Article Text

Abstract
Objective To evaluate whether time to pregnancy (TTP) is associated with neurological condition of 2-year-old children born to subfertile parents.
Design Data collected in a prospective, assessor-blinded follow-up study were used for cross-sectional analyses.
Patients Participants were the singletons of the Groningen assisted reproductive technique cohort study: all children were born to subfertile couples (n=209). The active waiting TTP of the couples obtained from fertility charts was recorded in years and months, and was converted to decimal years.
Main outcome measure The presence of minor neurological dysfunction (MND), assessed with the Hempel examination.
Results MND was present in 16 (7.7%) children. TTP of children with MND (median 4.1, range 1.6–13.2) was significantly longer than that of children without MND (median 2.8, range 0.1–13.3; Mann-Whitney U test p=0.014). Logistic regression analysis on the contribution of TTP to MND resulted in a crude OR of 1.27 (95% CI 1.06 to 1.54). After correction for gestational age, parental age and parental level of education, the association remained statistically significant: OR=1.30 (95% CI 1.05 to 1.61).
Conclusions Increased TTP was associated with suboptimal neurological development in 2-year-old children. This suggests that subfertility and its determinants are involved in the genesis of neurodevelopmental problems.
- Time To Pregnancy
- Subfertility
- Neurological Development
- Minor Neurological Dysfunction
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
What is already known on this topic
-
Time to pregnancy (TTP) may be used as a proxy for the severity of subfertility.
-
Other studies demonstrated that increased TTP is associated with more caesarean sections, pregnancy-induced hypertension, preterm birth, low birth weight, perinatal deaths and birth defects.
What this study adds
-
The present study showed an association between increased TTP and minor neurological dysfunction.
-
This association implies that factors associated with subfertility may have a negative effect on neurodevelopment.
-
The study contributes to the increasing body of evidence suggesting that subfertility per se, rather than fertility treatment, is associated with adverse outcomes.
Introduction
It is well established that children conceived with assisted reproductive techniques (ARTs), like in vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI), are at increased risk for preterm birth and low birth weight,1 conditions associated with developmental problems. Previously, we reported that neurological condition at 2 years was not affected by IVF/ICSI, that is, it was not affected by ovarian hyperstimulation nor by the in vitro procedure.2 An increasing body of evidence suggests that subfertility per se, rather than fertility treatment, is associated with adverse outcomes.3 ,4
In order to evaluate the effect of subfertility, time to pregnancy (TTP) may be used. The notion that TTP can be used as a proxy for the severity of subfertility is based on models that have shown that TTP is an important predictor of the chance of pregnancy in subfertile couples.5 ,6 About 10–20% of couples are subfertile: they fail to achieve a successful pregnancy after 12 months or more of appropriate, timed, unprotected intercourse.7 Other studies demonstrated that increased TTP is associated with more caesarean sections, pregnancy-induced hypertension, preterm birth, perinatal death and birth defects.8–13 Zhu et al,14 demonstrated that increasing TTP is correlated with a modest delay in psychomotor development in 18-month-old children. However, the association between prolonged TTP and detailed neurological outcome is not known. Therefore, the aim of this study is to evaluate the association between TTP and neurological status of 2-year-old children.
Methods
This study is part of the Groningen ART cohort study, a prospective assessor-blinded longitudinal study that focuses on developmental outcome of children born following IVF and ICSI. Two hundred and nine singletons were included in the analyses: 66 children born after controlled ovarian hyperstimulation-IVF/ICSI, 56 born after modified natural cycle-IVF/ICSI and 87 children born naturally to subfertile couples. As group status did not affect neurological condition at 2 years,2 we pooled the groups to form a set of 209 singletons born to subfertile couples.
Information on TTP was obtained from fertility charts and is recorded in years and months. Subsequently, TTP was converted into decimal years. TTP was defined as the time between the active child wish (ie, the start of timed unprotected intercourse) of the couple and conception. Note that in case of miscarriage, TTP had a new onset and ended at conception of the child included in the present study. This explains why subfertile couples may have a TTP of <1 year.
Around the time of the second birthday of children, neurological condition was assessed using the neurological examination according to Hempel.15 In the Hempel assessment, five domains of function are assessed as typical or deviant: fine motor function, gross motor function, posture and muscle tone, reflexes and visuomotor function. Children were classified as neurologically normal, simple minor neurological dysfunction (MND) or complex MND.16 Children are classified as neurologically normal if no domains are deviant or only the domain of reflexes. Simple MND implies the presence of one deviant domain (except reflexes) and it indicates a suboptimal, yet normal form of brain function. Complex MND implies the presence of multiple deviant domains and it represents the clinically relevant form of MND.
