Article Text

Abstract
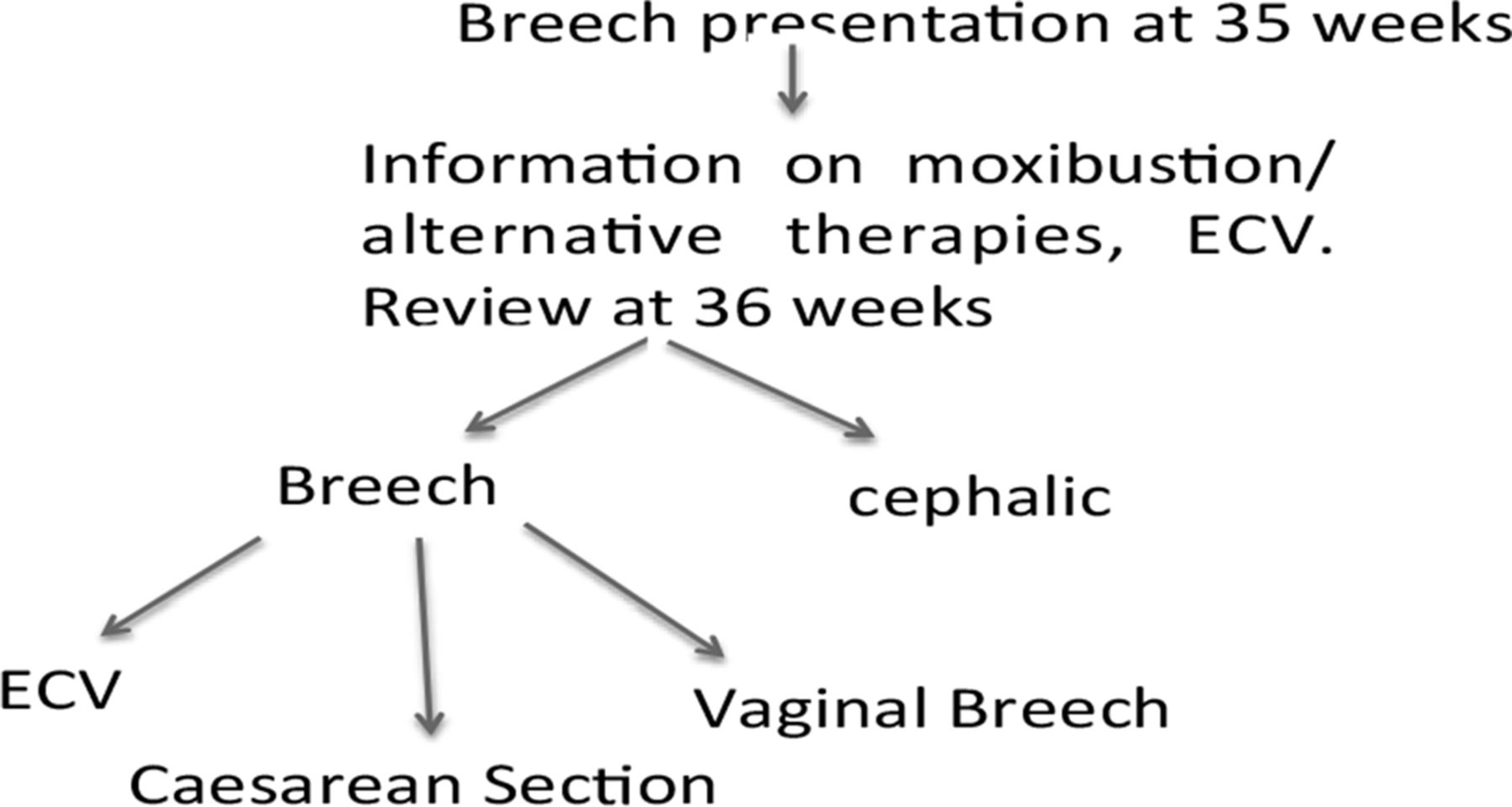
Since the Term breech trial, elective caesarean section (CS) rather than vaginal delivery has become standard practice for breech presentation. External cephalic version (ECV), manual rotation of the fetus from a breech to a cephalic position, is an alternative to a CS1 and is recommended by the Royal College of Obstetricians and Gynaecologists. Anxieties about procedural pain and concerns of risks to the fetus are major reasons women decline ECV.2,3 In 2011, 3.8% (n = 190) of babies were breech in our hospital and only 16.3% (n = 31) of these women opted for ECV after seeing various health professionals. Different obstetricians had an overall success rate of 25.8% performing ECV. A dedicated breech service led by a specialist midwife and an obstetrician was developed in 2013 (Figure 1). Over the subsequent six-months, 83 women were referred to the service. Sixty women were confirmed breech at their first visit and 50 persisted as breech at their second visit. Thirty-nine women (78%) agreed to an ECV performed between 36 and 37 weeks and the ECV success rate improved to 48.6% (p < 0.05 vs pre-service using Chi-square test). Reasons for the improved uptake and success of ECV include better communication, the offer of analgesia (remifentanil) and a single operator. 83.3% of the women who had a successful ECV subsequently achieved a vaginal delivery.

{kind=link}
Breech pathway
References
-
Sullivan EA, Moran K, Chapman M. Term breech singletons and caesarean section: a population study, Australia 1991-2005. Aust N Z J Obstet Gynaecol 2009;49:456–60
-
Rosman AN, Vlemmix F, Fleuren MAH, et al. Patients’ and professionals’ barriers and facilitators to external cephalic version for breech presentation at term, a qualitative analysis in the Netherlands. Midwifery May 13 2013; doi: 10.1016/j.midw.2013.03.013
-
Vlemmix F, Kuitert M, Bais J, et al. Patient’s willingness to opt for external cephalic version. J Psychosom Obstet Gynaecol 2013;34:15–21