ventilation, the measured tidal volumes were significantly higher during face mask compared with endotracheal ventilation.
-
In preterm lambs, we demonstrated that pressurisation of the oropharynx and trachea can account for part of the measured tidal volumes differences.
Introduction
Many preterm infants receive positive pressure ventilation at birth administered via a face mask.1 While this ventilation is commonly evaluated based on chest excursions, this is considered a poor proxy for the tidal volumes administered.2 As inappropriate tidal volumes given at birth increase the risk of lung and brain injury,3 respiratory function monitoring in neonates is suggested by experts to minimise the likelihood of injurious ventilation.4
Although a tidal volume range of 4–8 mL/kg is currently suggested for neonatal ventilation at birth,5 there is little evidence indicating what tidal volumes are safe in preterm infants. The recommended range is based on spontaneously breathing preterm infants on continuous positive airway pressure6 and intubated infants in the neonatal intensive care unit receiving volume-guaranteed ventilation.7 ,8 However, in contrast to spontaneous breathing and endotracheal ventilation, before gas can flow into the lung during mask ventilation, the oropharynx and part of the trachea must be pressurised. As these structures have a finite compliance, pressurisation of the upper respiratory tract may cause significant distension resulting in an increase in volume. As a result, it is possible that the proportion of the tidal volume entering and ventilating the gas exchange regions of the lung could be reduced, which should be taken into account when targeting tidal volumes during mask ventilation.
We hypothesised that during face mask ventilation, pressurisation of the oropharynx and trachea forms a significant proportion of the tidal volume measured at the mouth opening in deceased newborn lambs. Upon confirming this hypothesis, we then investigated whether this may also occur in infants. To test this, we examined whether equivalent inflation pressures resulted in larger tidal volumes during face mask ventilation compared with ventilation via an endotracheal tube. This was achieved by measuring tidal volumes immediately before and after intubation of preterm infants at birth.
Methods
Lamb study
Seven preterm lambs (Border–Leicester × Merino) born by caesarean section after 123–124 days (term is ∼147 days) and ventilated for 2 h. All lambs were ventilated for at least 2 h using a tidal volume of 4–8 mL/kg before they were killed by an overdose of pentobarbitone sodium (130 mg/kg intravenous). The experiments were started immediately after the animal was killed.
The lambs’ oesophagus was occluded at the cricoid cartilage. Leak-free occlusion was tested before experiments were commenced. Lambs were ventilated non-invasively using a Neopuff T-piece resuscitator (Neopuff, Fisher & Paykel Healthcare, Auckland, New-Zealand) and a close-fitting face mask (DLC Australia, Victoria, Australia). Tidal volumes were measured using a Florian respiratory function monitor (Acutronic Medical Systems, AG, Switzerland) placed in the respiratory circuit between the face mask and the T-piece of the Neopuff. Gas flow signals were recorded using PowerLab data acquisition system (Powerlab/8SP, AD Industries, Castle Hill, Australia). Inflations were administered with constant peak inflation pressures (PIP) of 35 cm H2O and positive end expiratory pressures (PEEP) of 5 cm H2O. The following measurements were performed: (1) the tidal volume was measured during ventilation of the total lung after occlusion of the oesophagus, (2) the upper respiratory tract (oropharynx and trachea) were ventilated after occlusion of the trachea above the carina and (3) the oropharynx was ventilated after occlusion of the airway tract at the glottis.
All experimental procedures on animals were approved by the Monash University Animal Welfare Committee.