Details on the inclusion period and materials and methods have been reported previously.2 ,17 Parents gave written informed consent for participation of their child in the study. The study design was approved by the ethics committee of the University Medical Center Groningen.
Statistical analysis
First, we reported background characteristics of the Groningen ART cohort in a descriptive table. Second, the Mann-Whitney U test was performed to evaluate differences in TTP between children with or without MND. Third, multiple logistic regression analyses were used to study the effect of TTP on the occurrence of MND (either simple or complex MND) while correcting for gestational age in weeks, parental age in years and parental level of education (high or not, used as an indicator of socioeconomic status). Fourth, we repeated the multiple logistic regression analysis to evaluate the effect of TTP on complex MND alone, that is, on the clinically relevant form of MND. We used Predictive Analytics SoftWare V.18.0 to analyse the data. Probability values of <0.05 were considered statistically significant.
Results
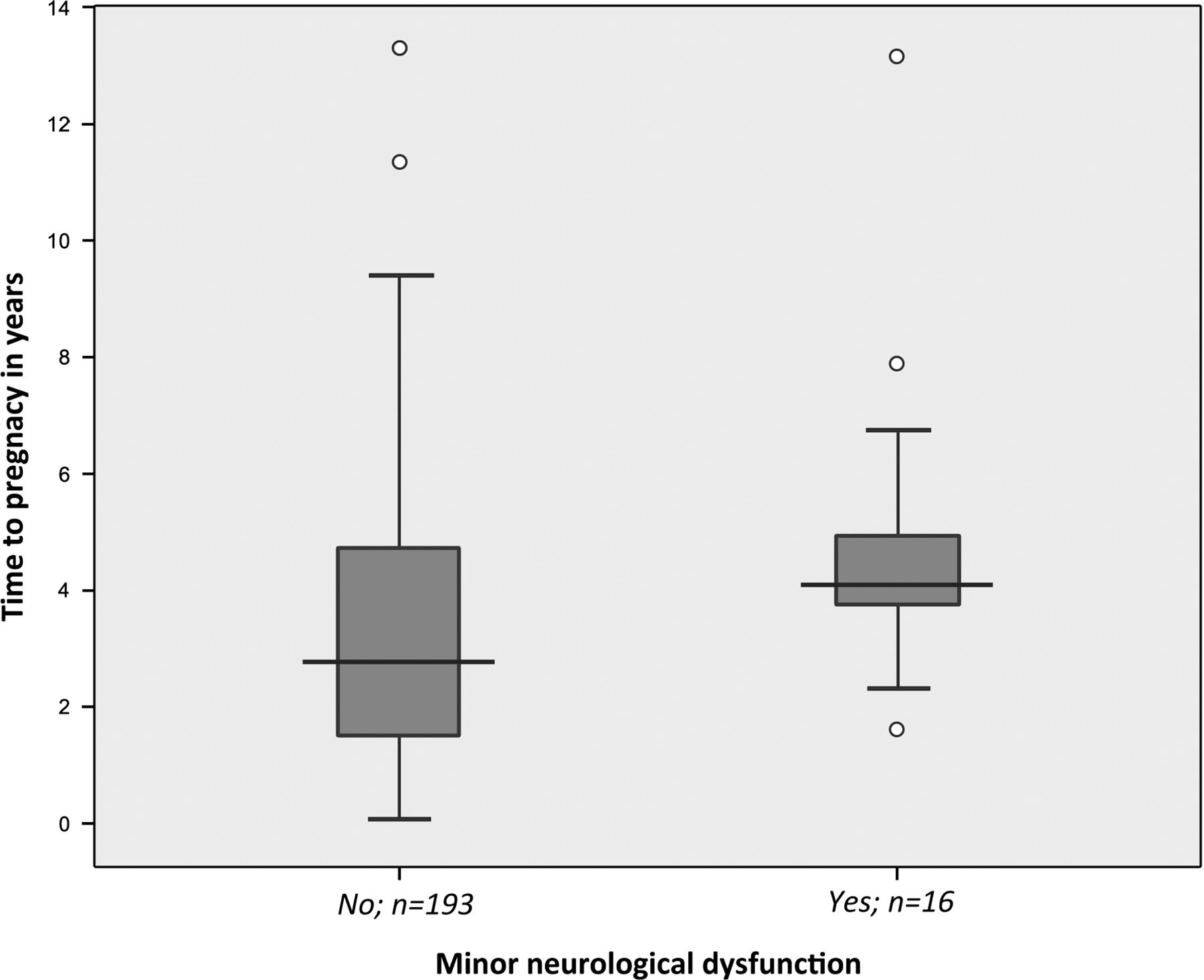
Table 1 shows the background characteristics of the children assessed (n=209). MND was present in 16 (7.7%) children: simple MND occurred in 10 children and complex MND in six children. TTP pregnancy showed a skewed distribution, median (range): 3.0 (0.1–13.3) years. TTP of children with MND (median 4.1, range 1.6–13.2) was significantly longer than that of children without MND (median 2.8, range 0.1–13.3; Mann Whitney U test p=0.014, see figure 1). Logistic regression of the contribution of TTP in years to the presence of MND (either simple or complex MND) resulted in a crude OR of 1.27 (95% CI 1.06 to 1.54, p=0.012). After correction for gestational age, parental age and parental level of education, the association remained statistically significant: adjusted OR=1.30 (95% CI 1.05 to 1.61, p=0.018). Logistic regression of the contribution of TTP in years to complex MND resulted in similar associations: crude OR=1.38 (95% CI 1.07 to 1.77, p=0.014), adjusted OR=2.29 (95% CI 1.03 to 5.09, p=0.041).
Infant, gestational, birth and parental characteristics of the singletons participating in the Groningen ART cohort study

{kind=link}
Time to pregnancy in neurologically normal children and in children with minor neurological dysfunction. Horizontal bars indicate median values, boxes IQRs, vertical lines full ranges and small circles extreme values.
The association between TTP and MND was mainly brought about by deviancies in the domain posture and muscle tone (n=7): crude OR=1.36 (95% CI 1.07 to 1.74, p=0.012). After correction for gestational age, parental age and parental level of education, this association lost statistical significance: adjusted OR=1.31 (95% CI 0.97 to 1.79, p=0.081). The other domains did not show a statistically significant association with TTP.