Human infant study
Infants <32 weeks of gestation were retrospectively included when (1) positive pressure ventilation was given via a face mask and (2) they were intubated in the delivery room. This data was collected as it is local guideline to measure tidal volumes during resuscitation. All infants were ventilated according to local guidelines (PIP 25 cmH2O and PEEP 5 cm H2O and at a rate of 40–60 inflations per minute) using a T-piece ventilator (Neopuff, Fisher and Paykel, Wellington, New Zealand). Infants were intubated at the discretion of the caregiver. No premedication before intubation was used. Pressure and volume were recorded using a Florian respiratory monitor (Acutronic Medical Systems, AG, Switzerland) as described previously.9 The flow sensor was placed distally between the T-piece of the Neopuff and an appropriate size face mask (Laerdal 0/0 or 0/1, Laerdal, Stavanger, Norway) or at the end of an appropriate size endotracheal tube (oral/nasal tracheal cuffless tube 2.5 or 3.0, Mallinckrodt, Covidien, Tullamore, Ireland). Infants were nasally intubated and depth of insertion was performed according to the estimated birth weight, using the ‘7-8-9 rule’,10 with the position of the tube being confirmed by chest X-ray upon arrival at the neonatal intensive-care unit.
In neonates, the gas flow signal was recorded at 200 Hz and integrated to provide inspired (Vti) and expired tidal volumes (Vte) using Spectra software (Spectra, Grove Medical Limited, Hampton, UK). Leak was calculated as the difference between inspired and expired tidal volume (leak=[((Vti−Vte)/Vti)×100]. PEEP and PIP were measured to calculate delta pressures (PIP–PEEP). Inflations during ventilation were analysed from 2 min before (mask ventilation) and until 2 min after intubation (endotracheal ventilation). Tidal volumes were analysed on a breath-by-breath basis. Spontaneous breaths and inflations where breaths coincided, were identified according to previous described patterns6 and excluded from this analysis. To assess loss of functional residual capacity after intubation, Vte of the first 10 inflations was compared with Vte of the last 10 inflations of face mask and endotracheal ventilation during the 2 min period.
Oxygen saturations (SpO2) were measured using a Masimo Radical 7 pulse oximeter (Masimo, Irvine, California, USA) with a LCNS Neo-3 sensor (Masimo) placed around the ulnar aspect of the infant's right wrist. Average fraction of inspired oxygen (FiO2) and SpO2 were compared from 2 min before intubation until 2 min after intubation. FiO2 was measured using a Teledyne oxygen analyser (Teledyne technologies, Thousand oaks, California, USA).
The local institutional review boards of the Leiden University Medical Center (Commissie Medische Ethiek, Leids Universitair Medisch Centrum) approved physiological recordings at birth in the delivery room when respiratory support was necessary for research purposes. Written parental consent was obtained before birth or, if not appropriate, as soon as possible after birth.
Statistical analysis
Data were analysed using SPSS (IBM, V.20.0.0, Chicago, Illinois, USA). Results are presented as mean (SD), median (range) or median (IQR) where appropriate. Vti and Vte were averaged for each infant and lamb to give each subject similar weight. Data were compared using a Mann–Whitney U test for non-normally distributed paired data and a related samples Friedman two way analysis of variance for paired samples.
Results
Animal data
Seven lambs were included (median (IQR) weight 3570 (3480–4040) grams). Tidal volume of the total respiratory system was 19.1 (11.8–25.9) mL/kg. The tidal volume of the combined trachea and oropharynx was 4.1 (2.0–4.9) mL/kg, which was 14 (12–21) % of the tidal volume measured during ventilation of the entire respiratory system. The tidal volume of the oropharynx only was 2.3 (1.3–2.7) mL/kg, which was 9 (7–10) % of the tidal volume measured during ventilation of the entire respiratory system. No leak occurred during this ventilation period.
Human infant data
Recordings of 206 infants were reviewed for the occurence of intubations. Seventeen infants were intubated in the delivery room. Of these, seven infants needed to be excluded: three infants were ventilated via a nasal tube and in four infants, breathing frequently occurred and coincided with almost all inflations. Thus, 10 newborn infants were included (patient characteristics are stated in table 1). The average duration of the intubation attempt in the infants was 63 (28) s. Tube positions were checked in all 10 infants upon arrival at the neonatal intensive care unit, location was considered correct and all were located in the trachea above the carina.
Patient characteristics
Inflations
In total, 1586 inflations were analysed (843 before intubation and 743 after intubation). PIP was 28.8 (25.5–32.7) cm H2O before versus 29.8 (25.0–30.8) cm H2O after intubation (ns), and PEEP was 6.0 (4.5–7.1) before versus 5.9 (4.4–8.1) after intubation (ns). Delta pressure (PIP–PEEP) was 23.7 (20.8–25.6) before versus 24.8 (20.8–26.0) cm H2O after intubation (ns). Median (IQR) leak was 18.7 (3.3–28.7) % before versus 0 (0–2.3) %) after intubation (p<0.0001).
Tidal volumes
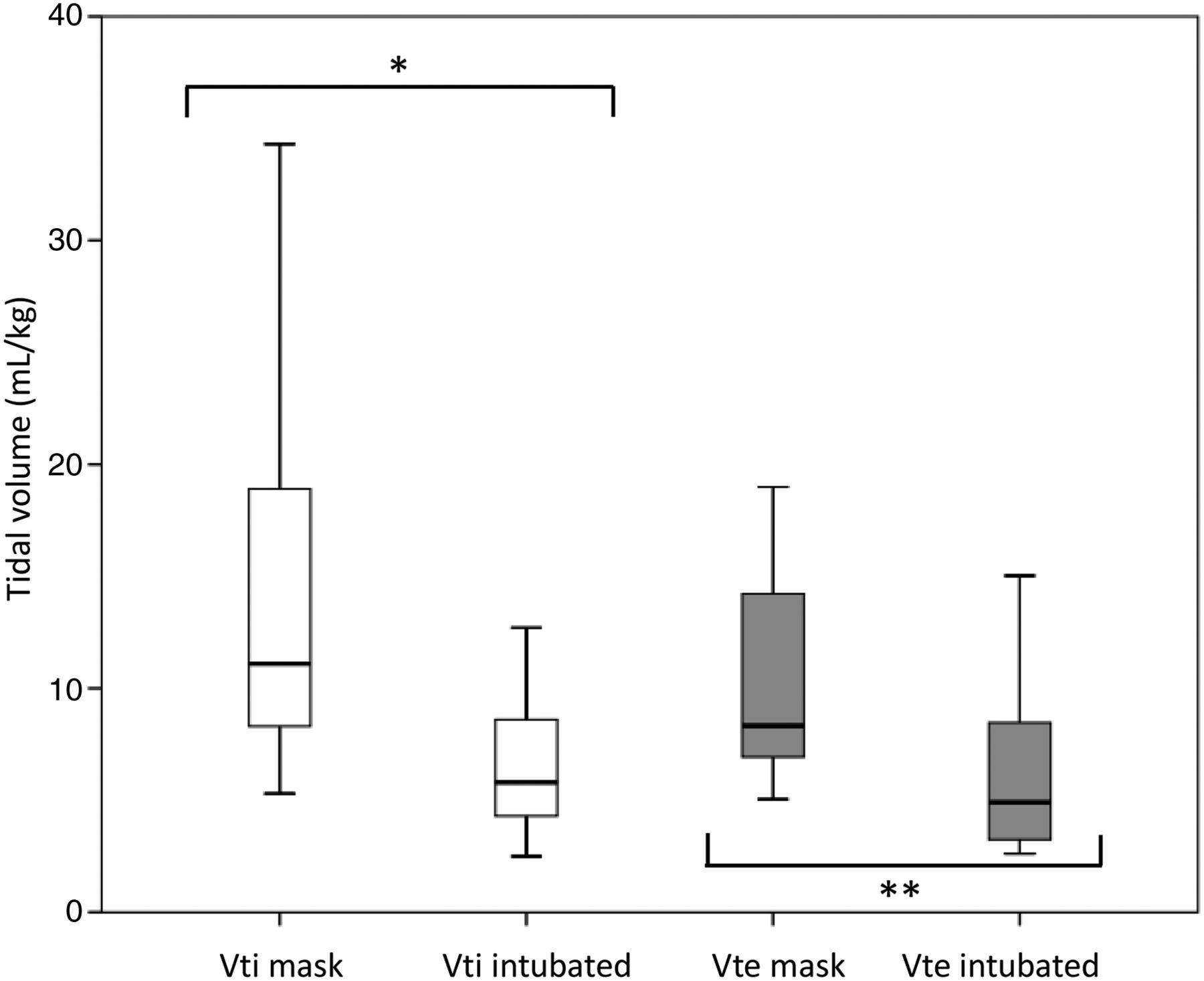
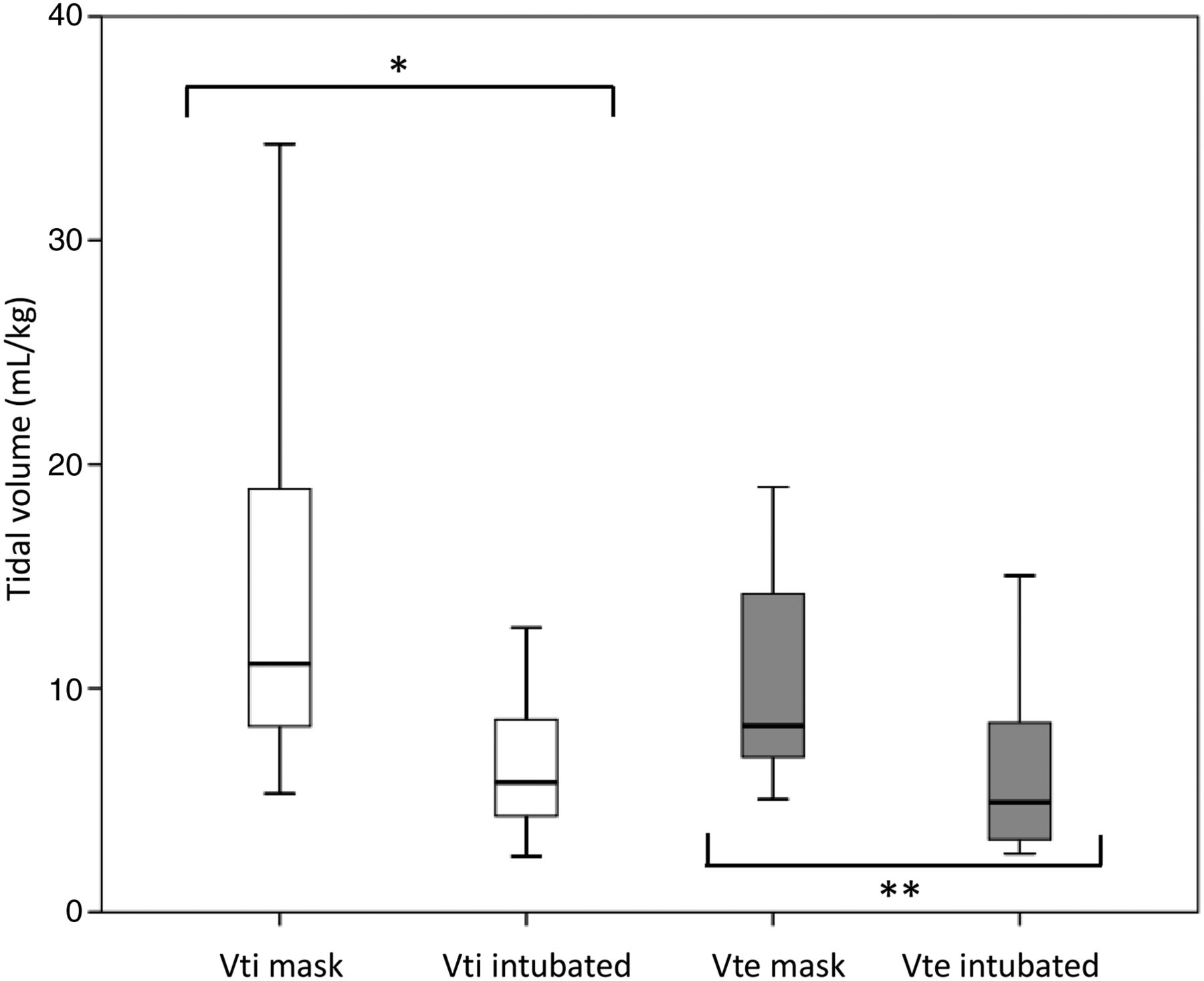
Both the Vti and Vte measured during mask ventilation were significantly higher compared with endotracheal tube ventilation (Vti; 11.1 (7.9–22.6) vs 5.8 (3.9–9.6) mL/kg (p<0.01)) and Vte; 8.3 (6.8–15.4) vs 4.9 (3.9–9.6) mL/kg (p=0.02)) (figure 1). During endotracheal ventilation, Vti and Vte were, respectively, 60 (44–81) % and 54 (29–87) % of the volumes measured during face mask ventilation.