Discussion
TTP was positively associated with MND, including the clinically relevant form complex MND. This finding is in line with the study of Zhu et al,14 who demonstrated that increasing TTP is correlated with a modest delay in psychomotor development in 18-month-old children. A major strength of the present study is the application of sensitive and age-specific methods to assess neurological condition. In addition, attrition was minimal (3%), and selection bias was reduced as couples were recruited prospectively during the third trimester of pregnancy. Note that we were able to pool the three original study groups to form one subfertile group as group status did not affect neurological outcome. In this way, we could increase the power of the study to detect an association between TTP and MND. We checked whether additional correction for group status in the multiple analyses altered the results; it did not (data not shown). A limitation of the study is that twins were not included. This means that the results cannot be generalised to children born after multiple gestation. Furthermore, it should be noted that only six children had complex MND, which means that caution is deserved in the interpretation of the association between TTP and complex MND. In conclusion, the present data suggest that increased TTP is associated with suboptimal neurological development. This implies that factors associated with subfertility may play a role in the genesis of neurodevelopmental problems. Further exploration of the associations between subfertility and health outcome in offspring is necessary for the correct counselling of subfertile couples.
Acknowledgments
We thank participating parents and children for their cooperation and enthusiasm.
References
Footnotes
-
Contributors MH-A, MJH and AFB initiated the study. KJM collected the data. PS created the data file. JS, PS, MH-A and MLH interpreted the data. JS and MLH analysed the data. JS and MH-A drafted the report. All authors commented on drafts. All authors have seen and approved the final version. The corresponding author had full access to the data and is responsible for the overall content as guarantor.
-
Funding The study was financially supported by the University Medical Center Groningen, Groningen, The Netherlands, Grant number: 754510, the Postgraduate School Behavioural and Cognitive Neurosciences and the Cornelia Foundation. The sponsors of the study had no role in study design, data collection, data analysis, data interpretation or writing of the report.
-
Competing interests None.
-
Ethics approval The study design was approved by the ethics committee of the University Medical Center Groningen.
-
Provenance and peer review Not commissioned; externally peer reviewed.