{kind=link}
Inspiratory (Vti, white) and expiratory (Vte, grey) tidal volumes measured 2 min before and 2 min after intubation. The box plots show median values (solid black bar), IQR (margins of box) and range of data. **p<0.01, *p=0.02.
There was a small, but significant, increase in Vte measured during the first 10 inflations compared with the last 10 inflations (10.0 (5.4–15.6) mL/kg vs 11.3 (7.6–17.0) mL/kg (p<0.05)) of the 2 min mask ventilation period. However, during endotracheal ventilation, the measured Vte did not change (5.6 (3.7–13.5) mL/kg vs 5.5 (3.5–11.5) mL/kg) (ns).
Oxygen saturation and fraction of inspired oxygen
Average SpO2 was not significantly different in the 2 min before versus the 2 min after intubation (69 (21) vs 72 (23) % (ns)). Also, FiO2 was not significantly different in the 2 min before versus the 2 min after intubation (100 (93–100) % vs 100 (95–100) % (ns)).
Discussion
The tidal volumes measured in spontaneously breathing infants and ventilated intubated infants have been used to recommend the volume ranges that should be used during mask ventilation of preterm infants at birth. To our knowledge, differences in the delivered tidal volumes during mask and endotracheal ventilation have not previously been investigated. We observed that, during positive pressure ventilation, the measured tidal volumes were significantly higher during face mask compared with endotracheal ventilation, despite the delta pressure remaining very similar. In ventilated newborn lambs, we demonstrated that pressurisation of the oropharynx and trachea can account for part of the measured tidal volumes differences between face mask and endotracheal tube ventilation. Thus, it is likely that distention of the upper respiratory tract partly explains the observed differences in tidal volumes. We speculate that inadequate gas exchange could occur during mask ventilation when this extra volume is not taken into account.
During face mask ventilation, the entire respiratory system pressurises, such that by end inflation, pressures should be equal at all points in the respiratory tree, including the upper airway above the glottis. In newborn infants, particularly preterm infants, the trachea, pharynx and larynx contain little cartilage and are therefore more compliant compared with the adult upper respiratory tract.11 As such pressurisation of the upper respiratory tract will cause distention and potentially increase the risk of damage and inflammation.12 ,13 Also as the oral cavity is compliant, application of an inflating pressure should cause distention of the upper respiratory tract as it pressurises. Part of the higher expiratory volume we observed during mask ventilation is probably due to deflation of the upper respiratory tract as it depressurises during expiration.
In lambs compared with infants, a relatively smaller amount of volume was measured during ventilation of the upper respiratory tract (14% vs 65%). This could be explained by differences in anatomy and upper airway compliances between preterm lambs and infants, which determine differences in upper airway distention. Also, it is possible that during mask ventilation of infants, a large amount of air enters the oesophagus and stomach. To avoid this problem, in the lambs, we obstructed the oesophagus, but this prevented us from calculating the relative contribution of flow in the trachea and oesophagus to the measured tidal volumes. However, as it is commonly observed that the abdomen becomes distended during incorrect ventilation, it could be that air enters the stomach and is returned during expiration. However, it is unlikely that this significantly contributes to Vte.
Other phenomena, besides distention of upper airways and trachea, could have influenced the measured differences in volumes during mask and endotracheal ventilation. During the intubation procedure, a loss in functional residual capacity could have occurred leading to a decrease in compliance. If this did occur, we then would have expected an increase in tidal volumes in the 2 min of ventilation after intubation, but these remained similar. Additionally, there were no significant differences in SpO2 and FiO2 levels before, during and after intubation, making a loss in functional residual capacity unlikely. Leak could have influenced the volumes measured, but we observed larger leak during mask than endotracheal ventilation and, thus, this does not explain the smaller volumes during endotracheal ventilation. Finally, distention of the mask during inflations could have influenced tidal volume measurement,14 but it was reported that the contribution of mask distention to tidal volumes is limited.15
The current recommended range of tidal volumes (4–8 mL/kg)5 is based on measurements performed in spontaneously breathing infants shortly after birth6 and intubated preterm infants. However, during inspiration, a subatmospheric pressure in the lungs and surrounding tissues is created and the transpulmonary pressure gradient causes air to enter the lung. The upper airway and trachea are not pressurised and less volume is needed to aerate the distal airways.16 During endotracheal ventilation, smaller amounts of tidal volumes are measured (3.8 (2.8–4.7) mL/kg)8 and recommended (4–5 mL/kg).7 However, during endotracheal ventilation the oropharynx and trachea are largely bypassed and the majority of the measured volume is volume directed into the lungs.
We speculate that, to achieve adequate ventilation, larger tidal volumes are needed during ventilation procedures that pressurise the upper airway to nullify the effect of upper airway distention. It is possible that when the current recommended tidal volumes are used during face mask ventilation, ventilation is mainly restricted to the upper airway and trachea which limits penetration of air into the distal airways. Indeed, this could explain why the SpO2 remained low, and a high FiO2 was needed during mask ventilation in these infants, despite them receiving apparently large tidal volumes. Further studies are needed before a range of larger tidal volumes can be recommended, especially when considering the fact that distention of the trachea could cause injury in preterm infants.12 ,13
The limited number of intubations in the delivery room recorded (8% of all recordings) made it difficult to perform a large study. Currently, a multicentre trial is in progress, examining whether a monitoring will increase the proportion of tidal volumes within a predefined ‘safe range’ of 4–8 mL/kg during ventilation of very preterm infants (<29 weeks of gestation) in the delivery room (NTR 4104). This trial could provide more data concerning the differences in tidal volumes given during face mask and endotracheal ventilation.
Conclusion
Vte was significantly larger during face mask compared with endotracheal ventilation. This is likely to be caused by distention of the upper respiratory tract during face mask ventilation as shown in a preterm lamb model. Our study suggests that the distention of the upper respiratory tract could be taken into account when targeting tidal volumes during mask ventilation. The observed range in tidal volume in spontaneously breathing preterm infants on continuous positive airway pressure should probably not be extrapolated to infants needing mask ventilation, but further studies are warranted to find the appropriate target range.
References
Footnotes
-
Contributors JJvV wrote the protocol, collected and analysed the data and drafted the manuscript. SBH and MLS helped with the animal experiment, helped with writing the manuscript and approved the final manuscript. VK analysed the data and approved the manuscript. ABtP conceived the protocol, helped with collection of the human data, helped with writing of the manuscript and approved the manuscript.
-
Funding This work was supported by the Netherlands Organisation for Health Research and Development (ZonMw) grant number 91612027 for ABtP, Australian National Health and Medical Research Council and the Victorian Government's Operational Infrastructure Support Program for SBH and a Willem-Alexander Children's Foundation scholarship for JJvV.
-
Competing interests None.
-
Ethics approval Commissie Medische Ethiek, LUMC.
-
Provenance and peer review Not commissioned; externally peer reviewed.